
Abstract
Purpose:
This study investigated the magnitude and consequences of educational debt for women physicians.
Methods:
Participants in a women's leadership course were surveyed.
Results:
Of the 185 U.S. physician respondents, 152 (82%) and 85 (46%) reported past debt and current debt, respectively. A total of 164 (89%) perceived a relationship between financial stress and burnout, although burnout scores did not vary by debt magnitude. One-fifth or more reported a negative past influence of debt on each of nine aspects of professional development or well-being.
Conclusion:
Educational debt has negative effects on the careers and well-being of women physicians.
Introduction
High levels of medical student debt are known to be negatively associated with mental well-being and academic performance and tend to drive physicians toward high-paying specialties. 1 The effects of debt on academic performance and choice of practice setting (academic vs. private practice) extend to residency and fellowship years.2,3 Medical students with greater debt are more likely to report financial stress. 1 The impact of debt may be particularly challenging for women, given gender pay gaps demonstrated in numerous studies spanning decades and adjusting for potentially confounding factors.4–6 High educational debt may disproportionately affect individuals who identify as underrepresented minorities or have disadvantaged backgrounds.1,7–9 A study of internal medicine residents showed that higher levels of debt were associated with greater symptoms of burnout. 10 Burnout can lead to attrition that further contributes to physician shortages. In the United States women now outnumber men among medical students, 11 and it is critical to explore educational debt and its impact on burnout and well-being in this population in greater depth. Therefore, we surveyed women physicians about educational debt and its potential consequences.
Methods
Participants in a women's leadership continuing medical education course were electronically surveyed in November 2019. Of the 608 registered participants (all women), 486 were attending physicians, including 422 from the U.S. The survey comprised 39 questions including demographics, questions about debt (defined as educational debt in the questionnaire) and compensation, a battery on perceived impact of debt on select work and lifestyle choices, and Copenhagen Burnout Inventory work-related burnout questions. For questions about the impact of debt on lifestyle or career choices, a 7-point Likert scale (ranging from strongly disagree to strongly agree) was used. To evaluate the associations of current debt with demographic factors (age, race, specialty, years out of training, number of children, practice setting, hours worked, relationship status, spouse/partner gender, spouse/partner full- vs. part-time work status, and time spent on parenting and domestic tasks), Kruskal–Wallis tests were performed. Analysis of variance was conducted to assess the relationship between average burnout score and factors including compensation, debt, and demographics followed by multivariable ordered logistic regression including two-way interactions on individually significant factors. Boston University institutional review board classified this study as exempt.
Results
Of the 185 (44% response rate) U.S.-based attending women physicians who responded to the survey, 152 (82%) reported ever having debt (median $101,000–150,000) and 85 (46%) reported current debt (median ≤$50,000; Fig. 1). A total of 134 (72%) perceived that women do more work-related citizenship/volunteer tasks than men. A total of 164 (89%) agreed or strongly agreed that financial stress is related to burnout. A significantly higher proportion (93%, chi square test, p=0.025) of those in the uppermost quartile of current debt were in agreement. Higher current debt was associated with lower age, lower number of years out of training, and having children 0–7 years old. Lower current debt was associated with having children over 18 years old (Table 1). Current debt escalated in association with increasing hours spent in parenting and domestic tasks by respondents. Higher maximum debt was associated with having children 0–3 years old. Lower maximum debt was associated with a career in academia and having children over 18 years old (Table 1). The racial/ethnic group with the greatest maximum debt was non-Hispanic White/Euro-Americans with a median maximum debt of $201,000–$250,000. This was followed by Latinx/Hispanic Americans and Black/African American/African/Afro-Caribbeans, and Middle Eastern/Arab Americans with a median maximum debt of $151,000–$200,000 each (Fig. 2). There was no significant difference in the amount of debt among women of various ethnic/racial identities; however, the sample size in numerous categories was small.
