
Abstract
Introduction:
In an attempt to address health inequities, many U.S. states have considered or enacted legislation requiring antibias or implicit bias training (IBT) for health care providers. California's “Dignity in Pregnancy and Childbirth Act” requires that hospitals and alternative birthing centers provide IBT to perinatal clinicians with the goal of improving clinical outcomes for Black women and birthing people. However, there is as yet insufficient evidence to identify what IBT approaches, if any, achieve this goal. Engaging the experiences and insights of IBT stakeholders is a foundational step in informing nascent IBT policy, curricula, and implementation.
Methods:
We conducted a multimethod community-based participatory research study with key stakeholders of California's IBT policy to identify key challenges and recommendations for effective clinician IBT. We used focus groups, in-depth interviews, combined inductive/deductive thematic analysis, and multiple techniques to promote rigor and validity. Participants were San Francisco Bay Area-based individuals who identified as Black or African American women with a recent hospital birth (n=20), and hospital-based perinatal clinicians (n=20).
Results:
We identified numerous actionable challenges and recommendations regarding aspects of (1) state law; (2) IBT content and format; (3) health care facility IBT implementation; (4) health care facility environment; and (5) provider commitment and behaviors. Patient and clinician insights overlapped substantially. Many respondents felt IBT would improve outcomes only in combination with other antiracism interventions.
Health Equity Implications:
These stakeholder insights offer policy-makers, health system leaders, and curriculum developers crucial guidance for the future development and implementation of clinician antibias interventions.
Introduction
The United States has poorer maternal health outcomes than peer countries and substantial racial and ethnic inequities among them.1–7 Black women and birthing people in the United States, for example, are approximately three times more likely to die from a pregnancy-related cause than white women and birthing people, and experience significantly higher rates of severe maternal morbidity (e.g., preeclampsia, preterm birth) and neonatal mortality.7–10 This elevated risk, deriving from historical and contemporary manifestations of structural and interpersonal racism,11–13 exists across the socioeconomic spectrum.14–16 Women and birthing people from historically oppressed populations in the United States report higher rates of mistreatment during pregnancy and birth than white individuals, and report disrespectful, disempowering, and coercive interactions with perinatal care providers.17–22 These unjust and preventable 23 inequities persist even in states where aggregate outcomes have improved.21,24–27
Recognizing the threat of implicit bias to patient care and outcomes,28–33 25 states and Washington DC have since 2019 introduced, and 6 have passed, legislation requiring implicit bias training (IBT) for health care workers. 34 The California legislature enacted the “California Dignity in Pregnancy and Childbirth Act,” effective January 2020 (“The Act”). 35 Among its core components is the requirement that all clinicians providing perinatal care at hospitals, licensed alternative birth centers (ABC), or primary care clinics providing ABC services undergo evidence-based IBT every 2 years, addressing 10 specific foci (Supplementary SA). 35 Many California facilities have directed providers to new or existing self-administered online trainings to fulfill these requirements. 36 The Act does not identify a responsible entity to guide training implementation nor monitor compliance.
Notably, little evidence exists that IBT can change providers' clinical practice or patient outcomes.29,37–41 Some antibias interventions have been shown to reduce individuals' awareness of, level of, and/or motivations regarding their biases.42–44 However, antibias intervention effects are typically short-term, modest, have little effect on behavior, and do not occur consistently across settings.45,46 These patterns appear to be similar within and outside of health care contexts,31,38,40 reflecting an “irony that implicit bias training as currently envisaged might not be an effective or realistic approach to rectifying the negative effects of implicit bias.”39(p.1458)
In light of growing state and health care system IBT requirements,34,47 it is crucial to identify features of antibias interventions that may enhance their ability to improve care and patient outcomes.29,47,48 Engaging the lived experiences and insights of key stakeholders—in California, the Black women and birthing people whom the Act was designed to benefit, and the perinatal clinicians who will take IBT—is a critical way to access these insights.49,50 We describe these stakeholders' perspectives regarding the challenges and recommendations for impactful clinician IBT.
