
Abstract
Introduction:
Misclassification of American Indian and Alaska Native (AI/AN) peoples exists across various databases in research and clinical practice. Oral health is associated with cancer incidence and survival; however, misclassification adds another layer of complexity to understanding the impact of poor oral health. The objective of this literature review was to systematically evaluate and analyze publications focused on racial misclassification of AI/AN racial identities among cancer surveillance data.
Methods:
The PRISMA Statement and the CONSIDER Statement were used for this systematic literature review. Studies involving the racial misclassification of AI/AN identity among cancer surveillance data were screened for eligibility. Data were analyzed in terms of the discussion of racial misclassification, methods to reduce this error, and the reporting of research involving Indigenous peoples.
Results:
A total of 66 articles were included with publication years ranging from 1972 to 2022. A total of 55 (83%) of the 66 articles discussed racial misclassification. The most common method of addressing racial misclassification among these articles was linkage with the Indian Health Service or tribal clinic records (45 articles or 82%). The average number of CONSIDER checklist domains was three, with a range of zero to eight domains included. The domain most often identified was Prioritization (60), followed by Governance (47), Methodologies (31), Dissemination (27), Relationships (22), Participation (9), Capacity (9), and Analysis and Findings (8).
Conclusion:
To ensure equitable representation of AI/AN communities, and thwart further oppression of minorities, specifically AI/AN peoples, is through accurate data collection and reporting processes.
Introduction
American Indians and Alaska Natives (AI/AN) comprise about 2.9% of the total U.S. population. 1 However, in parts of the United States, some counties are well over 50% of the population. 2 Those AIs who are members of a state or federally recognized tribe have health coverage through the Indian Health Services (IHS), Tribal Health Services, or in Urban Indian centers as per U.S. treaty responsibilities. Misclassification of race is a significant problem when describing health disparities and equity. With many decisions, including appropriate funding, organizational practices, and quality measures, accurate data are paramount. In short, this has been problematic for AI/AN populations as they are often racially misclassified in datasets, which are critical for decision-making. Although the purpose of this article is centered on cancer disparities and racial misclassification in cancer registries and databases, it is important to note that racial misclassification can be found in other major databases used to monitor health trends. For example, oral health data rely heavily on publicly available databases and, depending on how race data are collected, may be subject to varying amounts of racial misclassification. 3 If the data are not linked with IHS patient files, this misclassification in oral health data may skew or alter actual trends in the data.
In the United States, the age-adjusted cancer mortality rate (AADR) was 146.6/100,000, which was the second leading cause of death in 2021 following only heart disease (AADR 173.8/100,000) for both the overall population and the AI/AN population. 4 It is evident that pervasive and long-standing health disparities exist within the AI/AN communities. Some areas across the United States (such as the Northern and Southern Plains) experience significant health disparities among AI/AN males for colorectal, liver, and stomach cancer incidence. Among AI/AN women this includes liver, stomach, kidney and renal cell, cervix, and gallbladder cancer incidence.5–7 Thus, despite their small numbers compared with the general U.S. population (an estimated 5.9 million in 20201), the AI/AN population is important in eliminating cancer incidence disparities.