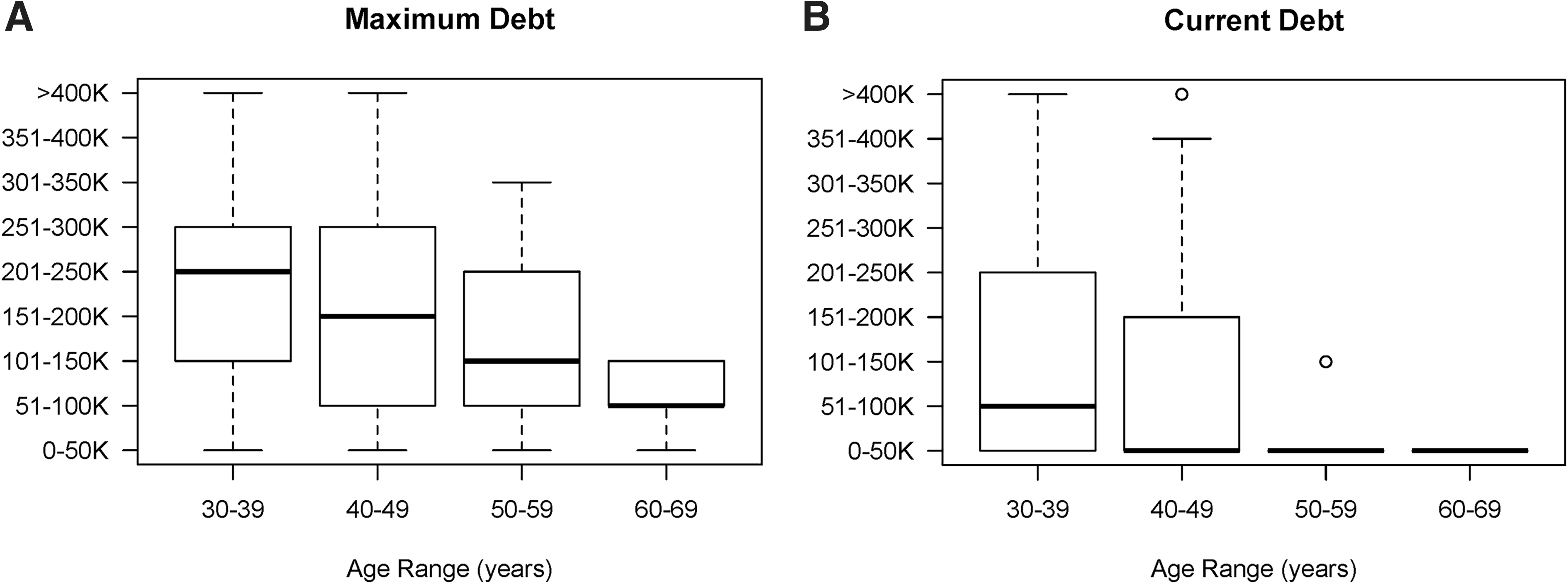
Educational debt stratified by age.

Maximum debt stratified by race/ethnicity. Maximum debt varied, although not statistically significantly, by race/ethnicity. The box spans the second through third quartiles; dark lines indicate the median, and whiskers extend across the first and fourth quartiles. Outliers are represented by circles.
Association of Educational Debt with Demographic Factors
Bold text indicates p-values less than 0.05.
VA, Veteran's Affairs.
One-fifth or more of respondents reported a negative past influence of debt on each work and lifestyle factor queried (Table 2). Debt was not significantly associated with burnout scores. One-way analysis of variance to assess the relationship between average Copenhagen Burnout Inventory work-related burnout score and demographic or compensation and debt-related factors revealed that a lower number of children, greater number of hours worked, and lower maximum and current personal compensation were individually associated with greater degrees of burnout. In a multivariable model including these factors, greater hours worked was significantly associated with burnout (odds ratio 5.1, 95% confidence interval 2.1–12.4). Two-way interactions revealed that working more hours while receiving relatively low compensation resulted in significantly greater burnout. Significant two-way interactions were also seen between numbers of children and greater current and maximum compensation. Greater compensation reduced burnout especially for those with larger numbers of children (Table 3).
Impact of Debt on Work and Lifestyle Choices
Percentage of agreeing includes those who strongly agree, agree, and somewhat agree, and excludes those who neither agree nor disagree, somewhat disagree, disagree, or strongly disagree.
CME, continuing medical education.
Factors Associated with Burnout in a Multivariable Model
Bold text indicates p-values less than 0.05.
ANOVA, analysis of variance; CI, confidence interval; OR, odds ratio.
Discussion
The majority of women physicians surveyed continued to report educational debt, and substantial percentages perceived negative effects of debt on their work and lifestyle choices. Prior studies on medical school debt reveal that high levels may impact specialty selection, academic performance, and mental health. 1 A past study of junior anesthesiology physicians found that educational debt was not associated with burnout but was associated with higher rates of distress and depression. 12 In our study, 93% of those in the highest quartile of educational debt agreed that financial stress was related to burnout. Debt has been found to lead to financial stress among medical students and delays in marriage, having children, and buying a home. 13 A 2020 Medscape survey found that more women than men physicians experience debt owing to childcare (20% vs. 13%) and college and/or medical student loans (33% vs. 23%). 14 Our study adds to this evidence by suggesting that educational debt may specifically constrain women physicians from investing in their health and well-being. In addition, higher educational debt may deter women from investing in career-related opportunities or working in roles that offer lower compensation (academia, administration).