Methods
With community collaborators and interdisciplinary researchers, we conducted a descriptive 51 multimethods community-based participatory research (CBPR) study. Community collaborators (L.J., J.H-T., H.F.Y., B.P.), themselves IBT patient and advocate stakeholders, codesigned and provided sustained guidance on recruitment materials and strategy, data collection instruments, analysis, and presentation of results.
Focus groups
We recruited individuals who received prenatal care, delivered a baby, and/or received postpartum care in a hospital in the San Francisco Bay area in 2019, 2020, or 2021. We advertised primarily via California birth equity-focused social media and fliers at large community clinics. We held five 90-min Zoom-platform focus groups (FGs) between August and November 2021 (3–7 participants per group). Participants received $75 for participation. A community collaborator with substantial CBPR expertise (L.J.) facilitated the FGs while a sociologist with substantial qualitative research expertise (S.B.G.) assisted and took analytic notes. The pair debriefed after each event to discuss content and data quality and finalize notes.
Interviews
We recruited perinatal clinicians from two San Francisco Bay Area hospitals (community, safety-net), purposively sampling for variation in unit role and self-identified demographics. S.B.G. conducted semistructured in-depth interviews with each participant via phone (44–80 minutes; mean=56).
In both FG and interview engagements, we provided a written and verbal overview of the Act to ensure that participants had the same baseline knowledge of the legislation, its intent, and requirements (Supplementary SA). In addition, both formats of data collection focused on what factors would hinder or support impactful IBT, which we defined as IBT “that could improve care and clinical outcomes for Black women and birthing people.” We used a variety of prompts to thoroughly investigate these topics (Supplementary SB, and SC). S.B.G. took analytic notes in each engagement, specifically documenting what respondents said about factors that did or could hinder or support IBT's ability to advance birth equity. She verbally presented notes back to participants at the conclusion of each engagement to facilitate the correction, clarification, or addition of data.
With respondent permission, we digitally recorded FGs and interviews and had them professionally transcribed. (See Supplementary SD for additional methods information.) The UC San Francisco Institutional Review Board approved study activities; all participants provided verbal consent.
Analysis
Following best practices, iterative combined inductive/deductive thematic analysis began and continued throughout data collection.52,53 The lead researcher added contextual and analytic notes to the notes participant-checked during interviews/FGs. Community collaborators (L.J., J.H., B.P., H.F.Y.) and S.B.G. discussed notes and transcript excerpts across numerous meetings to evaluate whether the study was capturing adequate data, to refine the data collection instruments, and to develop early familiarity with the data.
Upon conclusion of data collection, S.B.G., E.C., and S.Z. reviewed the full corpus of data for familiarity. In ATLAS.ti, we used a first round of codes to identify excerpts where participants described challenges, opportunities, or recommendations for implementing or achieving impactful IBT. In multiple meetings, SBG discussed segments of these data with community collaborators to check interpretation and to collectively identify and refine themes. S.B.G. developed a thematic coding scheme to characterize challenges and recommendations for implementing and achieving impactful IBT. S.B.G., E.C., and S.Z., and community collaborators reviewed the schema to evaluate its comprehensiveness and accuracy; collectively and iteratively refined its categories; and resolved disagreements via verbal and written discussion. S.Z. and E.C. applied these codes to the data in ATLAS.ti, which we used to extract relevant data and illustrative quotes. We present themes organized into five domains.
Results
Sample description
All FG participants (“patients”; n=20) identified as Black women, with 1 reporting additional racial identities (Table 1). Most patients were non-Hispanic/Latinx; had Medicaid insurance coverage; found it “somewhat” or “very” hard to pay for basic needs; and had a hospital-based delivery in 2020 to 2021. Interviewees (“clinicians”; n=20) were nurse midwives (n=6), physicians (n=6), registered nurses (n=5), or other staff (n=3). They self-identified as Black (n=4), multiracial (n=4), or white (n=12) women; two identified as Latinx or Hispanic women.
Study Participant Characteristics
Participants were given the option to select “Other” as a racial designation. They were invited but not required to provide further information.
CNM, certified nurse-midwife; RN, registered nurse.
