
Abstract
Background:
Behavioral alerts (BAs) are electronic health record communication tools used to notify clinicians and staff about patient behavioral incidents. Despite their widespread presence, limited research exists on the content and use of BAs.
Methods:
This study took place in a large, urban, academic general internal medicine practice. Demographics of patients with BAs were compared with all patients at the practice (N = 27,023). Only patients with active BAs (N = 518) were included in the qualitative analysis. Themes were generated through open and axial coding of BAs’ free-text and thematic analysis to describe the content of BAs.
Results:
A total of 518 patients in the practice had BAs (1.9%). Compared with the general practice population, patients with BAs were more likely to be Black (23% vs. 8.5%), have public insurance (77.8% vs. 41.9%), and have a psychiatric (62.5% vs. 30.7%) or substance use-related (36.1% vs. 5.8%) diagnosis. We identified six BA themes: criminalization (behavior described as criminal or necessitating law enforcement), implied overuse (exploitation of medical resources with recommendation for limitation), advocacy (author offers support and defense), coordinating care (logistic details), venting (expression of negativity without a plan), and warning (communication of risk).
Discussion:
The wide-ranging content of BAs demonstrates their varied, unstandardized use. The unregulated use of BAs should be reexamined and restructured to avoid negatively impacting patients, particularly given their disproportionate use for historically marginalized populations, including patients who are Black, have public insurance, and those with psychiatric or substance use-related diagnoses.
Introduction
Electronic health record (EHR) behavioral alerts (BAs) are communication tools intended to notify providers about historical patient behaviors. Created in response to violent incidents at the Portland, Oregon Veterans Affairs hospital in 1983, early BAs served as a warning of a patient’s potential for violence and a directive for a safety intervention. 1 Today, multiple EHRs offer BAs as a built-in function. Despite their omnipresence, limited research exists on BA content, use, and impact. The Occupational Safety and Health Administration defines workplace violence events and provides broad guidance on promptly communicating a potential threat in the patient’s chart; many institutions operationalize this legal requirement by using BAs, but the specifics, such as how to implement and use BAs, what information to include, and for how long, are left undefined. 2
Prior surveys and focus groups note that clinicians and administrators report authoring BAs in response to perceived patient risk for aggression, weapon possession, “drug-seeking behavior,” cognitive impairment, unauthorized leaving or trespassing, and attempted self-harm.1,3–6 Health care staff reported requesting security to stand by and act with more vigilance around patients who have BAs in their chart.1,3,5 While the initial goal of BAs was to provide staff direction and time to implement a safety plan, 1 and BAs do promote feelings of safety among nurses,7,8 these alerts have not appeared to meaningfully reduce rates of violence in clinical settings.1,9–13 Furthermore, there is emerging evidence that BAs may be harmful. 14 Interviewed medical staff expressed concerns that BAs promote patient stigmatization,8,15 limit patient care,8,13,15 criminalize patients’ disorders of mental health, 16 and negatively impact physician–patient relationships. 12 A retrospective cohort study across multiple emergency rooms recently found that the presence of a BA was also associated with higher rates of patient-directed discharge, elopement-style discharge, and leaving without being seen. 17
Given the lack of clear guidelines for creation and use of BAs, they are at high risk for biased application. Patients with BAs are more likely to identify as Black and male,17,18 have Medicaid insurance, 18 and have a psychiatric or substance use-related diagnosis.1,17 Bias may also amplify the harmful effects of BAs, as Black patients with BAs experienced longer wait times to see, yet shorter time with, emergency room providers and received less lab or imaging tests than White patients with BAs. 18
Despite the prominence, semipermanence, and questionable efficacy of BAs, to our knowledge, no qualitative studies have been conducted to evaluate the content of active BAs in clinical practice. The objective of this qualitative study was to investigate the content and purpose of BAs in a large, urban, academic primary care practice through thematic analysis.
