
Abstract
Purpose:
Lack of appreciation of cultural differences may compromise care for seriously ill minority patients, yet culturally appropriate models of palliative care (PC) are not currently available in the United States. Rural patients with life-limiting illness are at high risk of not receiving PC. Developing a PC model that considers the cultural preferences of rural African Americans (AAs) and White (W) citizens is crucial. The goal of this study was to develop and determine the feasibility of implementing a culturally based PC tele-consult program for rural Southern AA and W elders with serious illness and their families, and assess its acceptability to patients, their family members, and clinicians.
Methods:
This was a three-phase study conducted in rural Beaufort, South Carolina, from January 2013 to February 2016. We used Community-Based Participatory Research methods, including a Community Advisory Group (CAG) with equal numbers of AA and W members, to guide the study. Phase 1: Cultural values and preferences were determined through ethnic-based focus groups comprising family members (15 W and 16 AA) who had cared for a loved one who died within the past year. We conducted a thematic analysis of focus group transcripts, focused on cultural values and preferences, which was used as the basis for the study protocol. Phase 2: Protocol Development: We created a protocol team of eight CAG members, two researchers, two hospital staff members, and a PC physician. The PC physician explained the standard clinical guidelines for conducting PC consults, and CAG members proposed culturally appropriate programmatic recommendations for their ethnic group for each theme. All recommendations were incorporated into an ethnic-group specific protocol. Phase 3: The culturally based PC protocol was implemented by the PC physician via telehealth in the local hospital. We enrolled patients age ≥65 with a life-limiting illness who had a family caregiver referred by a hospitalist to receive the PC consult. To assess feasibility of program delivery, including its acceptability to patients, caregivers, and hospital staff, using Donebedian's Structure-Process-Outcome model, we measured patient/caregiver satisfaction with the culturally based consult by using an adaptation of FAMCARE-2.
Results:
Phase 1: Themes between W and AA were (1) equivalent: for example, disrespectful treatment of patients and family by hospital physicians; (2) similar but with variation: for example, although religion and church were important to both groups, and pastors in both ethnic groups helped family face the reality of end of life, AA considered the church unreservedly central to every aspect of life; (3) divergent, for example, AAs strongly believed that hope and miracles were always a possibility and that God was the decider, a theme not present in the W group. Phase 2: We incorporated ethnic group-specific recommendations for the culturally based PC consult into the standard PC consult. Phase 3: We tested feasibility and acceptability of the ethnically specific PC consult on 18 of 32 eligible patients. The telehealth system worked well. PC MD implementation fidelity was 98%. Most patients were non-verbal and could not rate satisfaction with consult; however, caregivers were satisfied or very satisfied. Hospital leadership supported program implementation, but hospitalists only referred 18 out of 28 eligible patients.
Conclusions:
The first culturally based PC consult program in the United States was developed in partnership with AA and W Southern rural community members. This program was feasible to implement in a small rural hospital but low referral by hospitalists was the major obstacle. Program effectiveness is currently being tested in a randomized clinical trial in three southern, rural states in partnership with hospitalists. This method can serve as a model that can be replicated and adapted to other settings and with other ethnic groups.