Challenges to and recommendations for impactful IBT
Patients and clinicians raised many of the same factors that they believed threatened (challenges) or should be addressed to improve (recommendations) IBT effectiveness (Table 2). We highlight substantive differences when relevant. Identifying labels are provided to indicate the patient focus group (FG) or clinician interview (CA or CB), from which quotations are drawn (Table 3).
Topics Represented in Respondents' Discussions of Challenges to or Recommendations for Effective Implicit Bias Training, by Respondent Subsample
“x” denotes that one or more participants in the column subsample reported a challenge or recommendation related to the row topic.
IBT, implicit bias training.
Recommendations for Impactful Clinician Implicit Bias Training (IBT): Illustrative Quotations from Patient and Clinician Stakeholders
“FG” denotes focus group participants: Black women who had been a patient in maternity care services. “CA” and “CB” denote interview participants from two facilities: multidisciplinary hospital-based perinatal clinicians.
Domain 1: State law and policy
Both patient and clinician stakeholders referenced aspects of state law and policy in their discussions. Clinicians expressed concerns that the scope of providers required to complete IBT is insufficient, citing the breadth of nonperinatal providers who interact with pregnant individuals. Requiring only perinatal providers is “changing one last step” in the pregnancy journey (CB01). Both clinician and patient respondents recommended expanding requirements to include a broader range of health care providers and staff, including outpatient settings.
Both groups were concerned about the Act not requiring enough detail, specificity, or intensity of training—gaps that many participants addressed in recommendations for IBT design and implementation, below. Patients were particularly interested in making IBT more frequent and specifying the minimum number of hours of training to ensure a level of intensity and comprehensiveness.
Some stakeholders, particularly patients, identified the lack of enforcement or accountability mechanisms in the Act as a challenge. Patient participants recommended that IBT and antibias performance be linked to standards, penalties, or hospital funding, without which, IBT “won't change a thing” (FG05). Patients also recommended that funding be built into future policy to support more comprehensive antibias education.
Domain 2: IBT content, format, and other qualities
Much of participants' discussion centered on challenges and recommendations for antibias training itself. Many participants expressed doubts that IBT could change clinician practice or deeply held biases (“You are who you are”; FG04), describing the influence of online IBT “like a drop in the bucket” (CA06). The majority of respondents also raised concerns that IBT was unlikely, on its own, to improve clinical outcomes for Black women and birthing people. Concerns focused on the training addressing a fraction of the problems that produce health inequities; that systemic factors, of which clinician bias is a part, will take generations to change; and that without systemic change, the training will have little power.
Content
Patients, and to a greater extent clinicians, shared concerns about IBT being superficial, repetitive, or overly simple: “It's different from fire safety. It's more nuanced” (CA09). Others felt trainings that were “generic” (CB10) and not specific enough to providers' patient population limited their impact. Patients and providers recommended that training provide a holistic treatment of racism, biases, mistrust, and inequities in U.S. medicine, although some felt that a better understanding of “racism as a whole” would have to precede this (FG02). Others suggested IBT include “powerful statistics” (CB03) that could demonstrate that racism, not race, underlies inequities. Many respondents recommended that IBT incorporate tailored information to connect it to the facility and community served (e.g., regarding patient experience, case studies, staff knowledge of racial disparities).
The majority of clinicians as well as some patients supported the use of real patient stories or narratives to make IBT impactful. Recommendations included narratives of what biased care feels like, of providers causing harm, and stories that ensured the experiences of Black women and birthing people, in particular, are “memorable” (CB08) and “real” (CA06) to IBT trainees.
Many clinicians felt IBT would be ineffective if their peers did not find it credible or relatable; if providers could not connect to the effort, they would not engage with it. Some had seen colleagues dismiss or become closed off to IBT. Clinician-respondents in particular recommended that training meet these challenges by fostering clinician reflection and introspection to understand bias in themselves (“make it personal,” CB06) and highlighting the ways reducing bias could improve clinical care.