Methods
Three researchers (Z.K., I.K., M.E.G.) conducted this study: two attending physician-educators (Z.K., I.K.) and an attending physician-scientist trained in qualitative methods (M.E.G.). All are general internists in the University of California, San Francisco (UCSF) Health’s largest primary care practice, which serves ∼27,000 diverse patients, 40% of whom are publicly insured (government-funded) and 60% privately insured (self-pay or employer-based). In this qualitative analysis, we included all patients in this practice who had at least one active BA in 2022, regardless of where the BA was placed (i.e., in the emergency department [ED], while hospitalized, in a subspecialty clinic) or by whom the BA was authored. There were no exclusion criteria.
Since 2012, UCSF’s EHR (Epic Systems Corp) has displayed BAs as a yellow flag. BAs include an EHR-generated title and unstructured free text (Fig. 1); an EHR user’s security class determines the type of flag they can activate or resolve. For example, all UCSF EHR users may activate a “General” flag, while only ED social workers and security members may activate “History of Violence” flags. At the time of data analysis, BAs have no built-in expiration date and remain active until an EHR user choses to deactivate (resolve) the alert. We included all active BAs, regardless of title, that described or referenced a patient’s—or the provider’s perception of the patient’s—actions and behaviors; we did not analyze resolved BAs.
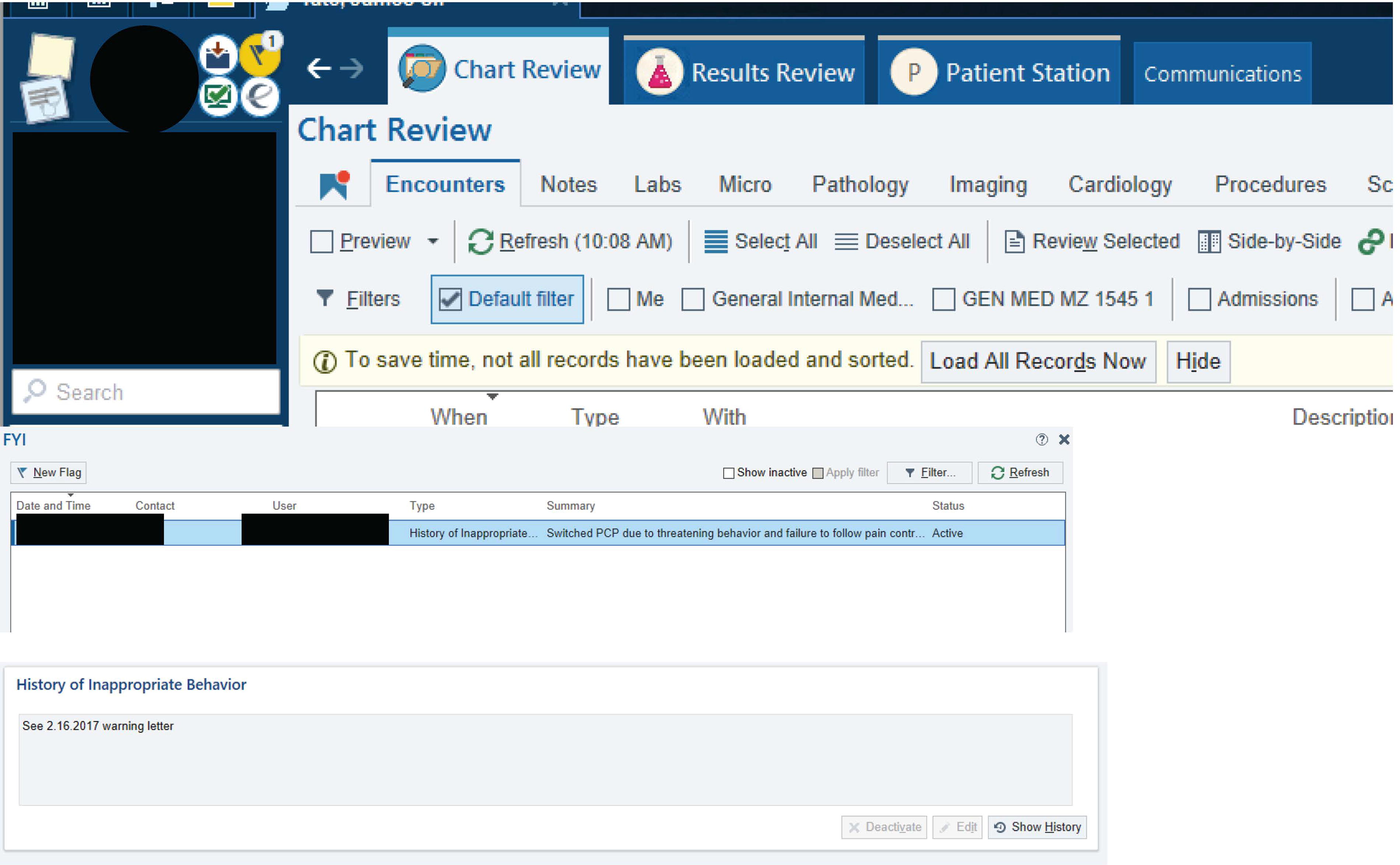
BA in the EHR. This figure shows the yellow flag in the upper-left hand corner of the patient’s chart that signifies a BA. Once the yellow flag is clicked on, a list of BAs appears. An EHR user can click on each BA to display its full title and text. BA, behavioral alert; EHR, electronic health record.
We explored the content of BAs and identified naturally occurring themes (inductive approach) through thematic analysis, 19 using Microsoft Word and Excel. Each researcher independently reviewed an initial subset of BAs using an open-coding approach; through iterative discussion, we identified consensus codes and created a joint codebook. Each researcher coded the remaining BAs using the joint codebook, revising the codebook over time through discussion. One researcher (Z.K.) then combined codes into a list of consensus codes for each BA, discussing iteratively with the research team. We identified themes to describe the perceived intention of the BA authors through axial coding 20 of consensus codes for each BA; we reconciled overlaps in themes through discussion.
