
Abstract
Objective:
This systematic review examined and synthesized peer-reviewed research studies that reported the process of integrating social determinants of health (SDOH) or social needs screening into electronic health records (EHRs) and the intervention effects in the United States.
Methods:
Following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines, a systematic search of Scopus, Web of Science Core Collection, MEDLINE, and Cochrane Central Register of Clinical Trials was performed. English language peer-reviewed studies that reported the process of integrating SDOH or social needs screening into EHRs within the U.S. health systems and published between January 2015 and December 2021 were included. The review focused on process measures, social needs changes, health outcomes, and health care cost and utilization.
Results:
In total, 28 studies were included, and half were randomized controlled trials. The majority of the studies targeted multiple SDOH domains. The interventions vary by the levels of intensity of their approaches and heterogeneities in outcome measures. Most studies (82%, n=23) reported the findings related to the process measures, and nearly half (43%, n=12) reported outcomes related to social needs. By contrast, only 39% (n=11) and 32% (n=9) of the studies reported health outcomes and impact on health care cost and utilization, respectively. Findings on patients' social needs change demonstrated improved access to resources. However, findings were mixed on intervention effects on health and health care cost and utilization. We also identified gaps in implementation challenges to be overcome.
Conclusion:
Our review supports the current policy efforts to increase U.S. health systems' investment toward directly addressing SDOH. While effective interventions can be more complex or resource intensive than an online referral, health care organizations hoping to achieve health equity and improve population health must commit the effort and investment required to achieve this goal.
Introduction
In Sir Michael Marmot's landmark Whitehall study (1978), 1 he offered primary evidence of the dose–response association between the health outcomes and socioeconomic status of those in the British Civil Service. As a result of this, our collective understanding of the impact of social, economic, behavioral, and environmental factors on individuals' health has grown. Social determinants of health (SDOH) are defined by The World Health Organization Commission2–4 as the “conditions in which people are born, grow, live, work, and age.” This landmark document outlined three recommendations for improving the conditions experienced by individuals: (1) address unbalanced distributions of power, money, and resources; (2) measure the problem; and (3) evaluate the impact of actions.
United States Health systems' interest in addressing SDOH has increased markedly in recent years, as exemplified by new attention from policymakers and researchers. For example, in the 2010 Patient Protection and Affordable Care Act, a mandate was implemented that requires nonprofit hospitals to participate in community-level planning to improve community health and to conduct Community Health Needs Assessments every 3 years. 5 Mounting evidence shows that SDOH account for substantially more variation in health outcomes than medical care.3,6 A social need is described as the need of an individual as a result of SDOH. 7 Thus, investment in addressing social need(s) through social services (e.g., housing, financial resources, food access), care coordination, and community outreach can positively impact health outcomes and reduce health care spending. 8
As the U.S. health care systems move toward value-based models that incentivize positive results, they have started the momentum to seek out new ways to collect data on SDOHs from patients' electronic health records (EHRs) and incorporate SDOH-related screen and referral, specifically to screen for social needs, and provide a tailored intervention into routine care among patients who are identified to have social needs.9,10
Prior reviews have explored the impact of screening for SDOH in clinical care settings, 11 using SDOH data found in EHR to predict risk, 12 reliability, and validity of screening tools, 13 and effectiveness of intervention in addressing multiple domains of SDOH or a particular social need in the health care setting,14,15 as well as evidence, implementation, challenges, and opportunities. 16 However, at least four questions related to the implementation and effectiveness of interventions to address domains of SDOH remain not fully answered. First, is screening for social needs in clinical settings effective? Few studies provided clear descriptions of the clinical workflow involved in screening for and integrating SDOH in EHRs, and the subsequent interventions either through social prescriptions, such as health professionals working with social workers or community connectors to refer patients who have social needs with community resources or social services. Social prescription can be administered through referrals or direct support within health care settings to address patients' social needs related to SDOH.
Second, are social needs interventions delivered in clinical settings effective at reducing cost/utilization and improving clinical outcomes? To our knowledge, and documented in other reviews,14,16,17 limited studies reported intervention effects on a full range of outcomes, including (1) process measures; (2) short-term outcome directly related to social needs (e.g., level of need and what percentage of these needs were met), (3) intermediate outcome or impact on health outcomes, and (4) long-term outcome or impact on health care cost or utilization. Within these studies, less than half reported impacts of such intervention on SDOH (48%), health impact (30%), and health care cost or utilization impacts (27%), respectively. 14 Third, what are the components of effective social needs interventions in clinical settings? Fourth, what are barriers, facilitators, and resources needed to implement effective social needs interventions in clinical settings?