There is clear evidence that oral health is critical for disease incidence and survival, including all-cause mortality8–14 but specifically heart disease,14–18 dementia, 19 stroke, 17 and cancer.15–18,20–24 Cancers associated with either tooth loss or periodontal disease include oral cancer,25–27 esophageal cancer,23,26 stomach cancer,23,25,26 colorectal, 28 liver cancer, 23 and lung cancer.22,29 These studies primarily focus on periodontal disease or tooth loss as a measure of oral health and there are often inconsistencies in the assessment of periodontal disease and tooth loss (whether self-reported or measured). 21 In 2020, AI/AN populations had the highest proportion of any racial or ethnic group in the United States (45.2%) not having seen a dentist in the past year and the most likely (23.7%) to be age 65 or older and have all of their teeth removed. 30
Research has shown that misclassification of AI/AN peoples exists across various databases in research and clinical practice.31,32 The implications are far-reaching as it can distort reported population estimates of outcomes not only of the AI/AN population but other races as well. This is an issue of numerator and denominator dissonance, and the direction of the bias is underestimation of risk for AI/AN populations. Currently, cancer incidence data often include patients who are linked to the IHS master patient file. The process of data linkage is that state vital statistics and/or cancer registry records are linked with the IHS patient registration database. 33 This identifies AI/AN records previously misclassified as non-native in the state or cancer data, thus improving data quality and reducing racial misclassification. 33 Efforts have been made by major databases such as the National Cancer Data Base and hospital cancer registries to link historical cancer data to IHS patient files, but this work is not complete. To date, the only regularly linked data are cancer registries, the Surveillance, Epidemiology, and End Results (SEER) Program, and the National Program of Cancer Registries (NPCR), which released the aforementioned linked data. Thus, cancer incidence and mortality data are linked. Linkage of IHS data and the National Death Index mortality data for other diseases has been done as well. 34 The objective of this literature review was to systematically evaluate and analyze publications focused on racial misclassification of AI/AN racial identities among cancer surveillance data. Specifically for the purposes of this article, the authors reviewed cancer disparities because of the ongoing data linkages between cancer registries and the IHS through the Centers for Disease Control and Prevention (CDC).
Methods
The Southern Plains Tribal Health Board (SPTHB), a nonprofit tribal public health organization dedicated to serving the 43 tribal nations throughout Oklahoma, Kansas, and Texas, conducted this systematic literature review. The authors checked PROSPERO in July 2023 but were unable to register the article because data extraction was already completed. As of July 2023, there were no relevant protocols published. The authors used the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement for this review. 35 To standardize data abstraction and determine consensus, COVIDENCE, the systematic review management system was used. Article screening, data extraction, and assessments were done independently by two reviewers (A.J.L. and A.H.) to reduce errors and to detect any differences in interpretation between extractors. Any inconsistencies were discussed and resolved by a third reviewer (J.E.C.). For all included studies, the following were extracted: bibliographic information, study design, exposure(s), and outcomes, including definitions, characteristics of study participants, numerical results, and sample size. Specifically, cohort year, region/state, name of registry/data source, cancer type evaluated, if misclassification was discussed (yes/no), how misclassification was accounted for, and race/ethnicity data collected were abstracted.
The search strategy was designed to access published articles. Terms identified and their respective synonyms were used by corresponding databases and were used in an extensive search of the literature. Full copies of articles identified by the search, and considered to meet the inclusion criteria, based on their title, abstract, and subject descriptors, were obtained for data synthesis. Sources of published articles included Ovid MEDLINE, PubMed, Web of Science, Scopus, and University of New Mexico Native Health Database with the searches taking place from November to December 2022. The search terms used included (American Indian OR Native American OR Alaska Native or AIAN) AND (misclass or mis-class or miscategory or mis-category or miscode or mis-code) AND (cancer or malignant). After assessment of eligibility, the articles were qualitatively assessed. The importance of the results in terms of clinical and public health relevance was discussed.
The goal of the search strategy was to identify any type of cancer to better understand racial misclassification among AI/AN populations. However, the authors also wanted to specifically highlight any studies that pertain to oral and pharyngeal cancer in the Results section to introduce translational applications of findings to oral health.
CONSIDER Statement
There are minimal guidelines related to reporting of research that involves Indigenous peoples. 36 The CONSolIDated critERia (CONSIDER) for strengthening the reporting of health research involving Indigenous peoples statement was created to provide a checklist for the reporting of health research involving Indigenous peoples. 36 It establishes 8 research domains and 17 criteria for the reporting of equitable research practices with Indigenous peoples. 36 The CONSIDER checklist domains were used during data extraction for this systematic literature review.