To describe our sample demographics, we examined patient self-identified gender and race/ethnicity, insurance type, preferred language (classified as English or non-English), and presence of a psychiatric and/or substance use-related diagnosis [defined by International Classification of Diseases, tenth revision (ICD-10) codes]. Administrators obtain self-identified demographics from all new patients at the first visit and the patient’s treating clinician selects ICD-10 codes at the visit’s conclusion; this information is recorded in the EHR. Patients with more than one BA were counted once in the demographic analysis. We compared demographic variables for patients with BAs with aggregated practice demographics using chi-square tests for gender, insurance type, race/ethnicity, and medical diagnoses and Fischer’s exact test for preferred language.
Our qualitative analysis followed the COREQ (COnsolidating criteria for REporting Qualitative research) guidelines. 21 The UCSF Institutional Review Board approved this study for expedited review.
Results
Out of 27,023 patients, 518 (1.9%) had a total of 619 active BAs. Compared with the general practice, patients with BAs were more likely to be Black (23% vs. 8.5%), have public insurance (77.8% vs. 41.9%), and have a psychiatric (62.5% vs. 30.7%) or substance use-related (36.1% vs. 5.8%) diagnosis (Table 1). Patient gender and preferred language did not statistically differ between those with BAs and the general practice.
Demographics of Patients with BAs
All p-values calculated using chi-square test unless otherwise indicated.
p Value calculated using Fischer’s exact test.
BA, behavioral alert.
Medical, Medicaid in California; Medicare Advantage, Medicare plan through private insurance company.
The 619 BAs were authored by 53 administrative staff members, such as front desk staff or security (286 BAs; 46.2%), 78 physicians (133 BAs; 21.4%), and 9 social workers (28 BAs; 4.5%). We could not identify authorship for 123 BAs (19.8%): 42 BAs (6.8%) contained a blank author field, and in 81 BAs (13.1%), the author’s role could not be confirmed in the UCSF directory or in an online search.
The 31 codes (Supplementary Tables S1 and S2) reflected 6 themes (criminalization, implied overuse, advocacy, coordinating care, venting, and warning).