Introduction
Culture fundamentally shapes how individuals make meaning out of illness, suffering, and dying, 1 and it strongly influences people's responses to diagnosis, illness, and treatment preferences.1–3 Considering patients' and families' culture is essential in all aspects of palliative care (PC). A lack of sensitivity to cultural differences may compromise end-of-life care for minority patients. 4 However, culturally appropriate models of care that consider the diverse cultural preferences of seriously ill rural patients and their family caregivers are not currently available in the United States. There is an urgent need for research that emphasizes varying end-of-life care cultural preferences.4–10
The triple threat of rural geography, racial inequities, and older age hinders access to high-quality PC for rural Americans. In a state-by-state report card,11,12 the Southeastern United States, where a there is a significant proportion of rural dwellers and African Americans (AAs), PC access was ranked the lowest in the nation. Rural patients with life-limiting illness are at high risk of not receiving appropriate care due to a lack of health professionals (nearly two-thirds of rural U. S. counties are designated health professional shortage areas), 13 long distances to treatment centers, 14 and limited PC clinical expertise. 15 Seventy-five percent of South Carolina (SC) is rural, and 34% of its residents reside in rural areas, 16 where poverty and unemployment rates are high and per capita income is low. 17 AAs comprise 36% of those who live in rural SC. 18
The lack of PC services in rural settings is evident in the lack of guidance by national organizations to address the unique challenges and barriers faced by rural patients. 19 The clinical guidelines on quality PC from the National Consensus Project 20 did not contain the term “rural” through the first three editions, nor did they address how these standards should be applied in rural settings. 21 Geographic inequities in access to PC are expected to rise as the rural population ages and the demand for PC increases. 22 Rural patients with life-limiting illness remain vulnerable and at high risk of not receiving appropriate care. During the past few months of life, rural patients may experience significant and unnecessary suffering that an accessible PC consult could have alleviated; this is a major disparity for seriously ill rural patients. 7 The need for research to guide best practices in providing PC to rural patients is pressing. 21
Even when palliative and hospice services are available, AAs, when compared with Whites, are more likely to receive medically ineffective, poor quality, and high-cost care, due to general mistrust of health care providers and a fragmented health care system that is generally insensitive to cultural differences that can guide treatment choices.23–28 Despite proven effectiveness, numerous studies have shown that AAs underutilize palliative and hospice care.29–34 Suggested reasons for this include both a lack of exposure to hospice or PC information35–37 and possibly differences in values for end-of-life care.
Historically, end-of-life care has been rooted in White middle class cultural and religious values,4,36 with its very different frame of reference, value system, and life experience compared with many AAs. 38 Where middle class Whites may emphasize individual choice, AA values support family-centered decision making. 7 Faith, spiritual beliefs, and guidance of a spiritual leader 36 are very meaningful to AAs, especially as they cope with illness and make treatment decisions.39,40 However, physicians rarely ask patients about their spirituality. 41 AAs rely on hope 42 and faith in God's healing power: 43 This can be at odds with physicians' felt need to share a terminal prognosis. 31
Inpatient PC consultations have identified unrecognized symptoms and unmet needs,44–48 and they have been associated with fewer intensive care unit (ICU) days49,50 and ICU deaths, 51 and improved care processes and higher rates of documentation of goals of care.29,30,52 However, lack of access to palliative consultations results in less availability of PC benefits to rural and minority patients.
Finally, and most significantly, historical and social factors, including slavery, racism, medical experimentation and exploitation,31,53 as well as ongoing racism and microaggressions, 54 have left a deep-seated legacy of mistrust in the AA community.55–57 A recent report 58 found that AAs and Whites were “worlds apart” in their perceptions of racial equality and actual gaps in household income. This is even more strongly felt in the “Deep South” where slavery was promoted. 59 A recent study 60 found that AAs are more likely than other racial groups to believe that physicians did not care about them as individuals, and were less likely to trust their physicians' judgment and personal competence.
The overall goal of this three-phase study was to develop and determine the feasibility of implementing a culturally based PC tele-consult program for rural Southern AAs and White elders with serious illness and their families, and assess its acceptability to patients, their family members, and clinicians. The aims by phase were: Phase 1: To determine cultural values and preferences of each ethnic group and ascertain ethnic group commonalities and differences. Phase 2: To develop a culturally based PC consult protocol across ethnic groups. Phase 3: To determine feasibility of program delivery, and acceptability to patients, caregivers, and clinicians, and patient/caregiver satisfaction with the culturally based consult.
Methods
The study was conducted at Beaufort Memorial Hospital (BMH) in Beaufort, SC. Beaufort County has a population of 175,852, and most of Beaufort County's census tracts are rural. 61 IRB approval for all three phases of the study was obtained from the University of South Carolina Institutional Review Board, and for Phase 3, from the Beaufort Memorial Hospital.