Eligibility Criteria
This review considered all English-language studies that involve human subjects on the racial misclassification of AI/AN identity among cancer surveillance data. Exposures of interest considered were AI/AN communities in the United States. The primary outcomes of interest were reporting racial misclassification among cancer surveillance data. The review considered observational studies, including cohort studies, retrospective chart reviews of large centers, and cross-sectional studies.
A total of 566 articles were selected from the various databases listed above (Fig. 1). Through COVIDENCE, 28 articles were removed as duplicates. A total of 538 articles were screened through title and abstract review, where 339 studies were irrelevant based on the eligibility criteria. A total of 199 were screened with full-text analysis to assess eligibility and 113 were excluded. A total of 86 articles were assessed for full-text data abstraction, of which 20 were excluded. A total of 66 articles were included for the analysis.
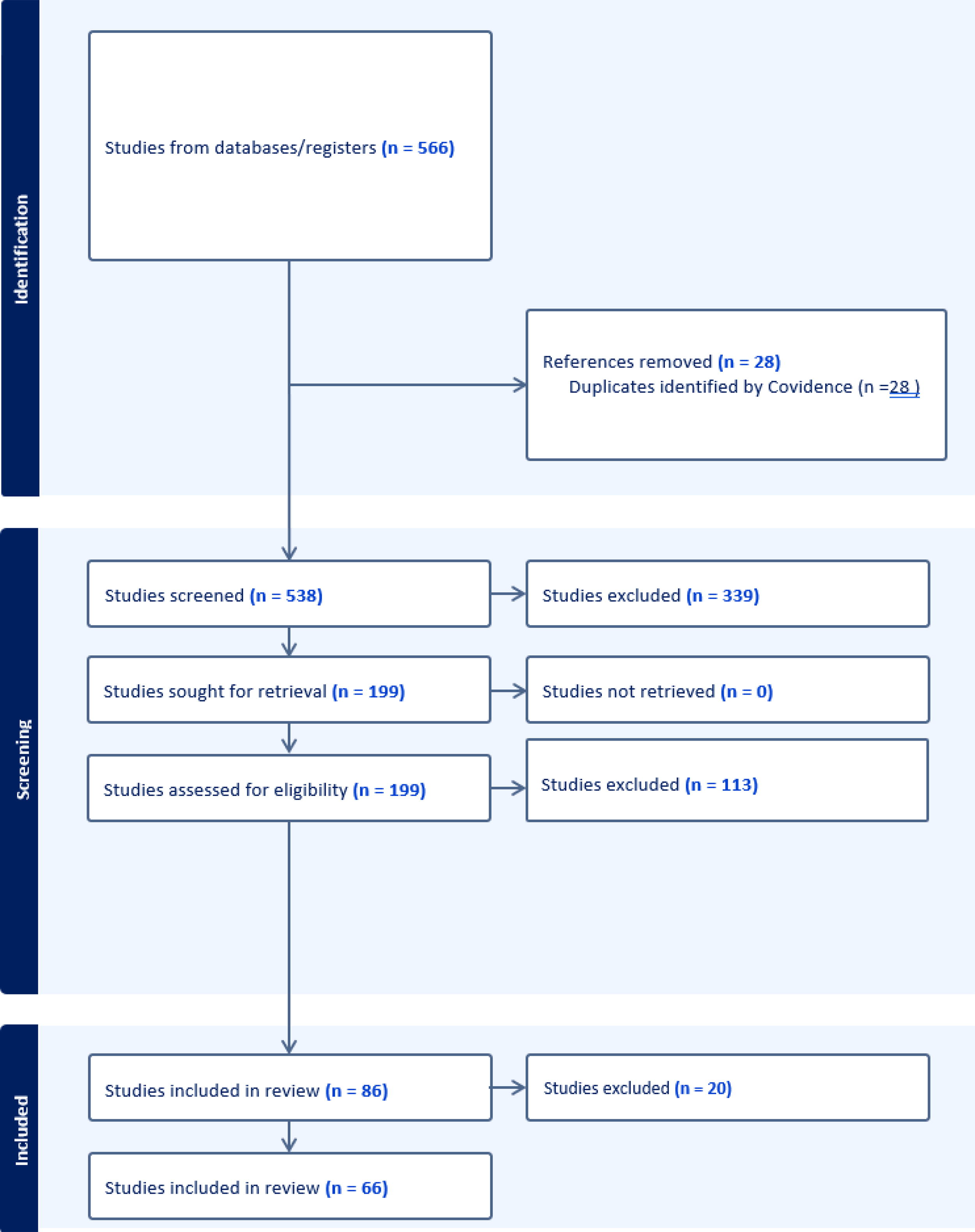
Study selection flow diagram, n = 66.