Both educational debt and compensation contribute to financial stress. A 2020 Medscape survey of >3000 women physicians revealed compensation as the number two workplace concern behind work-life balance. 15 More than one-third of these women reported negative effects of their gender on compensation. 15 Compensation disparities are well-documented for women in medicine, and they begin early with their first position after training, 16 continue throughout their careers, 17 and may have a greater impact on those from other underrepresented groups. In some specialties, compensation differences can be attributed reduced clinic volumes as a result of greater time spent with patients. 18 For an individual woman physician, pay disparities may result in hundreds of thousands or millions of dollars of lost income, retirement benefits, and savings over the course of her career. 19 Organizational and legal programs exist to combat pay disparities.20,21 Our study supports the relationship between lower compensation and greater degrees of burnout. The combination of lower compensation with greater work hours or larger numbers of children was particularly impactful, possibly owing to an inability to finance help with domestic or childcare responsibilities.
The impact of debt and compensation on women physicians may be even greater since the onset of the coronavirus disease 2019 pandemic, particularly in areas where women earn less than men. Because of the pandemic, many healthcare institutions are experiencing financial hardship, 22 which has resulted in furloughs, wage reductions, reduced retirement contributions, and elimination of reimbursement for professional expenses.
Recent reports have suggested solutions to educational debt. For example, an accelerated BA/MD combined program, currently 6 years in length, resulted in significantly lower educational debt compared with a matched cohort in a traditional MD program. 23 Another proposed solution is that the public, who benefit from a strong and diverse medical workforce, help to subsidize loan repayment. 24 Anecdotally, some medical schools now offer free or markedly reduced tuition to all students, supported by philanthropy. Loan repayment programs to support careers in government health centers or primary care have been longstanding options. 25
Our study is limited by the population of physicians sampled (participants in a women's leadership course, who may not be typical of other women physicians) and response rate. Gender is a nonbinary construct and all participants in this study self-identified as cis gender women, which limits generalization of the results to other groups. The low response rate and/or makeup of the original sample population may explain the lack of intersectionality in this study. Intersectional identities are critical to consider when evaluating educational debt and compensation, including but not limited to race. Although this study did not find significant differences in debt by race or ethnicity, only 8.6% of respondents identified as underrepresented minorities in medicine. Other important intersectional factors not assessed in this study are the impacts of disability, sexual orientation, and childhood socioeconomic status on the consequence of and willingness to take on educational debt.
Conclusion
In an era where women comprise the majority of U.S. medical students, these findings heighten the urgency to address educational debt and compensation equity on the physician workforce. The literature to date has not definitively demonstrated causal relationships between educational debt, financial stress, and burnout. However, this study demonstrates that many women physicians believe they are linked. Future research should focus on how gender-related compensation disparities and high levels of educational debt affect specialty selection, practice setting, and the well-being and professional development of women physicians.
Footnotes
Author Disclosure Statement
A.R.L. reports no disclosures related to this work. Unrelated to this work, A.R.L. has served on a one-time advisory board for Sanofi Genzyme on resident education in 2019 and has received honoraria for invited lectures such as medical conference and Grand Rounds lectures. R.J. has stock options as compensation for her advisory board role in Equity Quotient, a company that evaluates culture in health care companies; she has received personal fees from Amgen and Vizient and grants for unrelated work from the National Institutes of Health, the Doris Duke Foundation, the Greenwall Foundation, the Komen Foundation, and Blue Cross Blue Shield of Michigan for the Michigan Radiation Oncology Quality Consortium. She is an uncompensated founding member of TIME'S UP Healthcare. S.M.M. has no disclosures related to this work. S.M.M. is the cofounder of the CME leadership course GRIT: Women in medicine and receives no financial remuneration for this effort. Dr. Silver has no disclosures related to this work. As an academic physician, J.K.S. has published books and receives royalties from book publishers, and she gives professional talks such as grand rounds and medical conference plenary lectures and receives honoraria from conference organizers. She has participated in research funded by The Arnold P. Gold Foundation (physician and patient care disparities), Binational Scientific Foundation (culinary telemedicine research), and the Warshaw Institute and Massachusetts General Hospital Department of Medical Oncology (pancreatic cancer). J.K.S. is an uncompensated founding member of TIMES UP Healthcare.
Funding Information
No funding was received for this study.