Study design
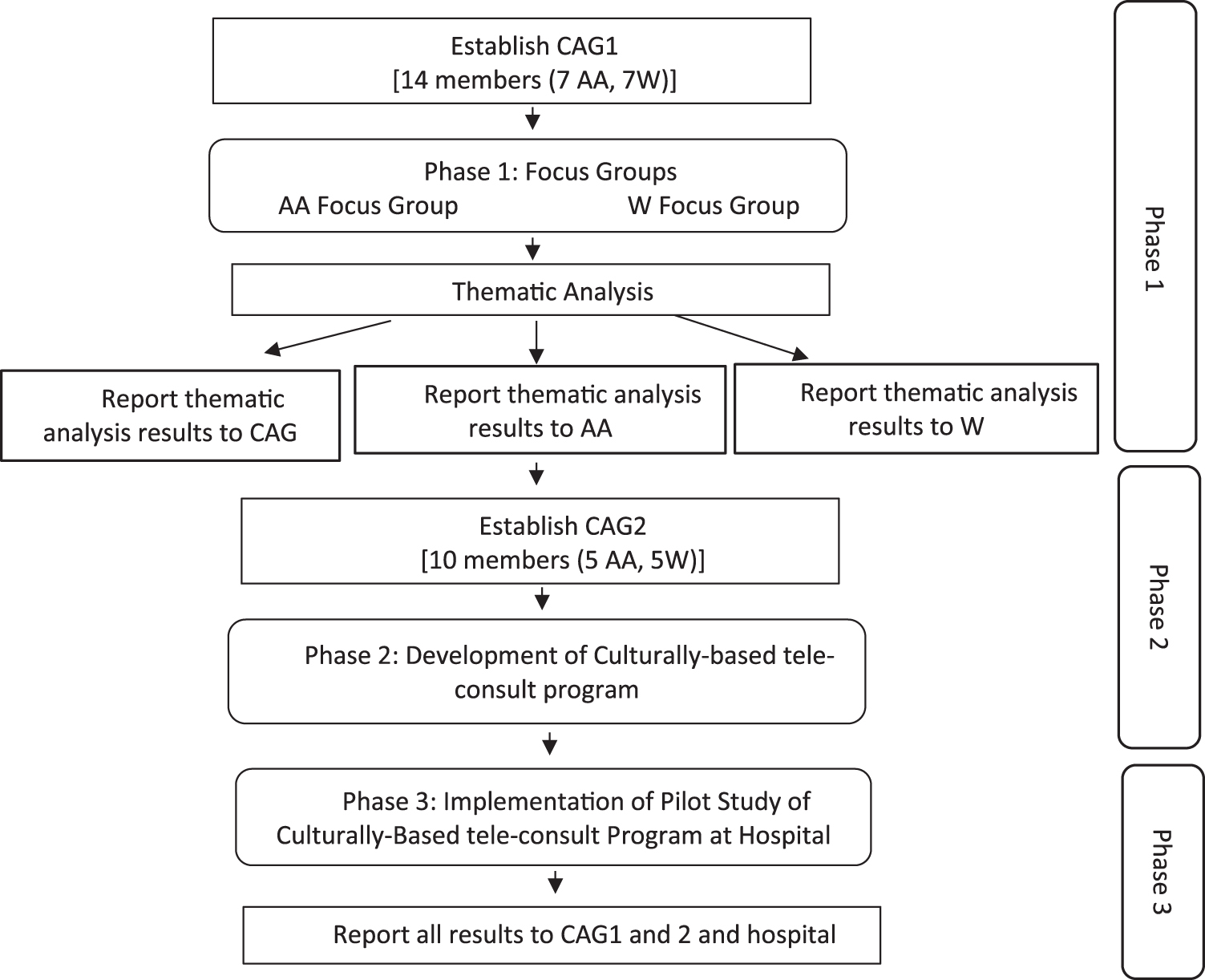
This three-phase study used Community Based Participatory Research (CBPR) methods and principles, as illustrated in Figure 1, to define the study protocol and identify feasibility of a culturally based PC consultation to improve PC access. CBPR, a public health method in which academia and the community form a joint partnership to address community issues, has been found to address health disparities62,63 and result in demonstrable positive health outcomes. 64
Study design.