Results
A total of 66 articles were analyzed for this review according to the PRISMA statement and the CONSIDER statement.35,36 The published year for the articles ranged from 1972 to 2022.5–7,33,37–98 Cohort years for the data varied, with the earliest cohort year being 1950–1967 46 to the latest being 2014–2018. 7
Of the 66 articles on cancer surveillance among populations in the United States, 12 (18%) did not discuss racial misclassification or did not account for misclassification in their study.
Articles That Discussed Misclassification
A total of 55 (83%) of the 66 articles discussed racial misclassification (Table 1). The dates of publication for these articles ranged from 1986 to 2022. Of these articles, the oldest and largest cohort of data, or range of data collected, was from 1969 to 1994.54,55 The most recent cohort of data that addressed misclassification was from 2014 to 2018. 7 The most common cohort of data (17 articles or 31%) used was from 1999 to 2004.6,40,42,51,58,62,65,75,80,84,91–94,97 There were 15 articles (27%) that used cohorts of data that bridged the gap between 2004 and 2018.43,44,49,56,57,59–61,66,68–71,75,76,83,90
Table of Results, n = 66
AI, American Indian; AN, Alaska Native; CDC, Centers for Disease Control and Prevention; IHS, Indian Health Services; OCCR, Oklahoma Central Cancer Registry; NPCR, National Program of Cancer Registries; SEER, Surveillance, Epidemiology, and End Results; CHSDA, Contract Health Service Delivery Area; AHCA, Florida Agency for Health Care Administration; NCHS, National Center for Health Statistics; NCI, National Cancer Institute; NDI, National Death Index; NVSS, National Vital Statistics System.
For the race and ethnicity data that were collected among these articles, the most common racial group comparison, a total of 69% (38) of articles, was between AI
Articles That Did Not Discuss Misclassification
Of the 66 articles included in our analysis, we found 11 (16%) studies that did not address racial misclassification in their research (Table 1). The earliest study in this group was published in 1979, 46 and the latest studies were published in 2021.77,79 The largest cohort of data among these articles was from 1955 to 2004. 67
Six of the 11 (55%) studies did not reference racial misclassification in their studies. Among these studies, one study used IHS records to obtain data for their research. The remaining five (45%) articles used a variety of nontribal-based databases, including the National Center for Health Statistics, National Cancer Institute, state cancer registries, and Military Health System Data Repository not accounting for misclassification.