Criminalization
Many BAs described a patient’s behavior as criminal or necessitating security presence. By invoking the need for law enforcement, the patients’ actions were presented as unlawful and dangerous.
“Patient has a hx [history] of being verbally abusive, sexually inappropriate and racist towards staff. Set firm limits on behavior. File charges on any criminal behavior.”
This criminalizing language was repeated verbatim in many BAs, suggesting a reliance on canned phrasing. Often, BA authors did not clearly identify specific behaviors that necessitated security or law enforcement presence nor reference an expiration date or request for reassessment.
“I’ve triaged him before and he had an almost identical presentation. Protocol should mention he has a low threshold for becoming agitated and that his presentation is not consistent with stated injury. He also asked me for narcotics just after sitting on the gurney. Should be placed near security for safety of staff.”
Even though the majority of these BAs describe noncriminal patient behavior, BA authors demonstrated a low threshold for describing patient behavior as unlawful.
“Pt agitated and threatening to harm staff after being told her marijuana and medications had to be stored for duration of hospital course. Pt aggressively removed her own IV. Pt required UCPD escort off property. Be aware of potential for escalation, place in high visibility area, low threshold to contact security or UCPD.”
Implied overuse
These BAs commented on the patient’s increased use or stated overuse of health care resources, and BA authors suggested limiting care resources, such as appointments, medications, and transportation.
“Fifteen ER visits over past year c/o [complaining of] s/p [status post] seizure. Appears to have some secondary gain for frequent ER visits. May be drug seeking for Ativan. Do not provide drugs of abuse unless there are strong clinical indications… Do not provide meals unless in the ER > 6 hours. Do not provide taxi vouchers unless medically necessary.”
These BAs often included speculation as to why the patient was utilizing medical resources and suggesting, or plainly stating, a concern for misuse. These BA authors invoke a patronizing tone, by describing patient’s use of the medical system as inappropriate.
“Newly homeless male with multiple ED visits for various somatic complaints. He may be seeking respite from homelessness… Try not to positively reinforce misuse of emergency services.”
While reference to patients’ social determinants of health were limited in general, these BAs often noted insurance status and housing, simultaneously recognizing a patient’s constrained access to resources and suggesting further restricted access to health care.
“Before deciding to admit, please review discharge summary and discuss with primary inpatient attendings on Psychiatry, due to history of no benefit from inpatient hospitalizations, and zero reimbursement from pt’s health insurance.”
These BA authors seem to advocate for protection of the medical system over the patient.
“…PMD or her Methadone Clinic should provide all medications. Do not provide food unless in the ED > 6 hours. Do not provide taxi vouchers as she should go home the same way she arrived.”
Advocacy
A minority of BAs provided patient-specific details to seemingly advocate on a patient’s behalf. These BAs suggested support and defense for the patient.
“Pt is Cantonese-speaking and will need Cantonese Interpreter for any visits. Primary language in chart is English due to how pt does not read Cantonese and wants all AVS [after visit summary]/MyChart correspondence messages to be in English.”
While similar to the theme “coordinating care,” these BAs included patient vulnerabilities and clinical elements to account for future medical decision making.
“Pt has very strong wish to be DNR/DNI, please refer to the POLST and Advance Directive which are scanned. She is concerned that she might be mistakenly resuscitated due to a ‘Prior’ Full code status recorded in the hospital, so please be advised that this is incorrect.”
Often, these BAs included unique patient details that seemingly had no other appropriate home in the EHR.
Coordinating care
In these BAs, authors appeared to be coordinating care for patients, despite being unable to communicate with future providers in real time. These BAs included appointment scheduling details, ways to contact the patient, and recommendations for follow-up providers. BA authors attempted to direct future care across clinical settings by communicating current patient-specific, yet standard-of-care, clinical information. In some instances, BA authors expressed lessons learned about prior unusual clinical presentations, reactions, or at-risk behaviors.