CBPR builds on community strengths; the community is integral to all phases of the research, for the mutual benefit of all partners involved in the process, and in disseminating findings and knowledge to all partners. 65 Consumer input has been demonstrated to enhance both the quality and acceptability of interventions. CBPR has been recommended as a promising strategy for PC research that aligns with the priorities of stakeholders, as a means to deliver tailored and appropriate care to underserved communities. 66
Phase 1 engaged community members in the planning phase, serving as the first step in forming relationships and building trust with the community, and in obtaining community guidance into the study. Community Advisory Group (CAG) members were recruited with the assistance of the community health educator at BMH who had strong ties with community groups.
The CAG included equal numbers of AA (n=7) and White (n=7) members. The AA members were a county council member, leader of the Gullah Church Nurses Association, a pastor of a local AA church, a hospital employee, a hospice social worker, and a community member whose wife had recently died. White members included the nursing director of the BMH Cancer Center, its community health educator, a local social worker, two local hospice staff, and a community member whose loved one had recently died.
Phase 1: CAG planning and focus groups
The CAG planning meetings for Phase 1 (1.5 h each) were held over 2 months at BMH. The CAG members received an honorarium for their time ($25/meeting) and a gas card ($25/meeting) for travel.
Focus groups
In designing the research protocol, we chose focus groups as the most appropriate data gathering method for the study, as past research has suggested they provide an atmosphere that is the most conducive to respondents in sharing their personal experiences.67–69 We presented our rationale for this decision and elicited CAG feedback as to the appropriateness. CAG members were familiar with focus groups; this method had been widely used in Beaufort in an assessment of health care needs, 70 and considered this method appropriate. The CAG members provided input into culturally appropriate ways to recruit for, plan, and run the focus groups. The AA members strongly recommended holding separate focus groups by ethnicity, making it clear that AAs would be more comfortable and more likely to speak openly if focus groups were limited to AAs. As a result, we revised the original consent forms to hold separate focus groups.
CAG members designed the recruitment flyer, using a design that was considered appropriate for each community, and distributed these to churches, hospitals, hospices, and other community settings. Local newspapers were sent information, and the principal investigator (PI) and CAG members were interviewed for three articles published. The CAG-developed screening protocol was used to determine eligibility of potential callers. The CAG members recommended that focus groups be held in a well-respected but neutral space. Meeting dates and times were weekdays after 5:00 pm, lasting no more than an hour and a half, and included a light dinner.
Focus group inclusion criteria
To be eligible to participate in the focus group, respondents had to be a family member of a loved one aged 60 and older who had died in the previous 12 months after an illness of 3 or more months, and in whose care they had been involved. Both the family member and loved one had to be Beaufort County residents, and the loved one had to have been treated in Beaufort County (with the possibility of occasional visits to larger hospitals in Charleston or Savannah). Thirty-one focus group members were recruited (15 White and 16 AA) (Table 1). Two thirds were immediate family; all provided at least 3 h of care/day to their loved one, with half providing 12 or more h of care per day.
Phase 1: Demographics of Focus Group Participants
χ 2 (1, N=31)=4.21, p=0.040.
AA, African American.
Focus group guidelines
Focus groups were conducted separately by ethnic group. Facilitators were of the same ethnicity as the group they facilitated, consistent with focus group methodology and as has been used successfully elsewhere. 71 Planning meetings to develop the guidelines for the focus groups were held with the PI, two co-investigators (Co-Is), and the two facilitators. Both facilitators (one faculty member and one doctoral student) had received training in conducting focus groups. The protocol included ground rules (e.g., confidentiality), an explanation of why focus groups were being held separately, and the questions (and their probes) posed to focus group participants over the two meetings.
Questions were designed to focus on topics that impact end-of-life care. In this article, we focus on family members' preferences toward the care their loved one received in the 12 months before their death. Questions on this topic included: (1) “What did you find to be particularly helpful about the care or treatment your loved one received during their end-of-life care?” (2) “What did you like or not like about the way the healthcare staff communicated with your loved one/the family?” (3) “During the course of your loved one's illness, whose advice did you seek or who helped in making decisions about your loved one?” and (4) “During the end-of-life care experience with your loved one, whom among the healthcare staff did you trust?”