To address these gaps, this systematic review examined and synthesized peer-reviewed research studies that reported the process of integrating SDOH or social needs screening into EHRs for documenting social needs and the intervention effects on a full range of outcomes, including process measures, impacts on social needs, health outcomes, and health care cost and utilization. In addition, this review discussed current gaps and opportunities to implement effective social needs interventions in future research.
Methods
Data sources and search strategies
Following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) checklist and guidelines, a systematic review was conducted to summarize the existing studies. 18 Four major medical and public health databases were used in this study, including Scopus, Web of Science Core Collection, MEDLINE (Ovid), and Cochrane Central Register of Clinical Trials (Wiley). Limits set included articles in English, conducted in the United States, and published between January 1, 2015 (the year immediately after collecting SDOH in health care systems was recommended by the Institute of Medicine) and December 2021.
The strategy deployed for this search used keywords and medical subject headings (MeSH) combined with database-specific techniques for advanced search. A number of keywords and MeSH terms were identified to represent the topics of SDOH, social needs, screening, and EHRs in health care setting. According to Healthy People 203019 framework, SDOH are categorized into five different domains: “economic stability, education access and quality, health care access and quality, neighborhood and built environment, and social and community context.” Given the current literature and the diverse topics of addressing social needs or SDOH, the Healthy People 203019 framework was used to select articles for inclusion and synthesizing (Fig. 1).

Healthy People 2030 social determinants of health framework. SDOH, social determinants of health. Citation of the SDOH graphic: Healthy People 2030, U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Retrieved December 12, 2021, from https://health.gov/healthypeople/objectives-and-data/social-determinants-health
Following the guidelines established above, the keywords and MeSH terms were established for each of the four databases. The strategy for this search is fully detailed in Supplementary Data S1. In sum, 2241 results generated from the literature searches were downloaded into the reference management software Endnote. After removing duplicate articles, 1325 unique publications were uploaded into Rayyan online review software 20 (https://rayyan.qcri.org/) for subsequent screening. For comprehensiveness, we included additional eight journal articles identified from other sources, such as Google Scholar, and further from a citation search by scanning the references of these articles.
Study selection: inclusion and exclusion criteria
Two independent reviewers (A.Y. and Y.W.) screened all the results to determine eligibility for this review. Selection was based on whether the study met all six inclusion criteria detailed below. The rationale for inclusion and exclusion criteria aligned with the study objectives.
Published in peer-reviewed academic journals, between January 1, 2015, and December 2021, and in English;
Studies that involved interventions/quality improvement initiatives targeting social risks or domains of SDOH;
Conducted in a U.S. health care setting;
Studies that explicitly mentioned or implied modules/tools embedded into EHR system and described the clinical SDOH-EHR integration as part of the clinical workflow, which also reported some or all of the components of the workflow (i.e., time frame and care team member[s] for administering an assessment/screening, and data entry; identify EHR-documented SDH needs and SDOH referral or intervention; tracking referrals and follow-up);
Studies that examined the impact of such interventions/quality improvement initiatives on a host of outcomes, including process and outcome changes on social needs, health impact, and health care cost or utilization.
Studies were excluded if they were (1) systematic reviews/meta-analyses; (2) opinions, commentaries, or perspectives; (3) qualitative studies; (4) cross-sectional or observational studies that simply used the hospital/clinic EHR system as a tool for extracting data records to investigate the associations between SDOH and health outcomes/health care utilization; or (5) study protocol. Lastly, we excluded studies primarily focused on health care access or outreach programs. Although health care access contributes to health disparities, the focus of this review was health system/clinical programs that integrate SDOH screening (to identify social and economic needs) into an EHR system to address patients' unmet social or financial needs.
Data extraction and assessment of bias
The data screening and extraction involved a two-phase procedure. The first screening phase was a title/abstract review, and the second phase was a full-text review. Both phases were blinded (one reviewer cannot see the decision of the other) to avoid reviewer bias and conducted in Rayyan. Conflicts on review results were resolved through group consensus. The first phase of screening identified 145 articles for the full-text screening. Following the inclusion and exclusion criteria being applied to the second phase screening, 28 articles were left for synthesis.