“Patient has ESRD [end stage renal disease] on peritoneal dialysis, chronic anemia and diastolic heart failure. He does not tolerate blood transfusions and has developed TACO (Transfusion-Related Cardiac Overload) in the past. If presenting to the ED with anemia, please transfuse only 1 unit at a time. Consult renal to coordinate his peritoneal dialysis with the transfusion…”
These BAs extend beyond logistic details: BA authors used these BAs to educate future providers and to express their opinion on what is best for the patient.
“Baseline Suicidal Ideations; multiple ED visits & cleared by psychiatry after reassurance. We need to think of some strategies to keep him out of the ED and discourage this behavior. Suggestions include: 1. Not consulting psychiatry if pt appears at baseline. 2. Do not feed him. 3. Do not provide any extra supportive care, such as nursing presence, or anything that will suggest to him that this is the place to get his needs met…”
Venting
Other BA authors seemed to use BAs to express their frustrations, without clear suggestions for future providers or patient care plans.
“Patient was rude on arrival to the PACU [post-acute care unit]. Very ineffective coping with course of care. Complained she had too much urine and needed to use bedpan 3 times. When belongings were not found quickly enough and she felt it was lost, she claimed she will make a scene and sue everyone in the hospital.”
Often, these BAs shared details of a clinical encounter during which a patient’s needs were not met.
“Pt very angry and upset over hospital course. Was upset surgery ran late and wanted to leave asap to pick up children from school. Pt confrontational and argumentative over everything. Demanding to see physicians but refused to wait…”
Authors in these BAs seem to place a negative value judgement on the actions they describe, disparaging the patient.
“Patient is currently in a recovery facility for his alcoholism through the last week of August 2017. Patient tries to get appointments to have a reason to get away from the sober living environment so he can drink.”
Warning
Some BA authors warned other providers about patient actions, using BAs to express safety concerns, such as weapon possession or risk for self-harm. BA authors also detailed specific incidents of inappropriate or aggressive behavior. Intertwined with the theme of “criminalization,” many BA authors provided a nonspecific directive to involve security.
“Patient physically assaulted staff via attempted kicking at security staff. Patient then scratched a security officer on the arm/elbow, causing multiple cuts. Contact security immediately for any escalation in behavior.”
Prior experiences may provide vital information for future encounters; however, BA authors demonstrated a dissonance between recognizing an individual’s medical or psychiatric illness’ contribution to current behavior and controlling it with a one-size-fits-all approach.
“Hx [history] of Cerebellar Atrophy w/resulting BLE [bilateral lower extremity] weakness, aphasia & memory deficits. She also has a history of depression, anxiety & mania. While awaiting IP [inpatient] bed, she crawled out of bed & onto the floor. When instructed to return to her bed, she became verbally abusive & attempted to kick the nurse. Be aware of her potential for assaultive behavior. Set firm limits on behavior. File criminal charges for any criminal behavior.”
A frequent focus of these warnings was opioid use; BA authors informed the reader of a history of opioid misuse and attempted to curtail further use by detailing who should be prescribed controlled substances and when.
“NO OPIATES FOR THIS PATIENT. Patient has demonstrated it is unsafe to give her opiates. Was unresponsive and woke up w/narcan, hospitalized, then, found to have B/L [bilateral] large Pes [pulmonary emboli] as well. No opiates for pain control, not even short term. Prior to this event there was concern for diversion and neglect at home.”
Overlapping with the theme of “implied overuse,” BA authors often noted a desire to limit opioid prescriptions, referencing prior adverse events or breaches of opioid agreements.
Discussion
To our knowledge, this is the first study to qualitatively examine the content of BAs; we found BA authors predominantly used a negative, nonpatient-centered tone, and introduced stigmatizing language into the EHR, by criminalizing and dramatizing patient actions and implying patient overuse of the medical system. We found that patients with BAs were more likely to have psychiatric and substance use-related diagnoses, identify as Black, and have public insurance than patients without BAs, as described in prior research.1,17,18
The public holds robust stigmatizing attitudes against those with psychiatric and substance use-related diagnoses,22–24 believing that these individuals are more likely to behave violently. 25 How clinicians document these diagnoses matter: mental health workers find a fictional character more personally culpable for their condition and deserving of punitive treatment if referred to as a “substance abuser” rather than a person with a “substance use disorder.” 24 Additionally, providers use more judgmental language and excessive quotations in EHR documentation for Black patients.26–29 Clinician and staff distrust of Black patients is seen in the increased request for security to stand by30,31 and use of physical restraints. 32 It is concerning that Black patients and those with psychiatric or substance use-related diagnoses bear the burden of BAs in this practice, as this may further the cycle of suspicion and negatively impact future care.