Focus group meetings
Two focus groups, a week apart, were held for each ethnic group at the local University in a comfortable meeting room. A light dinner was provided. The community health educator greeted each participant and introduced the PI and focus group facilitator. Respondents were presented with two IRB-approved study consent forms: the first to participate in the focus group study, and the second to be contacted for follow-up and potential participation in the next phase of the study. The facilitator started the meeting by introducing herself, the note takers, and the social worker who remained outside the room during all focus group meetings in case a participant(s) required professional support, and the two note takers sat at the back of the room.
Notes and tape recorders were transferred for storage in a locked, coded box to a locked data-storage room at the University. All tapes were transferred to Verbal Ink, a transcription firm. All transcriptions were kept on secured computers accessible only to the PI and study coordinator. All questionnaires were kept in locked university storage, with a unique identifier assigned to each questionnaire.
Data analysis
Analysis of the data followed standard procedures for qualitative data analysis;72,73 that is, systematic thematic analysis of transcripts identifying major and minor thematic areas; coding categories using open, axial, and selective coding; and sorting the data into coded categories, construct, and name typologies to describe family members' preferences for end-of-life care.67,68,73 A theme was defined as an issue raised or discussed by at least two or more members in that focus group. Themes were identified for coding based on the repetition of specific words, phrases and opinions, use of language and general thought patterns, as well as specific topics that dominated the focus group discussion.
Coding was conducted separately for each focus group meeting by two independent raters (R.E. and S.L.). Each independently reviewed and coded the data for themes, and then identified agreement. This was repeated for each of the four focus group meetings. In cases where there was no agreement, a discussion was held between the two raters and a Co-I (S.L.) experienced in focus group analysis, to reach consensus. Each agreed-upon theme and sub-theme was clearly defined, and several illustrative quotes were provided. Each theme was examined to determine whether it was similar across the two groups or whether it varied by group, and if so, in what way.
Report to CAG
After completion of the thematic analysis, results of each focus group were presented back separately to each of the focus groups, and all results were reported to CAG.
Phase 2: CAG planning and development of culturally based PC tele-consult
Expansion of CAG
To expand community input and to compensate for some CAG member withdrawal, the CAG was expanded to include six additional members, three from each of the focus groups (CAG2). Focus group members added were selected among participants who had agreed to be re-contacted, had participated fully in the focus group meetings, and who held varying perspectives and opinions on a range of topics.
CAG2 met monthly for 28 months with the research team, which included the study PI (R.E.), the PC physician (J.H.) who participated remotely via Go-To-Meeting, and the study coordinator. Meetings were held on a Thursday evening at BMH, and a light dinner was provided. The CAG2 members received the same reimbursement as in Phase 1.
Figure 2 illustrates the process used in developing the culturally based tele-consult. (1) First, the PC physician described the elements of a Standard Palliative Care Consult 20 to provide an overview of where the community recommendations would fit. (2) The CAG2 reviewed each of the Phase 1 themes, including sample quotes that illustrated each them. Following an overview of all the themes, each theme was reviewed and discussed individually. (3) For each theme, and for their ethnic group, CAG2 members recommended culturally appropriate programmatic recommendations for the culturally based PC consult that they were designing. If the theme applied to both groups equally, all members made these recommendations, and if it was applicable to one or other group only, members of that group made the recommendations. (4) All the recommendations were reviewed to ensure an accurate portrayal of what CAG2 recommended, and those that did, were written into a study protocol for the study team and the PC physician to adhere to. The group discussed those that were not accurately portrayed further, until the representation was accurate.

Phase 2 developing the culturally based PC tele-consult program. PC, palliative care.
Phase 3: CAG planning and implementation of the pilot study culturally based PC tele-consult
Few, if any, research studies take place in such small rural hospitals and a hospital “gatekeeper,” the Chief Nursing Officer, opened several doors to approach the hospital CEO. Approval was obtained from the hospital CEO, and after a formal presentation to their IRB, approval for this study was given. Presentations were made at hospitalists' meetings by the PC physician and the study PI on at least two occasions to explain the study aims and methods. Cards with eligibility criteria were created and handed out to all hospitalists. The Study Coordinator was present at the hospital every day and built relationships with floor nurses, to whom she explained the study and gave out eligibility cards.