Format
Participants from both groups, but particularly clinicians, highlighted the limitations of online self-administered training for changing biases and behavior. Multiple participants described such training as just a “box to check off” (e.g., FG04, CA05); one where distracted individuals could “click until it's over” (CA06) and not learn. “It's such a terrible platform for learning” (CB09). In response to this, many clinician-respondents recommended more interactive formats, featuring opportunities for colleagues to give and receive feedback, learn from each other, and be vulnerable and honest. Participants varied regarding what such sessions should look like (e.g., small group in-person versus online interactive sessions; interprofessional groups versus single-group trainings). A few clinicians also noted, however, that noninteractive trainings might better suit individuals for whom the stress or self-consciousness of interactive sessions would distract from their learning.
Other
Clinicians additionally discussed the limitations of IBT that lacked application to providers' day-to-day practice. Many expressed frustration that they were not learning strategies to use in clinic or hospital-based care. “Okay. I'm aware. So, what do I do from that?” (CA03). Both clinicians and patient respondents recommended that IBT integrate practical skills-building to make it “relevant, not theoretical” (CA10). Concrete examples included how to handle drug use conversations, patient disagreement on recommended treatment options, and other challenging clinic scenarios via strategies such as role playing, immersive/experiential teaching, and nonviolent communication. Regarding training frequency, multiple patient respondents felt that every 2 years would not be sufficient for changing behavior. Participants from both groups recommended training be implemented more frequently than dictated by law.
Domain 3: Health care facility IBT implementation
Participants, particularly clinicians, raised a number of challenges and recommendations related to the implementation of IBT in hospitals. Clinician-respondents were concerned that facilities could, for example, adopt an ineffective curriculum or engage trainers who were insufficiently committed or credible. Clinician-respondents recommended that facilities engage trainers whom providers respect and/or perceive as appropriate for the role, including individuals from affected communities; others recommended professional external trainers. Patients, but particularly clinicians, recommended that facilities work to create a supportive environment for IBT. They called for “safe” (CB06), “nonjudgmental” (CB03) training spaces that allowed for participant privacy and were free of shaming and defensiveness.
Some clinicians felt that logistics, time pressures, and competing responsibilities—including numerous other trainings—would impede IBT or make it more burdensome. “We are so overworked right now… It's hard to find any extra time for anything” (CB08). Others reported that insufficient funding for antibias work exacerbated these problems and limited facilities' access to more impactful training options. Clinicians recommended facilities provide protected and paid time/coverage for IBT and ensure participant receipt of continuing education credits for it.
Some clinician-respondents expected that the lack of evaluation of IBT effects would limit its impact. Both patients and providers recommended that facilities use data (e.g., pre-/post-assessments; patient experience reporting) to evaluate if IBT is improving care and outcomes for affected communities; and/or to guide and refine future training.
Domain 4: Health care facility environment of IBT
Patient and clinician participants also discussed challenges and recommendations related to the broader facility context in which training would take place. Some were concerned about leadership decisions, commitment, and communications about IBT. Some patients, for example, were concerned that hospital leaders could have the same biases IBT seeks to reduce, limiting leaders' support of training. Clinicians expressed concerns about rushed timelines and leaders who do not communicate the importance of IBT to staff. They recommended that leadership work to foster legitimacy and demonstrate commitment by allowing IBT appropriate time, fostering staff buy-in, and emphasizing its importance. Many participants recommended that facility leadership implement the policy- and training-focused recommendations described above (Domains 1–3).
Clinician respondents were particularly concerned about aspects of clinic culture and interpersonal dynamics that could limit the power or application of IBT. For example, several described that staff may not feel safe enough to let themselves be vulnerable in conversations about bias; or that hierarchies in the workplace inhibit discussion and critical feedback. Clinicians recommended the creation of spaces for antibias discussion and growth outside of training; fostering trusting relationships among staff; and developing a no-tolerance approach to bias and racism.
Primarily patients raised issues of accountability within the facility. They cited concerns that participation and change are unlikely without enforcement and that health care workers not required to take IBT may not participate. Patients in particular called for facilities to develop systems to be accountable for implementing IBT, and to hold themselves and providers accountable for providing unbiased care (e.g., vis-à-vis patient experience data, complaints). Other recommendations included patients being informed about providers' antibias training status and staff receiving supplemental training and, ultimately, penalties, if they continue to provide biased care.