The four articles mentioned previously, which accounted for misclassification in their studies, addressed the issue in various ways. Paisano et al. noted racial misclassification as a limitation to their research, but the factor was not accounted for in the study itself. 73 Davidson et al. did not reference racial misclassification because of how the researchers obtained their data. 48 Data for this study were gathered from the Alaska Native Tumor Registry, which consisted of all AN patients who have been diagnosed with any cancer while being a resident in the state of Alaska. The Alaska Native Tumor Registry worked with tribal facilities in the state to ensure quality in the data. However, this linkage was not directly discussed in the study, although the report was created in partnership with the IHS. Three studies noted that racial misclassification was not an issue in their research because of how their data were obtained. Lee et al. linked the Florida Cancer Data System with the Florida Agency for Health Care Administration and identified AI/AN patients through insurance payer information. 64 If patients indicated that the IHS was their insurance provider and that they received care from IHS facilities, they were included in the AI/AN group. The data collected in this study were not linked with IHS directly and therefore likely included a substantial level of misclassification. Both Baquet et al. and Schiff et al. noted the relative lack of racial misclassification in the New Mexico SEER Registry, because of the practice of the registry to link with IHS before publishing data, and, therefore, it was not an issue in either study.38,82
CONSIDER Statement Results
Among the 66 articles, the average number of CONSIDER checklist domains was three, with a range of zero to eight domains included (Table 2). The domain most often identified was Prioritization (60), followed by Governance (47), Methodologies (31), Dissemination (27), Relationships (22), Participation (9), Capacity (9), and Analysis and Findings (8). Only two articles met the criteria for each of the eight domains.89,98 The articles by Creagan et al. and Qian et al. did not meet any criteria for any of the domains.46,79 Regarding Governance, a total of 47 of the 66 (70%) articles met the criteria.5,6,33,37,39,41,43–45,47,49–55,57–59,61,63,67–69,73–76,78,80–83,85–98 Articles that met the criteria for the Governance domain described agreements between research institutions and Indigenous-governing organizations for research and/or specified protection of Indigenous intellectual property and knowledge arising from the research. A total of 60 of the 66 (90%) articles met the criteria for the Prioritization domain.5–7,33,38–45,47–63,65–72,74–78,80,82–98 The research from those articles explicitly stated how the research aims emerged from priorities identified by Indigenous stakeholders, governing bodies, and/or empirical evidence. A total of 22 of the 66 (33%) articles met the criteria for the Relationship domain.33,37,39,41,43,44,47,61,67,73,74,78,80,83,85,86,89,90,93,94,96–98 These articles either worked with Tribal or Native entities for the research, or they were established members of the research team. A total of 31 of the 66 (46%) articles met the criteria for Methodologies domain.5,33,37,39–45,47–50,52,53,61,64,67,72,74–76,78,81,85,87–91,97,98 These articles described the rationale of methods used and implications for Indigenous stakeholders and/or incorporated impacts of colonialization, racism, and social justice as part of the discussion and results. A total of 27 of the 66 (2%) articles met the criteria for the Dissemination domain.5,7,33,40,41,47,49,51,53,56,60,61,67–69,73–76,78,85,86,88–90,97,98 These articles stated the relevance of the findings to relevant Indigenous governing bodies and peoples and/or implementation strategies. A total of 9 of the 66 (1.5%) articles met the criteria for the Participation domain.33,42,47,67,83,88,89,98 These articles discussed how data were obtained and stored. A total of 9 of the 66 (2%) articles met the criteria for the Capacity domain.33,37,39,61,78,85,87,89,97,98 These articles described if research teams participated in professional development to partner with Indigenous stakeholders and/or described experiences with Indigenous research capacity. A total of 8 of the 66 (1.5%) articles met the criteria for the Analysis and Findings domain.33,67,78,83,85,88,89,98 These articles specified how the research analysis and reporting support the research aims.