BAs are EHR communication tools that lack standardization and structure. Without structure, BA authors often fill this space with one-size-fits-all language, canned phrases, and information that lacks clear purpose. Interprofessional communication—about staff safety and patient well-being—is diluted by warnings without a clear plan and limit setting without goals. Health systems should collaborate with Epic to restructure this tool to ensure health care providers and administrators document in a patient-centered manner. Policies are needed to direct both creation of new BAs and review and deletion of outdated, inappropriate, or unnecessary BAs. Promoting workplace safety is paramount; despite promoting feelings of safety,7,8 BAs have not been shown to reduce rates of violence,1,9–13 and they may operate as patient labels rather than tools for violence prevention. 13 Looking forward, urgent safety matters should be documented in the patient’s chart using structured templates that include person-first language, timeliness, justification, and recommendations for reevaluation or resolution. Ultimately, institutions may decide to limit who is able to write BAs, or require that BAs undergo review and approval prior to activation, and educate BA authors and reviewers on the potential of written documentation to facilitate implicit bias and structural racism.
BAs reflect many of the biases previously identified in medical encounters.26–29 Having a mental health diagnosis and poor functional status are characteristics associated with “difficult” patients; similarly, engaging with patients who endorse multiple symptoms, have high expectations, or have increased use of the medical system directly predicts “difficult” encounters. 33 As both a potential reflection of insidious discrimination and as overt and enduring labels in the EHR, BAs exemplify the circular process of labeling, stereotyping, and exercise of power that defines stigma. 34 Our research acutely demonstrates that Black patients and those with mental health and substance use-related diagnoses are more likely to have BAs and have inappropriate language used about them, highlighting a potential source of physician bias: simply knowing about a stereotype or label distorts future processing about an individual, 35 and future physician behavior is negatively influenced by implicit bias36,37 and exposure to stigmatizing language. 38
Limitations
While BAs are a built-in function in Epic, the largest EHR in the United States, their use is dictated by each individual health care institution; as our study took place at one institution, our commentary should be taken within the context of our institution’s policies. We analyzed active BAs only, to focus on BAs that could influence current patient care. We did not interview BA authors or patients, and therefore can only speak to the perceived tone and intention of BAs. Demographic clinic data was only available in aggregate, precluding a logistic regression analysis.
Conclusions
Our study found a predominantly negative tone and potentially biased application of BAs, demonstrating the consequences of the unstructured, unregulated use of BAs. What should be standard of care—communicating prior adverse reactions or safety concerns—is relegated to a space ill-equipped to transmit care details in a clear, timely, or patient-centered way. The result is often patient labeling, didactic lessons that age poorly, and long-lasting documentation of transitory negative impressions. By investing resources into reforming BAs, through education and policy change, health care institutions can dismantle this form of structural stigmatization.
Footnotes
Authors’ Contributions
Z.K., I.K., and M.E.G.: Conceptualization, methodology, formal analysis, investigation, and reviewing and editing. Z.K.: Writing the original and subsequent drafts.
Disclaimer
The content does not necessarily represent the official views of the National Institute on Minority Health and Health Disparities (NIMHD), the National Institutes of Health (NIH), or the Robert Wood Johnson Foundation (RWJF).
Funding Information
M.E.G. received support through a National Institute on Minority Health and Health Disparities (NIMHD) K23MD015115 and the Harold Amos Medical Faculty Development Program (AMFDP) funded by the Robert Wood Johnson Foundation (RWJF) Award 80734.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.