
Abstract
Introduction:
Despite the growing Arab population in the United States, there are gaps in our understanding of the health needs of Arab communities across the United States. To further our understanding of the health needs of Arab populations in New York City, New York University Langone Health (NYULH) conducted a community needs assessment of Arab Americans. The objectives of this needs assessment were to (1) identify individual and community-level health needs among Arab American community members in Brooklyn, NY; (2) identify gaps in available resources for Arab American community members in Brooklyn, NY; and (3) use findings from the assessment to inform NYULH and community-based organization programs for Arab American community members in Brooklyn, NY.
Methods:
This community health needs assessment was conducted using principles of community-based participatory research in partnership with community- and faith-based organizations that serve Arab American communities. A convenience sample was used to recruit participants (N = 511) from community-based settings in Fall 2019.
Results:
The prevalence of self-reported chronic diseases was high in the sample: 16% (diabetes), 25% (hypertension), and 26% (high cholesterol). Regular dental cleanings were low among participants with only 38% reporting a cleaning less than 6 months ago. Food insecurity (33%) and housing insecurity (18%) were reported by some participants.
Discussion:
This community health needs assessment identified individual and community-level health needs among Arab American community members in Brooklyn, NY. Specific health concerns included high chronic diseases, minimal dental care, and low cancer screenings.
Conclusion:
The findings from this assessment contribute to the limited health data on Arab Americans and highlight important health disparities that urgently need to be addressed, specifically around health screenings, prevention and management of chronic diseases, and dental care. Addressing these gaps in care and health outcomes will require culturally and linguistically tailored health programs designed for Arab American populations, which require input from community members and organizations to facilitate the effectiveness and acceptability of these programs.
Introduction
There are an estimated 3.7 million Arab Americans with ancestry from Arab countries in the United States, including significant representation from Egypt, Iraq, Syria, Lebanon, and Palestine. 1 New York has the fourth largest population of Arab Americans (194,809) and the majority of recent Arab immigrants to New York are from Egypt, Yemen, and Morocco. 1 Arab identity is complex in relation to geographic origins, race, ethnicity, culture, faith, language, and historical narratives, all of which require data collection methods informed by the lived experiences of Arab Americans and people from Arab-majority countries.2–4
Despite the growing Arab population in the United States, there are gaps in our understanding of the health needs of Arab communities across the United States. The lack of data on Arab Americans is directly tied to the absence of an “Arab” response option for racial/ethnic identity questions, which is evident in state and federal government forms, and national health questionnaires. 5 Often Arabs are classified as “White” resulting in the erasure of demographic and health information on Arab American populations, further masking the disparities between White populations and ethnic minorities.2–7 Health assessments among Arab Americans that have been conducted found significant health disparities related to poor mental health, tobacco use, chronic diseases such as diabetes, hypertension, and cancer, and intimate partner violence compared with non-Arab White Americans.6,8–11 Moreover, studies consistently reported barriers in access to health care by Arab Americans related to navigating the complex U.S. health care system, language barriers, and limited public health knowledge, which contributed to low health service utilization, highlighting the need for linguistically and culturally competent care to bridge gaps in access.9,12 It is critical to note the long-standing discrimination and stigma faced by Arab populations in the United States dating back decades, including heightened waves after the September 11, 2001 attacks and Executive Order 13769 banning refugees and immigrants from predominately Arab countries.9–11,13 The few studies available on the impact of social and political discrimination on Arab American health have indicated associations with poor maternal and child health outcomes.14,15
To further our understanding of the health needs of Arab American populations in New York City, New York University Langone Health (NYULH) conducted a community needs assessment of Arab Americans in Brooklyn, NY in Fall 2019. This needs assessment was undertaken at the request of a group of Arab-serving community-based organizations (CBOs) that had long been partners of the NYU health care system in Brooklyn. Their goal was to raise the visibility of Arab Americans within the hospital catchment area to hospital leadership and administrators, to identify the health needs specific to this community in Brooklyn, NY, and to use findings to inform the development of culturally relevant health programs and policies.