Two independent reviewers (A.Y. and Y.W.) extracted the data listed below from each article by following a uniform format: (1) study design, sample characteristics and sample size, study quality; (2) clinical setting; (3) target SDOH (what SDOH were screened and the screening tool[s]); (4) integration into clinical workflow (i.e., screening and data collection); (5) intervention; and (6) outcome measures. The quality of these studies was then graded based on the quality rating of the Grading Recommendations Assessment Development and Evaluation (GRADE). 21 Then the article results selection in each phase of search and screening processes are provided in Figure 2. PRISMA checklist was presented in Table 1.
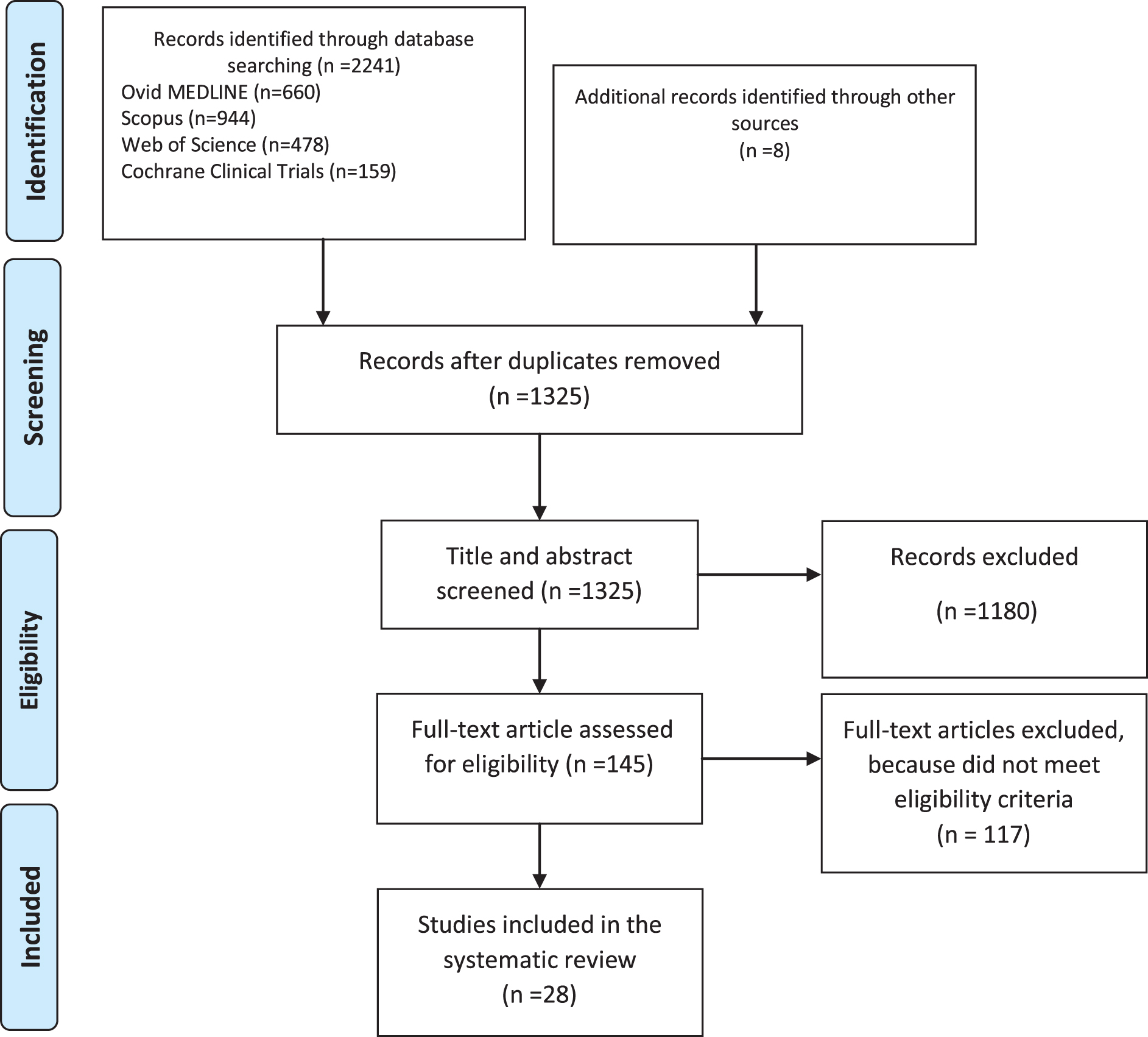
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Preferred Reporting Items for Systematic Reviews and Meta-Analysis Checklist
PICOS, participants, interventions, comparisons, outcomes, and study design.