Both groups shared concerns that antibias efforts could end up on the “back burner” at facilities (CB06). Recommendations included facilities providing digital and physical antibias reminders and creating regular unit-wide opportunities for complementary learning (e.g., discussions about bias and dignity in care; case reviews).
Domain 5: Provider commitment and behaviors
Finally, participants expressed that IBT effectiveness would be limited for providers who are insufficiently motivated or committed to IBT, or who do not participate in a “wholehearted” way (CB07). Some felt that this was particularly likely for online-only IBT. Others were more concerned about colleagues’, teams’, or leaders' lack of commitment to antibias/antiracism change more broadly, which could dampen the impact of IBT in the unit. Patient and clinicians recommended providers work to take the training seriously and “have an open mind” (FG03). Participants described providers not recognizing their own biases or their need to change as barriers to effective IBT. “I think it's super easy to be dismissive of the training … “Yeah, yeah, the racist people of the world need this but, like, I don't” (CA05).
In addition to impeding training effectiveness, such denial can produce defensiveness among clinicians, which multiple respondents felt could cause them to “shut down” or react negatively to the training. To counter these challenges, many participants recommended that clinicians work to develop self-knowledge of their biases, for example, via reflection and discussion, described above.
Finally, a small number of patients and clinician stakeholders referenced potential unintended effects of IBT as a challenge. One FG participant, for example, described that providers “overeducated” in IBT could think that they know what patients need before patients tell them or could feel more entitled to “police” Black women (FG01). A clinician feared that IBT could contribute to burnout if it does not clearly serve the core mission of providing health care.
Stakeholder expectations
Many participants expressed skepticism about IBT's effectiveness and felt that significantly reducing inequities in maternal care outcomes would only be achieved with multilevel interventions. Closed-ended questions asked at the end of these discussions reflected modest expectations. Most respondents expected that the training would decrease maternal morbidity and mortality, or improve relationships between clinicians and Black women and birthing people, “a little or somewhat” (Fig. 1). However, nearly all participants indicated that they wanted their provider to take IBT (patients) or that they themselves wanted to take it (clinicians). In the words of one participant, “I think the only outcomes [of IBT] would be either positive or nothing changes. And if it changed one Black woman's life, then it's all worth it” (FG02).
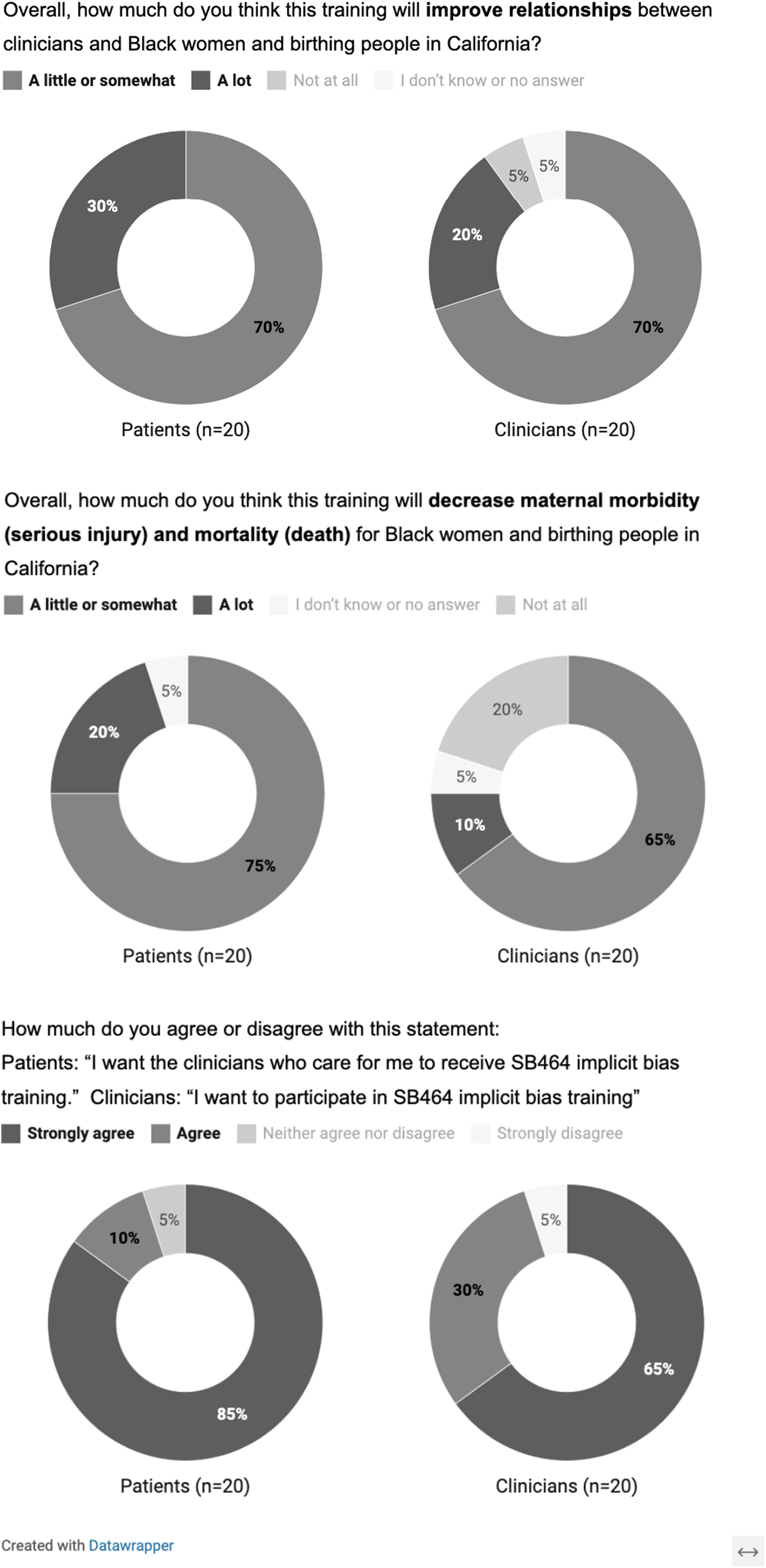
