
Abstract
Background:
Due to its prevalence, gallstone disease is a major public health issue. It affects diverse patient populations across various socioeconomic levels. Socioeconomic and geographic deprivation may impact both morbidity and mortality associated with digestive diseases, such as biliary tract disease.
Aim:
The aim of this systematic review was to review the available data on the impact of socioeconomic determinants and geographic factors on gallstone disease and its complications.
Methods:
This systematic review was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The MEDLINE and Web of Science databases were searched by two investigators to retrieve studies about the impact of income, insurance status, hospital status, education level, living areas, and deprivation indices on gallstone disease. Thirty-seven studies were selected for this review.
Results:
Socially disadvantaged populations appear to be more frequently affected by complicated or severe forms of gallstone disease. The prognosis of biliary tract disease is poor in these populations regardless of patient status, and increased morbidity and mortality were observed for acute cholangitis or subsequent cholecystectomy. Limited or delayed access and low-quality therapeutic interventions could be among the potential causes for this poor prognosis.
Conclusions:
This systematic review suggests that socioeconomic determinants impact the management of gallstone disease. Enhanced knowledge of these parameters could contribute to improved public health policies to manage these diseases.
Introduction
Gallbladder and biliary diseases are a major public health issue, affecting >193 million people worldwide in 2019. 1 Furthermore, gallstone disease is the leading cause of hospitalization due to gastrointestinal concerns in Western countries.2,3
Gallstone disease encompasses many diseases ranging from asymptomatic gallbladder stones to acute biliary pancreatitis (i.e., biliary colic, cholecystitis, obstructive jaundice, or acute biliary cholangitis). 2 The overall prognosis is quite favorable, with an overall mortality rate <0.5% for gallbladder stones, but mortality rate can reach 20–50% for severe types of acute pancreatitis.4–7
The treatment of symptomatic gallstone disease is essentially based on surgical or interventional procedures such as cholecystectomy or endoscopic retrograde cholangiopancreatography (ERCP). 2 These procedures can be distributed with a certain heterogeneity over the territories and this geographic heterogeneity can condition the access to care. Similarly, medical expertise and offer can differ depending on the care center. Consequently, treatment decisions for the same disease can vary.
Among nonclinical determinants, socioeconomic and geographic deprivation could impact both morbidity and mortality of digestive diseases.8–12 Socioeconomic determinants and geographic factors are highly correlated. 13 However, the geographic factors that influence health are not limited to the material deprivation of the patient's neighborhood, but include determinants such as the distance between patient's home and the health center, the geographical distribution of health centers, and geographical distribution of medical experts.
The aim of this work is to conduct an exhaustive review of the literature that evaluates the impact of nonclinical determinants (socioeconomic or geographic inequalities) on the management and prognosis of gallstone disease and its complications (i.e., cholecystitis, acute cholangitis, acute pancreatitis).
Methods
Study selection
Articles included in the review were selected using MEDLINE and Web of Science databases using the following MeSH terms: socioeconomic status (SES), social classes, socioeconomic factors, poverty areas, health care disparities, health care access, pancreatitis, gallstone, cholelithiasis, acute cholangitis, cholecystitis, biliary tract diseases, ERCP, and cholecystectomy and the formula ([Social class OR Poverty areas OR Health care disparities OR Health care access OR SES OR Socioeconomic factors] AND [Pancreatitis OR Gallstone OR Cholelithiasis OR Acute cholangitis OR Cholecystitis OR Biliary tract diseases OR ERCP OR cholecystectomy]) NOT Cancer. Selection was restricted to English-language articles indexed from database inception to October 4th, 2021. We also excluded articles published before 1985.
The search retrieved 102 abstracts that were carefully reviewed by a gastroenterologist (B.D.) and an epidemiologist (O.D.) for clinical relevance. The bibliographies of all full text articles selected were manually searched to identify additional studies that might be relevant. The data extraction process was conducted by a B.D. and verified by an O.D.
Definition of SES
The definition of SES and its specific assessment varied significantly between articles. Its relevance could be deeply influenced by the country in which the study is conducted. Overall, we can distinguish between two main categories of indicators for SES:
- Some studies used unique and individual variables such as income, socioprofessional category, or insurance status. Studies based in the United States can include and examine race/ethnicity as a social determinant of health. These parameters are not considered in European studies. Studies considering only a race/ethnicity criterion without another variable were excluded. - Others used collective indicators such as ecological scores that combine different parameters that better assess the complexity of SES. These indicators do not reflect the patients' situations individually, but assimilate their situation to a collective index depending on their residential area. Some studies considered the hospital status and location, urban or rural residential area, or different country regions that can impact access to health care.