Results
Twenty-eight studies22–49 were included in this systematic review. Their characteristics are summarized in Table 2.
Key Characteristics and Results of Twenty-Eight Studies Included in the Systematic Review
BMI, body mass index; BP, blood pressure; CC/SC, collaborative care/stepped care; CDC, Centers for Disease Control and Prevention; CDE, Certified Diabetes Educator; CHAMP, Complex High Admission Management Program; CHCs, community health centers; CHWs, community health workers; CPD, cigarettes per day; CRS, community resource specialist; CTI, critical time intervention; DBP, diastolic blood pressure; DUFB, Double Up Food Bucks; DULCE, Developmental Understanding and Legal Collaboration for Everyone; EHR, electronic health record; ER, Emergency Room; FQHCs, Federally Qualified Health Centers; FS, family specialist; ICD-10, International Classification of Diseases, 10th Revision; IMPaCT, Individualized Management for Patient-Centered Targets; KPSC, Kaiser Permanente Southern California; LDL-C, low-density lipoprotein cholesterol; MSW, Master of Social Work; NCM, Nurse Care Managers; PCP, Primary Care Provider; RCT, randomized controlled trials; SBDOHs, social and behavioral determinants of health; SBP, systolic blood pressure; SCP, standard of care plus; SDOH, social determinants of health; SNAP, Supplemental Nutrition Assistance Program; T2DM, type 2 diabetes mellitus; VIP, violence intervention program; WIC, women, infants, and children.
Study design, sample characteristics, quality of studies, and clinical settings
Out of 28 studies reviewed, 14 were randomized controlled trials (RCT)22,24–27,29,35,38,39,43–45,47–49 and the other study designs included quasi-experimental design or pre/post designs. Samples included adults and parents/caregivers of pediatric patients. In terms of clinical settings, the majority of the studies were conducted at health care organizations servicing low-income individuals and families, such as Federally Qualified Health Centers (FQHCs), safety-net hospitals, community health centers, and primary care practices where the prevalence of social and economic barriers to health is high among the patient population. The quality ratings of studies varied from very low to high based on the GRADE approach. 21
SDOH-EHR integration (i.e., screening, data collection, integration into EHR) into the clinical workflow
All studies provided some basic information regarding the screening for SDOH and integration of such screening into the workflow. The integration process was performed using any secure electronic device (e.g., tablets, computers) and software (e.g., electronic data capture systems/tools such as REDCap). The collected data were further integrated into EHR systems (i.e., Epic) of clinical institutions to identify at-risk individuals and to guide targeted intervention strategies or referral services to address corresponding unmet social needs in follow-up appointments. Studies reported either using EHR to identify at-risk patients who may need social and economic assistance,24,31,43 or in-person screening—usually including descriptions about responsible care team members and the time frame for SDOH screening.22,25,26,29–34,36,38–40,44,48,49 However, the time frame for data entry into the EHR was not discussed in studies. Of all the studies reviewed, only one 41 reported the process of SDOH screening and capturing responses as standard International Classification of Diseases, 10th Revision (ICD-10) codes in the EHR.
Target SDOH and interventions
The majority of the studies targeted and addressed multiple SDOH domains, including housing instability and inhabitability (i.e., supportive housing, rent subsidies, assist in household heat, or paying utility bills), basic needs (i.e., provide shoes, clothing), food insecurity, transportation, low income/financial constraints, unemployment/loss of job or underemployment, childcare, medical/legal assistance, lack of medical insurance and other public benefits enrollment, and concerns about adult household member's mental health, drug and alcohol use, neighborhood safety, trauma, exposure to violence (including domestic violence), and discrimination. Frequently, studies described participants having two or more social needs. The most often reported social needs were related to housing, food, childcare, and finances.