While physical and mental health needs have been extensively studied among various racial/ethnic minorities, it is crucial to prioritize examining these issues specifically within the Arab American community. 10 This is pivotal to preventing the perpetuation of health disparities and ensuring equitable health outcomes. 10 Health needs assessments conducted in Michigan, Chicago, and New York have provided valuable information on Arab American health. However, the varying geographic locations, diversity within the Arab American population, and multilevel determinants including sociocultural, physical, and built environments underscore the importance of examining health disparities within Arab American populations.9,11,16–18
The objectives of this community health needs assessment were:
Identify individual and community-level health needs among Arab American community members in Brooklyn, NY. Identify gaps in available resources for Arab American community members in Brooklyn, NY. Use findings from the assessment to inform NYULH and CBO programs for Arab American community members in Brooklyn, NY.
Methods
Participants
The Brooklyn Arab American needs assessment was conducted from September to December 2019. Eligibility criteria for participating included being 18 years or older, self-identification as Arab American, and currently residing in Brooklyn.
Data collection
The needs assessment was conducted using principles of community-based participatory research, specifically working in partnership with CBOs in all aspects of the assessment from the development of the instrument, data collection, analysis, and interpretation of the data to the dissemination of findings. As stated previously, this assessment was initiated at the request of Arab-serving community organizations in Brooklyn, NY. This partnership, called the Arab American community advisory group, with Arab-serving organizations was formed by NYULH Brooklyn to identify health needs among Arab American residents. The community advisory group met on a quarterly basis to discuss community health needs and concerns. In September 2018, the Arab American community advisory group requested an updated community health assessment to understand the current needs of Arab American residents in Brooklyn as the last assessment was conducted in 2008. A working group for the community assessment was formed from the community advisory group composed of the following organizations: Arab American Association of New York, Arab American Family Support Center, Moroccan American House Association, Arab Health Initiative of Memorial Sloan Kettering Cancer Center, Family Health Centers at NYU Langone, NYULH Center for the Study of Asian American Health, NYU Langone Hospital—Brooklyn, and the NYLH Brooklyn Data Station. The working group was composed of health care providers (e.g., physicians, social workers, community health workers) and health researchers with representation from diverse racial/ethnic, age, and education groups, which shaped the design and implementation of this needs assessment. The working group met to develop the survey instrument to focus on general and specific health needs among Arab American residents. Throughout the process of survey development, partner organizations provided valuable contributions to the survey instrument to identify the needs of their communities. Community partners assisted with the translation of the survey instrument to Arabic and back translation to English to ensure the accuracy and appropriateness of the translation.
NYULH provided training to staff members from these organizations who were fluent in Arabic and English on administering the survey to participants, covering topics such as obtaining verbal consent, determining eligibility criteria, maintaining privacy and confidentiality, engaging participants during recruitment and the survey, and sensitivities around certain topics covered in the assessment (e.g., mental health and alcohol consumption).
A convenience sample was used to recruit participants (N = 511) from a variety of community-based settings. Participants were recruited from the waiting areas of partner organizations, at mosque and church gatherings, tabling at community organizations and events, outreach to ESL classes, caregiver support groups, health fairs, and youth development programs as well as through referrals from community members. On a weekly basis, a NYULH staff member visited the partner organizations to collect the completed paper surveys. These surveys were then entered into the NYULH RedCap database. 19 Data entry and data quality checks were completed by a team of interns fluent in Arabic and English. Participants were offered a $10 gift card to complete the survey. The survey took approximately 20 min to complete.
Needs assessment instrument
The domains and examples of questions under each domain in the assessment survey were: (1) participant demographics (e.g., age, marital status, and education); (2) health status and physical activity (“During the past week, other than your regular job [if applicable], did you participate in any physical activities or exercise such as running, pushups, gardening, or walking for exercise?”); (3) health care access (e.g., health insurance status, recent doctor appointments, and preventative care such as cancer screenings); (4) mental health and stress (e.g., PHQ-2 and sources of support); (5) food insecurity (concerns around funds to purchase food and food lasting); (6) environment (health issues of concern to Arab American community in Brooklyn); and (7) households with children (e.g., available childcare and engagement with child). The complete needs assessment survey can be found in Supplementary Data S1 (English and Arabic versions).