Eligible patients were only approached after permission from the hospitalists was obtained by means of an order for a PC consult from the hospitalist. Based on CAG recommendations, CAG members were the first to meet the patient and family members to explain the study to them. If there was interest in the study, CAG members introduced the study coordinator who completed the consent process.
All PC tele-consults were conducted in the patient's hospital room at a time convenient to the patient and family members. The telehealth computer was brought in by the study coordinator who remained in the room with the family during the consult. After the consult, the PC physician charted his findings and recommendations, which hospitalists could review. The study coordinator alerted the hospitalist that the report was in the chart, and it was the hospitalists' decision whether to implement PC physician's additional recommendations if any were made.
Midway through Phase 3, to enhance hospitalists' referral and involvement, we implemented a system whereby the PC physician texted the hospitalist by using a secure health care communication method, after the consult and offered to discuss the consult by phone if the hospitalist wished.
Feasibility of program delivery, including its acceptability to patients, caregivers, and hospital staff, was assessed by using Donebedian's Structure-Process-Outcome model. 74 In this model, Structure examines the capacity of the care system (i.e., support of hospital staff and leadership, audiovisual equipment to access PC), Process evaluation addresses implementation fidelity to culturally based protocol, and Outcome evaluates acceptability of the program to patients and family and the effects of program on perceived patient and family satisfaction with the PC Consult (primary outcomes). Variables derived from this framework were measured through process evaluations (structure and process) and adaptation of FAMCARE-2 questionnaire (outcomes).
Results
Phase 1: focus groups
Calls to study hotline to participate in focus groups
Eighty-nine calls were received. Referral sources varied significantly between the two ethnic groups; the majority of Whites read about the study through articles in one of two local newspapers. Less than half of AAs called as a result of this source; most were referred directly by CAG members or through flyers placed in local churches by the CAG.
Exclusion
Eleven White callers and one AA did not meet eligibility criteria for focus group participation (primarily because their loved one had been treated in other parts of the United States).
Recruitment to focus groups
Due to higher than expected interest, we expanded our focus group numbers beyond our initially planned for 10 per group, and closed participation after consent was obtained from 15 Whites and 17 AAs.
Attendance at focus groups
All Whites (n=15) and all but one AA (n=16) who met eligibility criteria attended focus groups. There was considerable participation in both groups from all participants. Although a range of powerful emotions were shared, no one required the services of the social worker. Identifying data are presented in Table 1.
Relationships to loved ones varied significantly between the two groups. Most loved ones who had passed away in both groups were either parents or spouses, but there were more non-immediate family and friends in the AA group (i.e., great uncle, second cousin, godfather, and two close friends), supporting prior studies that document extended family members and fictive kin (unrelated by birth or marriage but with a significant relationship with the person, that are like a family member), as important members of AA families.75–77
Thematic analysis of focus group data
Ten themes, each with one or more sub-themes, emerged from the focus group data, and fell into two broad categories: (1) Experiences that patients and family members had at various treatment centers (physician offices, hospitals, hospices, nursing homes) during the care of their loved ones; for example, physician communication, pain medication; and (2) Cultural values, beliefs, and preferences; for example, the role of religion and church, family caregiving, cultural aspects of discussing death, and discussing prognosis.
Comparison of Themes Between Ethnic Groups: In eight of the themes, there were differences between the two ethnic groups within the sub-themes; one theme arose only among AAs (lack of trust) and one theme among Whites only (physician lack of respect for patients/family). All themes are described next.
Phase 1 themes and Phase 2 recommendations
As the recommendations made by the CAG in Phase 2 are built/depend directly on the themes in Phase 1, we present the results of both phases by the themes given next (Tables 2–11).
Theme: Lack of Trust in the Health Care System
CAG, Community Advisory Group.