Inclusion criteria
We therefore considered the full text articles that studied the impact of income, insurance status, hospital status, level of education, area of residency, and/or deprivation index in gallstone diseases (gallbladder stones, biliary colic, cholecystitis, obstructive jaundice, acute biliary cholangitis, or acute biliary pancreatitis).
Exclusion criteria
Studies were excluded if they were unavailable in English. Poster or oral presentation abstracts not linked to full-text articles were also excluded. We excluded studies that exclusively considered race/ethnicity criteria. Indeed, race/ethnicity criteria are not registered in medical studies in the majority of countries, except the United States. This point can lead to difficulties of comparison between studies, especially between Europe and the United States. Second, although there is a strong correlation between race and SES, it has been shown that racial disparities in health status are due to other parameters than only social disparities. 14 Racial segregation can lead to difference in social/environmental exposures and in care access. Many confounding factors between race and SES exist. We also excluded studies on malignant diseases or acute pancreatitis without data on biliary pancreatitis.
Outcomes measures
Do socioeconomic determinants or geographic factors impact the risk of developing a gallstone disease?
Do socioeconomic determinants or geographic factors impact access to treatment for gallstone disease?
Do socioeconomic determinants or geographic factors impact quality of care for gallstone disease?
Do socioeconomic determinants or geographic factors impact the prognosis of gallstone disease?
Quality assessment
To elaborate this systematic review, we followed 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 15 The quality of the studies was evaluated using STROBE criteria. 16 The items on the STROBE checklist v4 were interpreted in terms of their appropriateness of design to answer the study question. Scores were summarized as 0–11=III, 12–17=II, and 18–22=I, with “I” representing the highest quality studies (Supplementary Table S1). Only the studies with sufficient estimated quality were kept for this review. The review was not registered.
Results
Study selection and characteristics
Finally, 37 suitable studies were identified for review: 20 based on populations from the United States, 5 from the United Kingdom, 3 from Taiwan, 2 from Italy, and 1 from Switzerland, South Korea, Argentina, China, Sweden, Canada, and the Netherlands (Fig. 1).
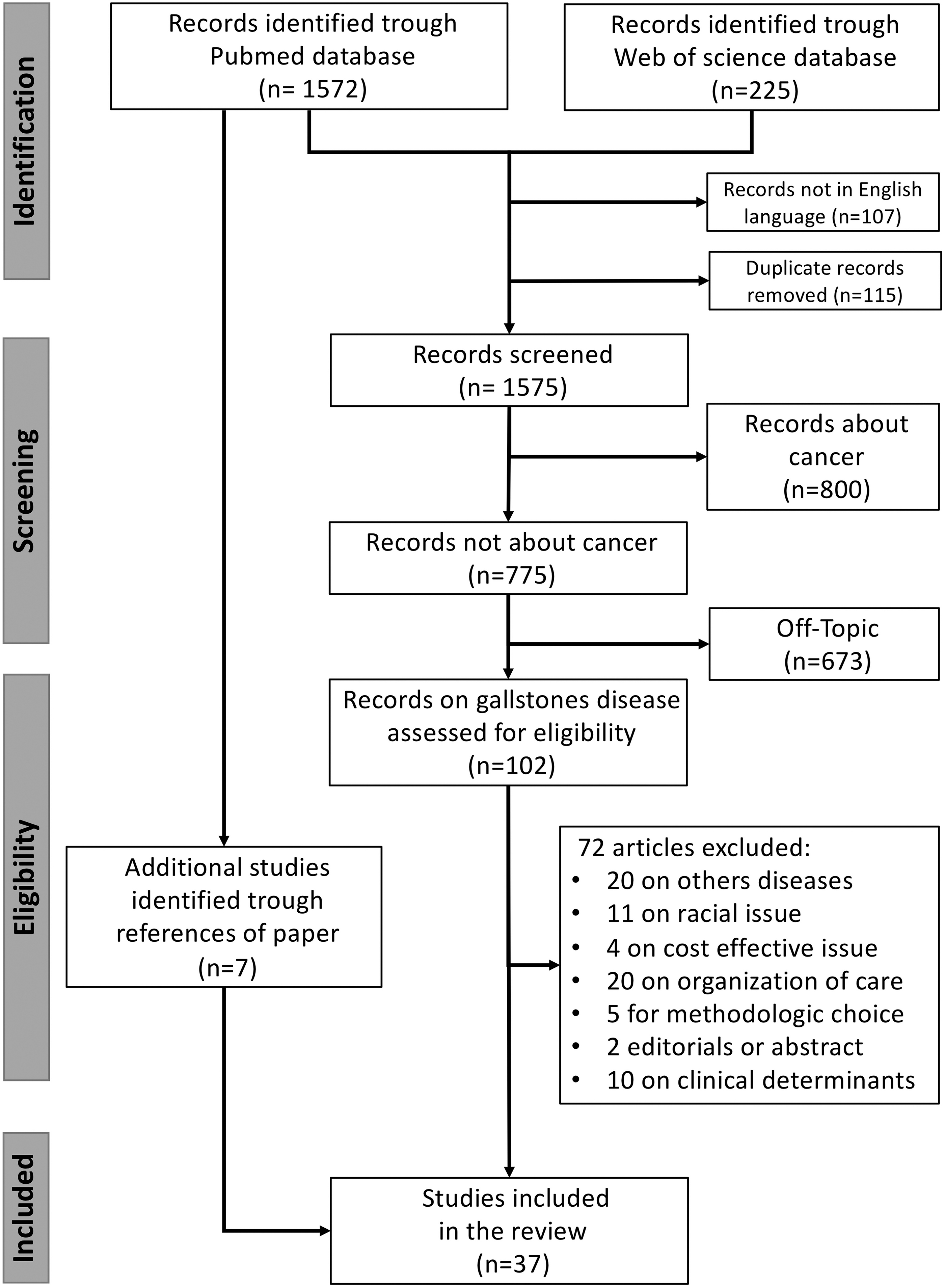
Flowchart describing the study selection process.
Table 1 shows the studies selected by summarizing the study period, its location, the number of included patients, the type of variable used to express the patients' SES, the disease or therapeutic intervention studied, and the main result of the study.
Studies Describing the Impact of Socioeconomic Status on Gallstone Disease