CONSIDER Checklist Domain Results, n = 66
Oral Cancer-Specific Results
Results related to oral and pharyngeal cancers were extremely limited. Among 66 articles included for final analysis for this systematic literature review, one identified oral cavity and pharynx cancer as the cancer-focus of the study. 80 The objective of the article was to determine the incidence rates for individual anatomical sites for cancers of the oral cavity and pharynx for the six IHS regions between 1999 and 2004 for AI/AN populations. 80 Furthermore, the authors conducted matching of NPCR and SEER data with the IHS health database to account for misclassification and analyses focused on Contract Health Service Delivery Area (CHSDA) counties. 80 The results indicated a lower incidence rate for all cancers of the oral cavity and pharynx combined for AI/AN populations in CHSDA counties compared with non-Hispanic White populations (8.5 vs. 11.0). 80 The authors also indicated that analyses by individual anatomical cancer sites and/or by IHS geographic regions suggest varied results. 80
Discussion
It is vital to ensure accurate data collection of race/ethnicity data in all health registries and databases to effectively monitor cancer trends and subsequently address cancer health disparities for minoritized populations in the United States. The gold standard for identifying cancer type is the cancer registry, which is based on medical records data. 31 Conversely, self-reported race and ethnicity are the gold standard for capturing such information and also align with federal standards for reporting such characteristics. 31 One study investigated the concordance between cancer registry and self-reported data regarding cancer type, race, and Hispanic ethnicity in a large, geographically diverse population from state cancer registries, including SEER and non-SEER regions in the American Cancer Society’s Studies of Cancer Survivors. 31 Using the Study of Cancer Survivors-I (SCS-I) and SCS-II found strong concordance for White and Black survivors and weak concordance for AI/AN and Asian/Pacific Islander survivors. 31 As members of the AI/AN populations are often misclassified in medical records by hospital personnel, it is imperative to use tools to improve accuracy such as annual linkage with the IHS. The advantage of using data linked with the IHS records is that patients receiving care from the federal agency are confirmed as AI/AN through membership of a federally recognized tribe. However, this linkage does not resolve all racial misclassification in health data. There are AI/AN patients not currently receiving or have never received care through the IHS or those who are members of a nonfederally recognized tribe that may be subject to misclassification.
In a publication by the CareQuest Institute for Oral Health in partnership with several tribal organizations, the authors provided suggestions on how to improve data quality in the collection and reporting processes. 3 Owing to the small size of the population, many researchers misclassify AI/AN data as “other,” which obscures and skews the data regarding the entire population. To address this, the Urban Indian Health Institute suggests oversampling the AI/AN population, allowing participants to choose multiple races and ethnicities that best represent them, aggregating data over longer periods of time, and weighted sampling. Data linkages improve data quality and data integrity, but if data linkage is not available for specific health topics, then the above recommendations must be considered.
An example of real-world data linkage practices and advancing community voices and health equity can be seen at the Public Health Agencies in the state of Oklahoma, such as the Oklahoma State Department of Health and the Oklahoma Department of Mental Health and Substance Abuse Services. These state departments have been keenly aware of the issue of racial misclassification and its impact. These agencies have special tribal-liaison divisions that work closely with the SPTHB to address the issue. Great strides have been made at acknowledging the issue exists; however, much work remains in tackling sources of misclassification considering the systemic nature of the problem. It is impossible to say how many systems a record passes through before the final data point. Each one of these systems presents the opportunity for racial misclassification. Optimistically, these agencies are extremely collaborative and partner with the SPTHB in conducting regularly convening workgroups. Even specific divisions within these agencies are willing to disseminate corrected datasets. A real opportunity exists as the Oklahoma State Department of Health recognizes the issue of racial misclassification and is proactive in seeking enhanced-linked datasets. States generally wait for the CDC to conduct the linkages; however, Oklahoma proactively sends its mortality files and requests the linkages directly. 99 Oklahoma is also the only state that has an online data query system with these linked data. 99 Although the issue of racial misclassification is incredibly profound, Oklahoma recognizes this and is proactively seeking solutions. Through collaborations and workgroups, we have seen that as awareness spreads, professionals are open and incredibly eager for solutions.
Through partnerships with other Tribal Epidemiology Centers, the SPTHB has learned that racial misclassification is an issue they, too, are working to tackle. These Tribal Epidemiology Centers often share information and support as they work to help better their communities. The SPTHB has worked closely with the United Southern and Eastern Tribes and the National Council on Urban and Indian Health on actions for tackling racial misclassification. There has been tremendous collaboration, cooperation, and output from these partnerships. The SPTHB plans to leverage these and other partnerships to implement systematic change not just to mitigate racial misclassification once it has occurred but to reduce the incidence of it.