Interventions all targeted individual-level SDOH, including social and economic needs. These interventions vary by the level of intensity of their approaches. The simplest approach involved health system staff identifying social risks and needs among patients and following up either by distributing a booklet of community resources or referring patients to community resources or social services. This practice usually had little follow-up or process evaluation to determine whether patients received the resources they needed. The second and more advanced approach involved a patient navigation process (usually administered by patient navigators, social workers, or case managers) that helped navigate patients to external human or social services based on EHR-embedded SDOH information. The third approach involved a transition care coordination model that helped patients move through different levels and types of care at different facilities. Referrals, developing an individual plan for coordination of care, and managing information exchange between providers and other social service organizations is the responsibility of the care coordinator. This approach usually targets patients at higher risk for hospital readmission.26,27,43,49
Outcome measures
Based on the Centers for Disease Control and Prevention program evaluation framework,50,51 we organized the outcome measures into four categories, including (1) process measures, (2) short-term outcome directly related to social needs, (3) intermediate outcome or impact on health outcomes, and (4) long-term outcome or impact on health care cost or utilization. Process measures established whether program activities were being implemented as proposed. Meanwhile, outcome measures evaluated effectiveness of the program on the short-term outcomes on the targeted population, for example, changes on the SDOH, intermediate outcomes such as the health outcome, and the long-term outcome, such as the impact on the health care cost and utilization. Most studies (n=23, 82%) reported the findings related to the process measures, and nearly half (n=12, 43%) reported outcomes related to SDOH. By contrast, 39% (n=11) of the studies reported health outcomes, and only 32% of the studies (n=9) presented findings related to the impact on health care cost and utilization.
The process measures and impacts on patients' social needs
The process measures include number of social referrals; number of people able to identify their social needs; rate of patients who agreed to receive help (referral uptake); percentage of patients who contacted a referral agency, enrolled in new community resources, reported using community resources or social services; and patients' overall satisfaction with the referral/patient navigation services or satisfaction with care.22–25,28,30–41,43,45,46 Findings were largely positive for process measures. Similarly, although fewer studies reported findings related to a program's impact on patients' social needs change, those studies led to improved access to resources, resolutions of identified problems, or decreased self-reported social distress score.22,23,25,29,31,34,35,40,42,44
The health outcomes
Overall, few studies included the health measures. The health outcomes measures had little consistency across studies and varied by population age (adults vs. the pediatric population). Health outcome measures included health-related behaviors24,34,37 (e.g., quit cigarette smoking, fruit and vegetable consumption, etc.), physical health,28,30,32,33,38,39,44 quality of life and depression, 45 and injury. 31 The evidence of program impacts on health is mixed. Some studies reported improved health, including increased likelihood of quitting smoking, 24 improvements in child health (caregiver self-report),29,44 better blood pressure during pregnancy, 30 decreased violent reinjury rate, 31 improvements in systolic blood pressure (SBP) and diastolic blood pressure, lowered low-density lipoprotein cholesterol level, 33 increased fruit and vegetable consumption, 34 self-rated physical health and disease self-management, 38 improvements in quality of life, and reduction of reported depression. 45 In contrast, others reported no changes in behavioral health, 37 in patient-selected chronic disease (HbA1c, body mass index, SBP, or cigarettes per day),38,39 or hemoglobin A1c. 33
Health care cost and utilization
Across studies, health care cost and utilization measures varied widely while findings were mixed but trending positive. Several studies reported positive impacts on health care cost and utilization measures, such as improved immunization completion rates, routine visits for preventative care, lowered ED visits/hospitalizations among children25,47; decreased 30-day hospital readmission rates, repeat hospitalization, or total utilization in adults,26,38,39,42 while others reported null findings in adults.37,43,46 Only one study reported the cost-effective findings regarding return in investment in an average Medicaid payer within the fiscal year.42,43
Discussion
This systematic review of 28 studies conducted within the U.S. health system examined and synthesized the process of integrating SDOH screening into EHRs and the impact of social needs intervention on a full range of outcomes. In studies that reported the process measures, findings were generally positive. Similarly, findings related to programs' effects on patients' SDOH-related social needs change demonstrated improved access to resources. However, these interventions impact on health outcomes and health care cost and utilization were mixed. As a whole, this study contributed to the literature by shedding light on several clinical and population health-related research questions regarding the implementation and effectiveness of social needs screening and interventions.