ACA, Affordable Care Act; ADI, area deprivation index; aOR, adjusted odds ratio; CI, confidence interval; CNI, community needs index; DCI, distressed communities index; ERCP, endoscopic retrograde cholangiopancreatography; GP, general population; GS/SP, Government-Subsidized/Self-Pay; HC, hospital charges; LIP, low-income population; LOS, length of stay; MA, Massachusetts; NCHS, National Center for Health Statistics; NHI, National Health Insurance; OR, odds ratio; PCP, primary care provider; RR, relative risk; SES, socioeconomic status; SVI, Social Vulnerability Index.
Given the heterogeneity of indices used to assess the patients' SES and the diversity of outcomes described in these studies, we were unable to perform a meta-analysis on this issue.
Do social determinants impact the risk of developing a gallstone disease?
Old data seemed to show a higher prevalence of gallstone disease in the most socially deprived patients. A study conducted in England in the 1990s showed a standardized consultation rate for gallstone disease >100%, which is higher than the expected proportion, in the most disadvantaged strata of the population; this finding suggests a possible overincidence, but without significant difference among the rest of the population. 17 One study shows an estimated relative risk (RR) of cholelithiasis substantially lower among highly educated people in comparison to patients with only primary school education (RR=0.65, 95% confidence interval [CI]: 0.56–0.75). 18
A case–control study aimed at identifying the risk factors associated with intrahepatic stones showed that a higher level of education lowered the risk of intrahepatic stones. 19 More recently, a study conducted in Jilin Province showed that patients with gallbladder diseases were more often from a rural area and had a lower level of education and lower income. 20 In a multivariate analysis, only living in a rural area was significantly associated with gallbladder diseases (odds ratio [OR]=1.65, 95% CI: 1.49–1.82). 20
A study conducted in South Korea over 30 years showed an increase in the proportion of gallbladder stones, following in the same proportions, the improvement in socioeconomic conditions in the country. 21 It is difficult to determine whether the increased prevalence of gallstone disease was due to an increased incidence of lithiasis or to an increased diagnosis correlated with an improvement in the performance and accessibility of paraclinical examinations such as ultrasound. Likewise, this study could not determine whether, at the individual level, social deprivation influenced the risk of gallstone disease. A case–control study indirectly questions the disproportionate risk of gallstone disease as related to SES. This study did not find any difference depending on the SES. 22 This work was not designed to truly answer the question of the incidence of gallstone disease according to the populations' socioeconomic determinants.