Data analysis
Descriptive statistics were computed for all variables. Self-reported health findings were stratified by age, and chi-square tests were conducted to note differences in the sample. Missing data were not included in the analysis. Cronbach’s α was used to assess reliability of the patient health questionnaire (PHQ)-2. All statistics were computed using SAS version 9.4 (Copyright 2016 by SAS Institute Inc., Cary, NC) and SAS-callable SUDAAN version 11.0.4 (Research Triangle Institute).
Ethics
The Arab American needs assessment was submitted to NYULH’s institutional review board as a modification to an existing needs assessment protocol. The study modification was approved on September 21, 2019.
Results
Demographic information on participants is detailed in Table 1. The majority of participants were female (60%), most have lived in the United States for 10 or more years (46%), and a majority had public health insurance (77%). In relation to income and education levels, 45% had an annual household income less than $25,000, 32% had less than a high school education level, and 26% had a college or higher degree. Languages spoken by participants included Arabic only (48%), and Arabic and English (46%). Participants were born in a variety of countries, including Yemen (25%), Morocco (24%), Egypt (14%), and the United States (11%).
Participant demographics (N = 511)
Participants were asked about self-reported health status, which is presented in Table 2. A series of questions were asked about whether participants had ever been told by a provider that they had diabetes, hypertension, or high cholesterol. Self-reported diagnoses were 16% (diabetes), 25% (hypertension), and 26% (high cholesterol). Stratifying results by age revealed a high prevalence of diabetes (60%), hypertension (80%), and high cholesterol (66%) among participants aged 65 and older. Significant associations were noted between all age groups with diabetes, hypertension, and high cholesterol.
Self-Reported Chronic Conditions, Dental Care, and Mental Health
p < 0.05.
Body mass index was calculated using self-reported height and weight, which indicated a sizable proportion of participants were obese in the following age groups: 25–44 (25%), 45–64 (31%), and 65 and older (27%). Overall, obesity among participants was 24%. Risk of depression was measured using the PHQ-2 and reliability of it was low in the sample (Cronbach’s α of 0.78). A total of 21% of participants were at risk for depression.
Next, participants were asked about cancer screenings (Table 3). A total of 52% of female participants were screened for cervical cancer less than 3 years ago, compared with 45% reporting they had never been screened. Cervical cancer screenings (less than 3 years) varied by age: 18–24 (9%), 25–44 (58%), 45–64 (70%), and 65 and older (42%) with significant results found for ages 18–24 and 45–64. Most female participants (66%) had been screened for breast cancer less than 2 years ago. Breast cancer screening varied by age (71% of women aged 44–64 and 25% of women aged 65 and older) with lower rates among older women. Most participants (56%) had never been screened for colon cancer. There were differences for colon cancer screenings by age with 39% of participants aged 44–65 and 68% of participants aged 65 and older reported being screened in the past 10 years.
Cancer Screenings
p < 0.05.
Unable to conduct chi-square tests because of the large amount of missing data.
Finally, participants were asked about social needs related to food, housing, and barriers to care, and priority community health issues and resources needed (Table 4). Food insecurity (33%) and housing insecurity (18%) were reported by some participants. In relation to barriers to care, participants cited transportation problems (20%), not able to afford care (19%), and did not have time/took too long (16%). The top five community health issues cited by participants included diabetes (58%), cancer (46%), heart disease (40%), obesity (33%), and mental health (27%). Participants mentioned affordable housing options (50%), access to high-quality medical care (40%), access to high-quality dental care (35%), vaping/hookah prevention (35%), and jobs and training (33%) as resources needed for community members. Resources adults cited as needed for teenagers included smoking, vaping, and hookah prevention (41%); access to education and college preparation courses (38%); job readiness and training programs (36%); substance misuse awareness (35%); and access to mental health services and support (30%).