First, our study expands the literature on the current clinical workflow for SDOH screening and integration in EHRs. To our knowledge, few review articles provided clear descriptions of the clinical workflow involved in screening for and integrating SDOH in EHRs, and the subsequent interventions through social prescriptions, such as health professionals working with social workers or community connectors to connect patients who have social needs with community resources or social services. Our findings indicate that research is needed to explore more efficient means of SDOH screening/EHR integration (i.e., screening, data collection, and integration into EHR) into the clinical workflow. Studies reviewed in this article reported various methods for screening and coding, and only one study explicitly described using codes from International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) to document patients' SDOH. To facilitate the integration into the clinical workflow, the essential first step is data standardization.
It is critical to implement data standardization in clinical decisions to ensure suitable interventions and referral practices are deployed by nurses, physicians, and health staff to address SDOH and the sharing of social needs data across health care facilities.52,53 In addition, data standardization is important for valid data aggregation across EHR system of various practices and communities. However, no uniform, accepted data model or established criteria represent these determinants in EHR systems.53,54 Similar to utilizing ICD-10-CM codes and Current Procedural Terminology in diagnosis and procedures/billing, respectively, the American Hospital Association has suggested documenting and coding SDOH using the many available ICD-10-CM codes. 55 For example, categories Z55–Z65 (“Z codes”) of the ICD-10-CM codes are available for hospitals to capture patient's social needs. Current Z codes include data on patient's socioeconomic status such as access to employment, education and literacy, housing, or adequate food and/or water.
Although the American Hospital Association wants to promote the usage of Z codes, health systems' adoption of SDOH Z codes remain slow. Based on a retrospective cohort study using the 2016 and 2017 National Inpatient Sample from the Healthcare Cost and Utilization Project database—the largest publicly available all-payer inpatient care database in the United States, of 14,289,644 admissions, 269,929 (1.9%) had an associated SDOH Z-score content. 56 This number indicates SDOH Z-scores are not being utilized to an appropriate degree within the health system. Thus, the coding being used at this time is probably reflecting the true burden of social needs poorly for hospitalized patients as unstable housing was reported in 37% of patients with diabetes in a national survey of safety net patients, 57 which is much higher than 1.9%.
In addition, particularly in light of the COVID-19 pandemic, we have observed how SDOH pathways, when linked with pre-existing comorbidities, apply a burden of morbidity and mortality that is much higher than expected upon minority communities.58–60 Without accurately and timely collecting, documenting, identifying, and addressing SDOH, we cannot effectively improve health outcomes and reduce the health disparities that have long existed to realize equity in health care.
Second, consistent with previous review articles, our review showed that current studies that included both health and health care cost and utilization measures were limited in number and mixed in their results to provide conclusive evidence for the effectiveness of reducing cost/utilization and improving clinical outcomes.14,17,61 In the current review, about half of all studies used RCT design, and only one study reported cost-effectiveness.42,43 More rigorously designed studies are needed as the field moves forward to clarify cost-effective intervention approaches. The sample sizes of studies vary from 18 to 34,225 in nonexperimental design studies and from 89 to 1300 in experimental design studies.
The measurements vary widely even within the same outcome domains and thus make it difficult to compare and synthesize. For example, a study reported the total health care utilization (a count of all visits to the emergency department, outpatient, and/or inpatient) would limit our ability to compare the results in each usage. Null findings from studies that focused on participants with a high-risk or high-utilization rate may experience a widespread statistical phenomenon–regression to the mean, 62 as seen in a recent RCT study—Camden Coalition of Healthcare “Hotspotting” intervention. 43
Third, although interventions vary by the level of intensity, there was insufficient evidence that the intervention intensity and the health or cost and utilization outcomes were dose–response correlated. More contacts or heavy intensities in social needs interventions did not necessarily lead to better health outcomes. A recent randomized control trial compared two interventions in pediatric urgent care settings and suggested no statistically significant differences in the delivery of personalized printed resources about social services with or without longitudinal, in-person navigation services. 44
Fourth, when examining the barriers to/facilitators of, and resources needed to implement effective social needs interventions in clinical settings, we must consider not only patients' uptake but also social service agencies' capacity. Research may assume that current social service agencies have the ability to address the social needs of all community members. 63 But in reality, social service agencies have capacities that vary broadly by the type of social need (easier to manage food-related needs than housing needs or public transportation) and location of the community. 63 This was documented in a recent study, which found that 2-1-1 referrals for food-related needs were the most likely to be met, while referrals for housing-related needs were the least likely. 64 It is not surprising that studies found that only a small portion (10%) of those with social needs could connect with resources to address these needs 42 or low participation rates in government benefits or assistance. 43
A recent review 16 suggested a deeper understanding of an individual's social needs patterns, timing, and sequences. Our findings suggest that for social needs to be met there must be a shift from reactive damage control to proactivity that seeks to address many upstream determinants (such as racism) at the population level.