In the specific case of biliary pancreatitis, more robust data exist. Socioeconomic deprivation has been associated with increased incidence of acute pancreatitis.23,24 In a large British study of 10,589 cases of acute pancreatitis, Roberts et al 24 reported an incidence 1.9 times (95% CI: 1.8–2.0) higher in severely disadvantaged patients than in the highly affluent patients. This difference persisted when we considered only gallstone etiology (1.5, 95% CI: 1.4–1.7), even if it was more obvious for alcoholic acute pancreatitis (3.9, 95% CI: 3.4–4.5). 24 These data confirmed the results of a preliminary study from the same team 25 and of another earlier British study of 963 cases, which also found a higher incidence of biliary pancreatitis in severely disadvantaged people. 23
Overall, the data currently seem too limited to conclude the potential impact of socioeconomic determinants on the incidence of gallstone disease, except for biliary pancreatitis.
Do social determinants impact access to treatment for gallstone disease?
All the recent studies conclude that there is rather limited access to cholecystectomy for the weakest social categories. A Dutch study shows an impact of income level on the incidence of cholecystectomy without analyzing the cause of these differences. They report a decreased incidence in low-income women (0.87) and an increase in men (1.12). 26 After acute cholecystitis, it has been demonstrated that more patients with private insurance underwent cholecystectomy during the same hospitalization than patients with Medicaid (89% vs. 83%; p<0.001). 27 The time to access cholecystectomy is inversely associated with the level of education: patients with a low level of education had a 16.2% lower rate of access to surgery and a 13.5% longer waiting time. 28
This limited access to cholecystectomy for patients with a low SES is also illustrated through changes in cholecystectomy rates before and after health care reform in the United States. Before reform in Massachusetts in 2006, patients with government insurance and no insurance had 6.6% and 9.9% lower chances of having an immediate cholecystectomy after an episode of acute cholecystitis, respectively. The health care reform resulted in a 2.5% independent improvement of this probability in these same patients (p=0.049). 29
Conversely, the National Reform of 2014 allowed a reduction in emergency cholecystectomies (62.1–59.3% after the reform, p<0.01), an increase in the proportion of patients treated in teaching hospitals (45.4–60.4%; p<0.01), and an increase in patients receiving Medicaid (26.3–34.0%, p<0.001) inversely proportional to the decrease in self-pay patients (19.3–13.6%, p<0.001). 30 This decrease in the proportion of self-pay patients was also observed in a cohort study on cholecystectomies performed for benign gallbladder disease. 31 In addition, there was an increase in the proportion of outpatient surgeries (80.0% vs. 78.2%, p<0.001). 31
While it is clearly established that there is a benefit to perform cholecystectomy during the same period of hospitalization for nonsevere acute biliary pancreatitis, 32 the applicability of this recommendation is sometimes difficult. 33 A recent large-scale American study showed that the rate of same admission cholecystectomy for nonsevere acute biliary pancreatitis was higher in patients with private insurance (OR=1.1, 95% CI: 1.0–1.3). 34 Another U.S. study supports these results in concluding that Medicare payer status decreased the odds of undergoing same admission cholecystectomy after ERCP for acute gallstone pancreatitis. 35
Overall, after a complication (biliary colic, cholecystitis, or biliary pancreatitis), the likelihood of having cholecystectomy, as recommended, is lower in severely deprived patients. However, in patients previously hospitalized for gallstones treated with ERCP, the rate of early cholecystectomy (performed within 14 days after sphincterotomy) was significantly lower in populations of patients with high SES (41.3% vs. 48.4%, p=0.0134). 36 While these data should be interpreted with caution, they appear to show that once treated, patients from a severely deprived class follow the proposed treatments. The main explanation would be that the initial access to treatment is difficult. It is also possible that caregivers take advantage of hospitalization to complete the entire care program for the most fragile or the most isolated patients who would be less able to return for the rest of their care.