Social Needs, Priority Community Health Issues, and Resources Needed
Discussion
This community health needs assessment identified individual and community-level health needs among Arab American community members in Brooklyn, NY. Consistent with previous studies among Arab Americans, participants had high prevalence of chronic disease, particularly diabetes, 13% among all participants, 28% in participants aged 45–64, and 60% in participants aged 65 and older; and high cholesterol, 26% among all participants, 45% among participants aged 45–64, and 66% among participants aged 65 and older.9,12,17 These results compared with the 12% of the U.S. population that has diabetes and 11% of the U.S. population with high cholesterol.20–22 While 25% of participants reported having hypertension, this prevalence was lower than the national average of 45%. 23 Prior studies among Arab Americans consistently reported diabetes as a top health concern, as well as hypertension (range of 13–36%).12,17,18 However, the low reporting of participants receiving dental cleanings has not been reported in previous literature. Mental health was an additional top concern identified by participants (27%). This finding was consistent with other studies that have highlighted mental health as a concern for Arab Americans including increased rates of anxiety and depression among Arab immigrants compared with U.S.-born Arab Americans and societal stigma as the primary fear preventing participants from accessing mental health care.9,16
The majority of data published on Arab American health have emerged from Michigan, which is home to the largest Arab population in the United States. Studies conducted in Michigan were predominately composed of Lebanese participants (65% in some studies), reflecting the significant Lebanese presence in the state. 17 Studies conducted among Arab communities in other settings often do not include specific data on Arab identity. In our study, 25% of participants were from Yemen, 24% from Morocco, followed by participants from Egypt (14%), United States (11%), Palestine (7%), Syria (7%), and Jordan (7%); participants from Lebanon were the smallest demographic (3%) in our assessment. These findings from our study and others highlight the diversity within the Arab American population and reinforce the need for appropriate representation across published literature on Arab American sub-ethnic groups. Further, in our study, only 11% of participants were U.S.-born. This is lower than the 47% U.S.-born Arab population in NYC but provides valuable insights into the health concerns of Arab immigrants who make up a significant portion of the community. NYC has a higher population of Arab immigrants compared with other cities, with 53% of the Arab-identified population born abroad, contrasting with the nationwide percentage of 43%. 24 This underscores the diversity and complexity of the Arab American community in NYC, further emphasizing the need for increased visibility of Arab Americans within health studies. The health disparities identified in this study and other research provide a partial perspective of the health and well-being of Arab Americans, who are often overlooked in health equity initiatives because of their lack of representation in health data. While we may only have an incomplete understanding of Arab American health, the data we do have available indicate significant health disparities and gaps in access to care, which urgently need to be addressed by public health agencies and health care systems through culturally tailored and sustainable initiatives to reach Arab communities. As with our needs assessment, these health equity initiatives should be planned and implemented in partnership with community- and faith-based organizations, who have the expertise and relationships to ensure the acceptability and feasibility of these programs.