Fifth, we call for future studies to report the capacity for innovation and the implementation of value-based payment models. The value-based payment has the potential to spur innovation in upstream prevention, such as screening patients for social risks. By doing so, the health system (i.e., physician practices) can take the early step of addressing social needs that lead to poor health. None of the social screening and EHR integration studies reviewed in this study reported the implementation of a value-based payment model.
This finding was not surprising, although, as a recent cross-sectional study of social risk screening by U.S. physicians indicated that implementing social risk screening in the U.S. health care setting was not associated with the practices' overall exposure to value-based payment. 65 Instead, Brewster et al. found that adopting social risk screening in the U.S. health care setting was associated with high innovation capacity and focusing on low-income populations, regardless of payment incentives. 65 Most of the study settings reviewed in our study were at health care organizations servicing low-income individuals and families with limited innovative capacities, such as FQHCs, safety-net hospitals, and community health centers.
The recent finding by Brewster et al. and our observations have important implications. First, the current practice capacity for innovation, rather than payment incentives, is the primary driver of social risk screening. Second, there is an urgent need to standardize approaches and implementation assistance to reduce the level of innovative capacity required to introduce social risk screening at the practice level.
Lastly, one solution U.S. health systems can provide to improve community capacity is to make more direct investments instead of just screening and making referrals. For example, a recent study 66 identified that 78 new programs (involving 57 health systems, including 917 hospitals) made direct financial investments (at least $2.5 billion) in SDOH from 2017 to 2019. Those investments were committed to direct SDOH, including housing, employment, education, food security, social community context, and transportation. We applaud the efforts of these health systems and encourage them to continue direct and large investments in SDOH.
Limitations
This systematic review has at least two limitations. First, this review has strict inclusion and exclusion criteria, and all studies reviewed were limited to those in the U.S. health system. In addition, the majority of the studies were performed in community health centers. Therefore, we caution against generalizing our findings to other settings. Second, there may be review-level limitations such as incomplete retrieval of identified research and the study/outcome-level limitations, including heterogeneous nature of the studies (variety of outcome measures, different study designs) and the small number of published studies with rigorous design. These limitations make it difficult to quantify the intervention's effects by systematically conducting a meta-analysis. We recommend carefully designed meta-analyses on outcomes related to effectiveness and health care cost and utilization in future studies with rigorous study designs.
Conclusion
In conclusion, this systematic review found positive findings on the effects of interventions on process measures and patients' change on SDOH-related social needs. However, the findings were mixed about the impacts of these interventions on health and health care cost and utilization. Our review supports the current policy efforts to increase U.S. health systems' investment toward directly addressing SDOH, such as housing, food security, and job training. To effectively screen and respond to SDOH in health care settings, a number of changes must occur: federal standards must be established for reflecting SDOH data in EHR, data collection of SDOH, or social needs must be incentivized through financial or quality measures, and rigorous research that examines the impact of these actions must be expanded. While effective interventions can be more complex or resource intensive than an online referral, health care organizations hoping to achieve health equity and improve population health must commit the effort and investment required to achieve this goal.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors would like to acknowledge efforts for this study were partially supported by: National Institute of Diabetes and Digestive Kidney Disease (Egede PI: K24DK093699, R01DK118038, R01DK120861) (Campbell PI: K01DK131319-01); and National Institute for Minority Health and Health Disparities (Egede/Walker PI: R01MD013826). Funding organizations had no role in the analysis, interpretation of data, or writing of the manuscript.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.