These inequities are also observed for access to other therapeutic procedures. Percutaneous cholecystostomy represents an alternative to surgery in clinically frail patients. Its access and use might be impacted by socioeconomic factors. 37 It has been shown that patients from poor social classes are less easily transferred for biliopancreatic diseases (OR=0.73, 95% CI: 0.55–0.96, p=0.024), which would imply inadequate access to specific care techniques or expert centers for these populations. 38
Inequities could also be due to geographic factors. Regarding the management of bile duct stones, Poulose et al 39 demonstrated that patients treated in urban areas benefitted more from ERCP, while patients in rural areas were more easily managed by surgery. The availability of ERCP in urban areas was estimated at 35–44% versus 5–25% in rural areas. 39
Recent data showed that the rate of urgent ERCP performed in the 2000s in patients with acute biliary pancreatitis without associated cholangitis was higher in high-volume hospitals, teaching hospitals, and midwestern and western U.S. states. 40 Even if the indication for this procedure has changed and is currently reserved for pancreatitis associated with cholangitis, this testifies to the unequal access to urgent ERCP according to institutions. Concerning same admission cholecystectomy for mild acute biliary pancreatitis, a previously cited study shows that same admission cholecystectomy was positively associated with urban hospitals (vs. rural; OR=1.5, 95% CI: 1.3–1.7) of the South (vs. Northeast; OR=1.5, 95% CI: 1.3–1.7). 34
Only old data did not seem to show an impact of SES on performing cholecystectomy: there was no increase in the standardized rate of surgery according to the SES estimated by the patient's or spouse's profession. 17 These conclusions were confirmed more recently by the Swedish Palsson. 41 In this investigation, neither marital status, level of education, or level of income showed any impact on the incidence of surgery. However, it should be noted that this study was conducted on a population of cholecystectomized patients. There is no detail in these data to determine the impact of SES on access to surgery.
All these data, even if they remain open to criticism, highlight more complex access to various therapeutic interventions for vulnerable populations to treat gallstone disease without the potential to identify the factors that influence these conclusions: limited access to care for economic reasons, difference in treatment by physicians, patient refusal of proposed care depending on the level of education, and so on.
Do social determinants impact quality of care for gallstone disease?
Socioeconomic determinants could also influence the quality of care. Varela and Nguyen 42 showed that patients with private insurance were more likely to have a laparoscopy than open surgery for cholecystectomy (OR=1.25, 95% CI: 1.21–1.29). These data were confirmed by two American studies. The first shows an increased risk of conversion to open surgery for patients receiving Medicaid (3.9% vs. 3.0%, p=0.001). 27 In the second one, patients with the lowest income level underwent urgent operations more frequently (71.7% vs. 66.9%, p<0.001) by the open approach (14.8% vs. 11.3%, p<0.001). 43
A Swiss study concluded that there was an increased risk of open surgery in patients without private insurance. 44 Similarly, it has been shown that socially frail patients are more likely to undergo cholecystectomy in an emergency setting than electively, regardless of the clinical situation and the cause of the intervention. In two studies, using collective indices of social deprivation, in particular the “Social Vulnerability Index,” Carmichael et al45,46 showed that having a high index of deprivation increases the risk of emergency operation (OR=2.05, p<0.04). The same team showed that this increased risk was present in patients without insurance or with public insurance (OR=2.78, p<0.001). 47
In addition, they found in this study that these patients had more chronic symptoms, which would tend to show that they wait for long periods of time to consult with a physician and ultimately need emergency surgery. 47 Another U.S. study showed that uninsured patients were much more likely to undergo urgent operations (99.3% vs. 47.9%, p<0.001). 48 A recent American study showed that the probability of outpatient surgery was lower in patients with Medicare (OR=0.77, 95% CI: 0.75–0.80, p<0.001) or Medicaid (OR=0.56, 95% CI: 0.54–0.57, p<0.001), or among self-pay patients (OR=0.28, 95% CI: 0.27–0.28, p<0.001), than in patients with private insurance. 49
The type of institution would possibly have little impact on the quality of interventions. According to Ibrahim et al, 50 “Critical Access Hospitals” in the United States, defined as hospitals with fewer than 25 beds and located more than 35 miles from any other hospital, had a lower in-hospital mortality after cholecystectomy (1.3% vs. 2.2%, OR=0.58, 95% CI: 0.47–0.72, p<0.001), lower rates of major complications (5.0% vs. 12.1%, OR=0.32, 95% CI: 0.28–0.36, p<0.001), or overall complications (13.2% vs. 21.7%, OR=0.48, 95% CI: 0.45–0.52, p<0.001). However, these results must be considered with caution because the patients treated in these centers were less severe. 50
Conversely, in biliary pancreatitis, it has been shown that hospital status determines the application of best practice recommendations. Thus, the proportion of cholecystectomized patients during the same period of hospitalization for nonsevere biliary pancreatitis was higher when these patients were treated in hospitals in urban areas (OR=1.5, 95% CI: 1.3–1.7) or in high-volume hospitals (OR=1.3, 95% CI: 1.2–1.4). 34 Finally, the Swiss study, previously cited, demonstrated that patients living in a rural area were more likely to have open surgery for cholecystectomy. 44
Do social determinants impact the prognosis of gallstone disease?