Health initiatives in response to needs assessment findings
The findings from this community needs assessment informed NYULH and CBO programs and services for Arab American community members in Brooklyn, NY. The community assessment working group met to discuss and interpret findings, including dissemination plans and how findings could inform programs for Arab American residents. Members of the working group disseminated findings from the assessment in various forums (e.g., presentations and one-pagers) and NYULH and CBOs launched a series of health initiatives to address health disparities identified through the needs assessment. Moreover, consistent with the literature emphasizing the need for culturally and linguistically competent care to address health disparities in Arab American community, NYULH and community partners used culturally informed approaches for these implementation and dissemination efforts (detailed in Fig. 1).9,12
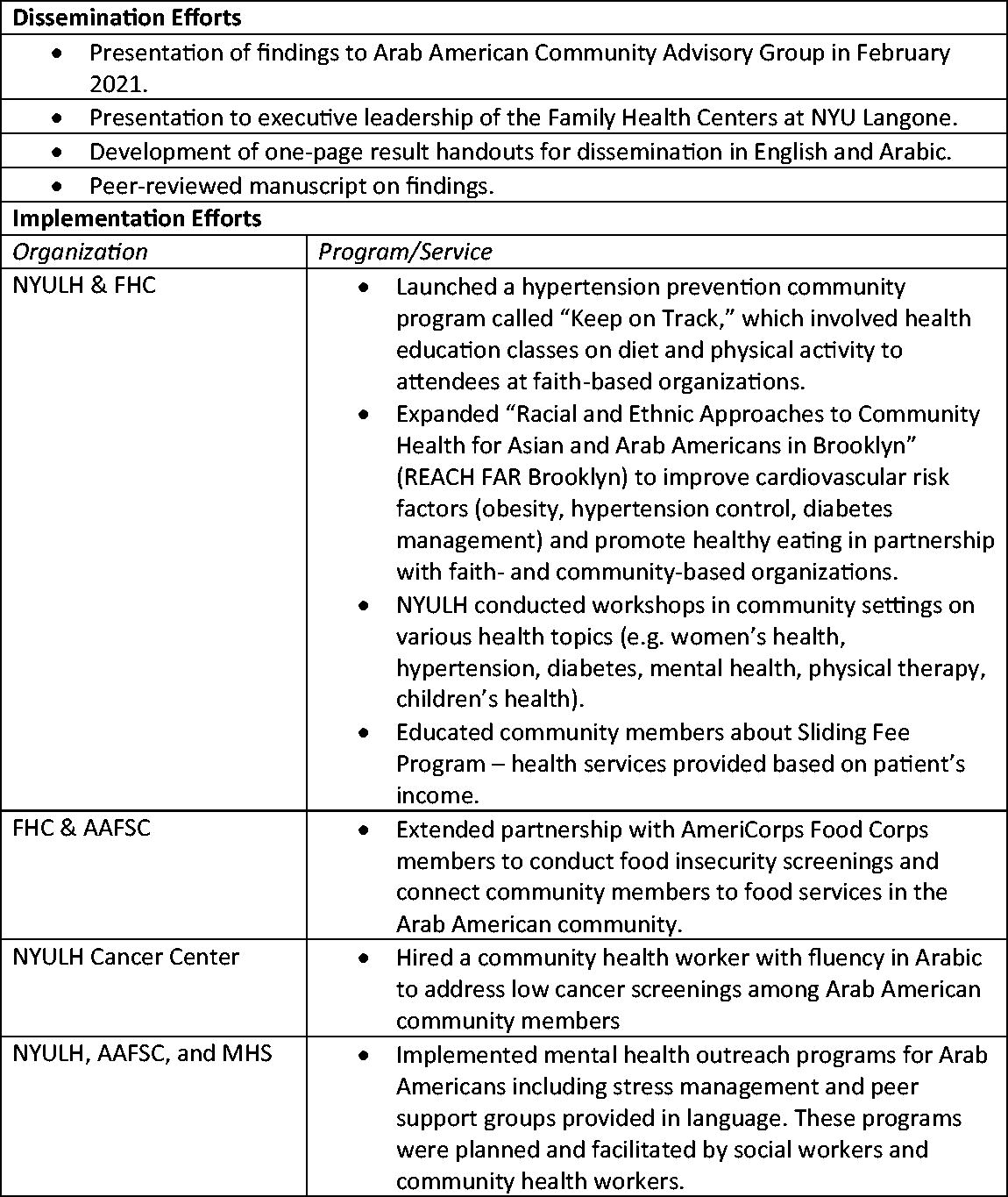
Community needs assessment dissemination and implementation efforts.