Patient and clinician opinions regarding the impact and desirability of implicit bias training. These graphics depict the proportion of respondents in each group that endorsed the presented survey responses to three opinion questions. Surveys were conducted at the conclusion of each data collection encounter.
Discussion
Patient and clinician stakeholders in the San Francisco Bay Area identified numerous challenges and actionable recommendations for IBT regarding aspects of (1) state law and policy; (2) IBT content and format; (3) health care facility IBT implementation; (4) health care facility environment; and (5) provider commitment and behaviors. We note that some factors presented as a challenge in one domain may be addressed by a recommendation in another. Patient and clinician insights overlapped substantially. Patients, however, focused more on aspects of state policy change than clinicians (e.g., IBT funding, intensity of training) and on the importance of accountability/enforcement in state policy and health systems.
Clinicians focused more on facility-based considerations (e.g., training logistics, clinic culture) and enhanced IBT features such as greater interactivity and use of real patient stories. Importantly, participants from both groups reported that IBT would improve the care and outcomes of Black women and birthing people only in concert with other system-focused equity interventions (e.g., workforce diversification; more accessible high-quality prenatal care).
Findings from this study align with some research and expert opinion on best practices for IBT. For example, participants underscored the importance of IBT that encourages critical reflection, builds skills, and avoids shaming.30,47,54,55 They also expressed the need for iterative, ongoing training to reduce implicit biases.30,37,47 Extending beyond typical IBT, they recommended evaluating the training's effect on patient experiences and outcomes29,30,36,40,47; improving the unit's interactional environment30,46,56; and complementary antiracism changes to the health care system.29,33,36,40,57,58
Our study yielded novel findings as well. Participants, particularly clinicians, stressed going beyond generic case studies to include real data from their patients, facilities, and colleagues. This may be a compelling way to foster perspective-taking – a component found to reduce bias in some populations.32,38,54 Patient stakeholders in particular recommended that IBT policy include robust accountability systems, involving people with lived experience of biased care, to strengthen the development, implementation, enforcement, and evaluation of trainings. These echo recommendations made by California birth equity advocates as well. 36 The differences between our findings and typical IBT approaches likely reflect the unique wisdom of stakeholders and their focus on maternal health outcomes rather than on shorter-term attitudinal outcomes prevalent in IBT scholarship.