Overall, all available data show a poor prognosis for gallstone disease in severely deprived patients regardless of their clinical status.
Patients with low socioprofessional status have poor prognosis after cholecystectomy. 43 In a large American study of 2,058,611 cholecystectomies, the authors separated patients into 4 categories according to the quartile distribution of household income. The poorest group of patients was younger (50.5 vs. 53.4 years for the richest p<0.001), had fewer comorbidities according to the Charlson comorbidity index (2.08 vs. 2.16, p<0.001), and had more patients without private medical insurance (31.1% vs. 54.8%, p<0.001). 43 High-income patients had lower mortality (OR=0.88, 95% CI: 0.82–0.95, p<0.001), while patients without private insurance had more post-operative complications and poorer survival. 43
An Asian study on 225,558 cholecystectomies confirmed these results. A higher rate of 30-day mortality (4.65% vs. 2.18%, p<0.001), complications (0.62% vs. 4.01%, p=0.008), or readmissions for complications (1.83% vs. 1.09%, p<0.001) was observed in patients with low income than in the general population. 51 In outpatients, the rate of complications or rehospitalization was higher in self-pay patients or patients with Medicaid/Medicare. 49
This poor prognosis is also true in patients treated with percutaneous cholecystostomy, with significantly higher hospital mortality in low-income patients (OR=1.816, 95% CI: 1.079–3.056). 52
In the United States, patients hospitalized for acute cholangitis with Medicare/Medicaid had a poorer prognosis than insured patients: a significant increase in mortality, a longer hospital stay and increased medical costs. 53 More generally, in patients who benefitted from ERCP, the patient's lack of insurance was a risk factor for readmittance following this procedure (OR=1.18, CI: 1.06–1.32). 54
Regarding acute biliary pancreatitis, Roberts et al 55 did not find a significant impact of socioeconomic deprivation on the mortality of pancreatitis, regardless of its etiology. To our knowledge, no data exist on the influence of these parameters on the occurrence of severe or complicated forms of acute biliary pancreatitis.
Data about the impact of geographical factors on prognosis are few. In one study, the rate of complications or rehospitalization in outpatients after cholecystectomy was lower in patients living in metropolitan areas than in rural areas (OR=0.44, 95% CI: 0.31–0.62, p<0.001, and adjusted OR=0.79, 95% CI: 0.65–0.96, p=0.016, respectively). 49
Discussion
Both severe and complicated types of gallstone disease seem more frequent in underprivileged populations.23,25,43 Furthermore, their prognosis seems less favorable regardless of their clinical status.23,43,51,52
If this review seems to show an impact of socioeconomic determinants or geographic factors on access to treatment and the prognosis of biliopancreatic disease, the precise role and the importance of these determinants are very difficult to dissect.
Several risk factors influence the occurrence of gallstone disease (sedentary lifestyle, diabetes, obesity, Non-Alcoholic SteatoHepatitis, diet, hormonal treatments, and history of bariatric surgery). 56 These risk factors are socially stratified and distinguishing the impact of a socioeconomic factor on the disease or its risk factors is not always easy. Likewise, a socially stratified risk factor can influence the development of a severe type of the disease and the type of treatment provided. For example, it is clearly established that the risk of gallbladder stones is higher in patients with obesity, but these patients also have an increased risk of presenting symptomatically or severe type of the disease. 57 Obesity can also affect the type of surgery (open, outpatient surgery, etc.) and the complication rate. 58 Obesity is clearly impacted by socioeconomic determinants.59,60
The reasons for the association between SES or geographic distribution and lithiasis disease or the quality of its management are currently hypothetical. Further analyses would be necessary to determine the relative impact of each of these determinants on the following: disease development, initial diagnosis, attitudes of patients and caregivers toward the disease, quality of patient care offered and provided, monitoring, and prevention. For example, the lesser quality interventions may be due to a less favorable clinical situation for patients who wait longer to seek medical care. 47 In addition, caregiver's might tend to choose treatments that reduce care costs or the length of stay for financially fragile patients. Finally, the level of expertise of caregivers in centers caring for these deprived patients might be lower. 54
The data collected in this systematic review have several limitations. A majority of the studies are conducted in the United States. In this country, where payment for health care costs can depend directly on the patient's insurance status, the level and type of treatment can clearly depend on the patient's SES. This is perfectly illustrated by the changes in cholecystectomy management of U.S. patients before and after the health insurance reform in the United States.29–31,61 In European countries, the health care system generally allows for the equal treatment of patients after the diagnosis. Potential inequality according to social status can result from differences in patient access to diagnosis and to the center of competence. 62 Few data from European countries are currently available to verify the potential transposition and universality of results shown in this review.