Additionally, while the data for this needs assessment were collected prior to the COVID-19 pandemic, the urgency to address gaps in Arab American health have only become more apparent. The exclusion of racial/ethnic data categories for Arab Americans persisted in COVID-19 research studies despite racial/ethnic health disparities increasing during the pandemic. 7 Given the high prevalence of underlying health conditions and comorbidities of COVID-19 such as diabetes, cardiovascular disease, and hypertension identified among Arab Americans, it is likely that COVID-19 may have had a disproportionate impact in Arab populations. 25
Strengths and limitations
Strengths of this community health needs assessment include partnering with community organizations to ensure culturally appropriate and in-language data collection methods, and community-based collection efforts to ensure the wide reach of the survey among community members. Another strength is the findings from the assessment informing health initiatives for Arab American community members. Further, these results contribute to the existing literature on Arab American health and expand our understanding of health needs in this critically understudied population. There are some limitations to this study, including the use of a convenience sample, which affects the representativeness of the sample and generalizability of the findings. Further, the high non-response rate to certain questions may reflect participant discomfort with answering certain questions, which may be due to stigma associated with specific health topics (e.g., cervical cancer screenings and mental health). Given the missing responses in our data, which ranged from 10% to 20%, in particular to certain questions about income, depression, and weight we were limited in our analysis, which we kept to descriptive statistics and chi-square tests when feasible because of these missing data. Finally, the PHQ-2 had low reliability with this sample, which suggests limitations of using the PHQ-2 to measure depressive symptoms in Arab American populations.
Conclusion
The findings from this community health needs assessment highlight important health needs among Arab American residents in Brooklyn, including low cancer screenings, high prevalence of chronic diseases, and minimal dental care. As noted in previous studies, there is a dearth of health information on Arab Americans given aggregate racial/ethnic categories used in data collection instruments, which contributes to the erasure of critical health information on Arab Americans. While efforts by individual researchers and institutions to address these knowledge gaps are helpful, systematic changes in how government agencies and health care systems collect racial/ethnic data are urgently needed to redress the invisibility of Arab Americans and other ethnic groups. 26 The Arab American population is diverse and growing, and without timely and accurate data on their health and well-being, we are missing crucial information to reduce health disparities in this population. In 2024, the White House Office of Management and Budget announced new federal guidelines for collecting race and ethnicity data, including the addition of a Middle East and North Africa (MENA) category to federal forms, including the 2030 census. 27 This is an important step at the federal level to accurately collect data on Arab Americans, identify health disparities, and allocate resources accordingly. However, given the history of discrimination against and surveillance of Arab communities, government agencies need to share plans for ensuring the confidentiality of data collected and transparency regarding how data will be used, so community members feel safe responding to this new racial/ethnic category on government forms. Further, some advocacy groups are concerned that the MENA category may contribute to the undercounting of Black Arabs and indigenous populations in Arab-majority countries, among other potential issues with groups not being accurately captured under the MENA category. 28 If this new racial/ethnic category is implemented in a way that earns the trust and participation of Arab communities and captures the diversity of Arab Americans, it has the potential to address significant gaps in our understanding of Arab Americans and facilitate health initiatives to address health disparities among Arab Americans.
Footnotes
Acknowledgments
The authors want to thank the staff of the following organizations for their assistance with this community needs assessment: Arab American Association of New York, Arab American Family Support Center, Moroccan American House Association, and the Arab Health Initiative of Memorial Sloan Kettering Cancer Center. The authors want to thank and acknowledge Dr. Ahmad Jaber, one of the founders of the Arab American Association of New York, who dedicated his life to the provision of medical care, education, and social services to immigrant communities in NYC.
Authors’ Contributions
Writing original draft: N.A., A.R., and M.D.T. Formal analysis: N.A. Conceptualization: E.G., N.I., S.K., M.D.T., M.J., R.C., Y.K., C.A., S.L., and G.A. Writing—review and editing: N.A., A.R., N.I., E.G., S.K., M.D.T., M.J., R.C., Y.K., C.A., S.L., and G.A.
Author Disclosure Statement
The authors have no conflicts of interest to report.
Funding Information
This study was funded by
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.