Nonetheless, it is important to acknowledge that the concept of race, especially for public health and medical research is, and has historically been, convoluted, complex, and at times problematic. The collection of race information for the purposes of research with the aim of categorizing various population groups has led to the marginalization of groups of people, owing to the intricacies of such categorization and historical factors. For example, the concept of race arose in the late seventeenth century, with the rise of the transatlantic slave trade, and was even used to justify slavery with groundless, racist notions such as biological inferiority.100–102 Furthermore, race is a social construct based on numerous secondary physical features such as skin color, and despite extensive scientific research in opposition, there is still the unsupported belief that “race,” reflects fundamental biological differences.100,102 In addition, and adding to the complexity, AI/AN is a political identity. In the 2020 publication of Data and Native American Identity, author Kimberly R. Huyser (2020) explains:
Ultimately, the American Indian and Alaska Native identity is inherently political. It is political through the formal enrollment and connection to Native Nations. For federally recognized tribes, this also confers a government-to-government relationship between the U.S. federal government and the tribal government. Thus, the complex nature of Native identification necessitates the importance of a multidimensional measurement of race— self-reported race, socially assigned race—and questions about the connection to a Native Nation or Native community. The connections to an American Indian or Alaska Native community should be tailored for each community that tap into mechanisms of mutual acknowledgment. 103
Furthermore, in Morton v. Mancari, the Supreme Court established that AI/ANs can be treated differently from other U.S. citizens by the federal government even though there are antidiscrimination laws.104,105 The Court held that if the law or action is based on long-standing legal responsibilities toward AI/AN interests and promotes tribal self-governance, members of tribes should be considered as political groups as opposed to racial groups.104,105 This indicates that under the trust doctrine when members of Indian tribes receive special treatment from the federal government under the Affordable Care Act (ACA), treatment cannot be considered racial discrimination because tribes are considered political groups, not racial groups. 102 So, the question is, if widely recognized as a political designation rather than a race category, would that change how AI/AN data are collected and shared?
Since the last treaties were signed in 1871, AI/AN populations have been burdened with inadequate access to health care resources and services.106,107 AI/AN health disparities in the United States are a social justice issue that should be recognized as a national priority to increase resources and services for this population. Clearly, there are educational gaps in both the fields of public health and medicine in accurately reporting self-reported race/ethnicity and accounting for misclassification in research analysis. Such topics should be at the forefront of educational curricula. Furthermore, promoting equitable research should also be at the forefront. Incorporating the CONSIDER statement was an intentional use of an Indigenous framework to strengthen research and advance Indigenous health outcomes. Future research should be led by and in partnership with Native researchers and organizations. When researchers and health clinicians are of diverse racial and ethnic backgrounds, this advances health equity work.
Limitations
Limitations to this study include that most were retrospective observational studies, for which missing data are inevitable. Outcomes evaluated were limited to published articles and in the English language only. Regarding the CONSIDER criteria, some of the domains are difficult to establish such as Native researchers might be members of the team but not work for a tribe or tribal serving organizations.
Conclusion
Cancer surveillance data represent real patients in the United States and should accurately reflect their identities. Adherence to self-reported race/ethnicity in data collection for research and health information is essential to understanding racial health disparities especially for many minoritized populations, such as AI/AN populations. The implications of the findings of this review are far-reaching, including how oral health data are related to cancer. Oral health is associated with cancer incidence and survival; however, misclassification adds another layer of complexity to understanding the impact of poor oral health. By using cancer data as an example, the impact of misclassification of race on AI/AN populations is evident. To ensure equitable representation of AI/AN communities, and thwart further oppression of minorities, specifically AI/AN peoples, is through accurate data collection and reporting processes. Data linkages improve data quality and data integrity.
Authors’ Contributions
J.S., A.J.L., and J.P. conceived the study. A.J.L., A.H., and J.E.C. completed the analysis. A.J.L. led the writing.
Ethical Approval and Consent to Participate
Ethical approval and patient consent were not required. This material is the author’s own original work, which has not been previously published elsewhere.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
Support for this research comes from the CareQuest Institute of Oral Health through their Advancing Equity through Oral Health funding initiative.