On the other hand, the tools used in this review to assess patients' SES are heterogeneous, which can lead to difficult comparisons. The majority of the studies selected in this review uses individual indices such as education level, occupation, income, or insurance status. While these indices are specific to patients, few studies combine a synergistic analysis of several of these indices that could cause interpretation bias. For example, a patient may have low income over a period of time, despite a high level of education. Conversely, other studies use indices of social deprivation, which have the large advantage of providing a measure of people's SES in the absence of individual data by using the patients' address.
However, the place of residence is not necessarily a relevant index to define the patients' economic status. In the future, the use of standardized assessment tools could limit these biases and allow a better comparison of results between studies.63,64
A better knowledge of factors influencing the management of biliary diseases could help to restore health equity in the management of gallstone disease. Since patients' insurance status can impact their access to high-quality care, health insurance policies can be changed first as it was conducted with the reform of health insurance in the United States in 2013. In theory, improving care for populations with low SES should be based on improved access to teaching hospitals and/or high-volume care centers.65–67 Currently, the geographic distribution of the centers is only slightly regulated.
An example of territorial organization of care has been used for several years to manage acute illnesses by creating neurovascular units to manage stroke or to allow for the early treatment of patients with heart attack, with the distribution of coronary angiography centers. We could imagine, using the same example, a regulated distribution of ERCP centers as a result of the impact of ERCP delays on the prognosis of acute cholangitis.68,69 At the patient level, the fight against risk factors (sedentary lifestyle, and obesity), which are themselves socially stratified, can make it possible to reduce the occurrence of gallstones disease, especially in the most fragile patients.
To cite only this example, the creation of walking groups within disadvantaged communities has proven to improve the practice of physical activity. 70 The support of patients by workers dedicated to this task can improve the care and adherence to care of the most fragile patients. Interprofessional teams that include social workers in integrated care settings can improve the coordination of care and behavioral health of patients, compared to the usual primary care model. The addition of social workers to primary care teams reduced Emergency Department Visits 71 or the number of hospitalizations. 72
Following the same logic, patient navigation programs using community-based culturally and linguistically concordant patient navigators, which can serve as a bridge between the patient and the health care system, have been developed for many years to support the most fragile patients and motivate them to follow the best care. Other programs have shown to improve enrollment in cardiac rehabilitation, 73 colorectal cancer screening participation, 74 or early access to supportive care for patients with advanced cancer. 75 Such programs could be developed in gallstone diseases to improve access to care and avoid emergency treatment or complications.
At the level of physicians, interventions aimed at improving adherence to guidelines could be elaborated. 76 Such interventions could make it possible to develop good surgical practices and standardize these practices regardless of geographical areas or local expertise. Financial incentive strategies have also been developed, but with mixed results. 77
Conclusion
Gallstone disease represents a growing public health problem in Western countries. Few data are currently known on the impact of socioeconomic determinants and geographic factors on the occurrence and management of these diseases, but all seem to highlight poor access to optimal treatment for vulnerable populations. A better knowledge of these parameters could possibly improve public health policies for the management of these diseases and the distribution of care.
Footnotes
Authors' Contributions
Guarantor of the article: B.D. Study concept and design: all authors. Literature screening and data acquisition: B.D. and O.D. First draft of article: B.D. Figure design: B.D. Data interpretation, critical revision of the article, and approval of final version: all authors.
Author Disclosure Statement
Authors declare no conflict of interests for this article.
Funding Information
No financial support.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.