The findings have important and transferable 59 implications for clinician IBT. First, state lawmakers have the opportunity to address many of the challenges stakeholders identified by integrating clear governance, monitoring, evaluation, and appropriate resources into IBT policy; and specifying more IBT features that stakeholders recommend (e.g., skills-building; site-specific content; live interaction). Specific action steps for policy-makers, codeveloped with multilevel IBT stakeholders and policy experts, are available elsewhere. 60 Second, many California hospitals have utilized online, self-administered IBT curricula. Although thoughtfully designed, 61 their format, intensity, and/or content do not currently match many stakeholder recommendations presented here. Even without a legal mandate, public and private funders, IBT curricula developers, and health care leaders should work collectively to integrate more stakeholder-endorsed components into future IBT offerings, then rigorously evaluate and refine these approaches. 41 Mitigating qualities of health care settings known to exacerbate the effects of clinician bias (e.g., understaffing, time pressure) could additionally further antibias reduction.32,54,62
Health equity implications
Evidence-based IBT is one of many interventions needed in our national effort to reduce maternal health inequities.63–65 As with all health equity interventions, it will be most successful if designed with the robust and ongoing input of the individuals closest to the problem.49,50,66,67 For clinician IBT, this means engaging the Black women and birthing people from communities disproportionately burdened by maternal health inequities—to assess whether the intervention can meaningfully improve their care experiences and outcomes—and the clinicians, to assess whether the intervention will be feasible, sustainable, and impactful in their workplaces. With the growth of clinician IBT requirements, it will be crucial for stakeholder wisdom to guide future efforts.
Strengths and limitations
This study centered stakeholders in both its research and operations. Study leadership and collaborators included community stakeholders, and the study sample represents diverse members of key IBT stakeholder groups, thereby capturing an important range of views and experiences. However, study respondents were based in a single region—California's Bay Area—and did not include ABC clinicians. Preliminary survey research has indicated that current and former health care workers outside of our study region largely support recommendations reported here. 68 However, future studies should thoroughly explore stakeholder priorities and realities in other settings.
Conclusion
Patient and clinician stakeholders identified numerous challenges to IBT improving care and clinical outcomes for Black women and birthing people. Recommendations spanned several domains, reflecting the multilevel work that will be required to advance maternal health equity. Stakeholder-identified challenges and recommendations represent crucial insights for the development and implementation of health equity interventions. Lawmakers and health system leaders should leverage these and other stakeholder insights in IBT decision-making.
Footnotes
Acknowledgments
We are deeply grateful to the patient and clinician participants of the MEND study for their time, energy, and wisdom.
Authors' Contributions
S.G.: conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; resources; software; supervision; visualization; writing—original draft; and writing—review and editing. L.J.: conceptualization; formal analysis; investigation; and writing—review and editing. A.M.: formal analysis; investigation; writing – original draft; and writing—review and editing. H.F.-Y.: conceptualization; formal analysis; and writing—review and editing. J.H.: Conceptualization; formal analysis; writing—review and editing. B.P.: conceptualization; formal analysis; and writing—review and editing. E.C.: data curation; formal analysis; methodology; and writing—review and editing. S.Z.: data curation; formal analysis; methodology; and writing—review and editing. S.H.: conceptualization; formal analysis; investigation; and writing—review and editing. B.D.C.B.: conceptualization; formal analysis; writing—original draft; and writing—review and editing.
Data Availability
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by UC San Francisco's California Preterm Birth Initiative. Dr. Garrett was additionally supported by the Agency for Healthcare Research and Quality (AHRQ T32HS022241); and National Institutes of Health (National Center for Advancing Translational Sciences through UCSF-CTSI KL2 TR001870). Dr. Chambers Butcher is supported by the National Institute on Minority Health and Health Disparities (K01MD015785, “Community Racial Equity Training and Evaluation of Current and Future Health Care Clinicians (CREATE) Study”). This article's contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH or AHRQ. Funding sources had no involvement in the study design; collection, analysis, or interpretation of data; writing of the report; or decision to submit the article for publication.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.