Theme: Discomfort with Telehealth
Theme: Treat Family and Patient with Respect
Theme: Religion, Church, and Pastor
PC, palliative care.
Theme: Discussing Death and Prognosis
Theme: Family Caregiving for Patient
Theme: Hospice and Nursing Homes
pt, Patient.
Theme: Clarity About Opiate Dosage
Theme: Advanced Care Planning
ACP, Advanced Care Planning; AD, Advance Directive; DNR, do not resuscitate; ICU, intensive care unit.
Theme: Need for Services
Lack of trust in the health care system and in physicians was a theme in the AA group (Table 2). To build trust, CAG members suggested that they meet and greet AA patients and families first, introduce themselves, briefly describe the study and the consult, and explain that they were an integral part of the development of the protocol. Although the issue of lack of trust did not arise among White CAG members, they felt this would be beneficial for White patients too, and suggested they be the first to meet White patients and families.
To do this, CAG members had to become hospital volunteers and undergo volunteer training. All but one CAG members did so. The CAG also developed a colorful page about the study in which they used images of the ethnically diverse CAG working on the study, a photograph of the PC physician for this study, a computer with a person in a bed talking to a patient, and a simplified illustration of the data to be collected, which they would share with the patient and family.
Telehealth, the remote delivery of health care and sharing of medical knowledge using telecommunication, has been used to deliver health care to remote areas,78–84 and it was the method by which this consult was conducted primarily due to the health professionals' shortage (including PC services) in the rural South, together with large geographical distances in rural areas. Since this method was not widely used in local health care settings, we anticipated that community members might be unfamiliar with it. We therefore, raised the issue in the focus groups to hear how community members felt about it and what their suggestions were for a reduction in potential community concern. Recommendations made to overcome this discomfort were the same for both ethnic groups and included the PC physician wearing a white coat (to indicate that he/she is a physician), as well as the PC physician acknowledging the inability to be physically close to one another. They also requested that a family member be in the room, and, to ensure continuity of care between the tele-consult and hospitalists, that the study coordinator be present (Table 3).
A theme that arose in the White focus group was their experiences of physicians acting with a lack of sensitivity, outright rudeness, and/or not respecting confidentiality (Table 4). Although this was not raised by the AA patients, both ethnic groups strongly endorsed the recommendation that the PC physician conducting the consult would always treat the family and patient courteously, and never violate patient confidentiality.
Table 5 highlights a significant cultural value that impacts both ethnic groups, the role of religion and church in the lives of both ethnic groups. Although religion and church was important to both groups, in the AA group, religion was considered the source of all comfort, with the church serving as the center of all aspects of community and personal life. The pastor played a key role in helping family members accept the reality of the impending death in both groups. A difference occurred in terms of support: In the White group, it was the church members that provided support; whereas in the AA community, family was key (as seen in Table 7).
Table 6 highlights a core cultural value of the AA group, and that is that the family takes care of their loved one, regardless of the sacrifices it requires. “It's the way we was taught. We just take care of one another.” Sending a loved one to a nursing home was considered unacceptable among the AA group, and only one CAG member had a loved one in a nursing home, due to the patient having Alzheimer's and continually running away, requiring her to be in an enclosed environment. This has implications for the physician referring patients to home hospice or nursing homes (see also Table 8) where nurses or other professionals will come into the home.
Three themes about death and dying emerged in the AA focus group, all of which are tied to church teachings and doctrine. Death and impending death were not talked or preached about in church, and consequently, not discussed in community members' homes; the concept of maintaining hope, a fundamental aspect of faith, was reflected in names of AA churches, in pastoral messages, and in community songs, and the unshakeable belief that whatever happens to the patient is in God's hands.
Based on these concepts, the CAG asked physicians to understand these concepts, recognize them as important, approach the concept of death and dying with great caution, and explain that the decision was in “God's hands.” If the physician was uncomfortable with “God,” CAG requested that the physicians say, “It's in the hands of a higher power.”
Specific guidelines for sharing prognosis with AAs included never telling the patient that he/she is dying, under no circumstances specifying time until death, explaining what is taking place in the patient's body in non-medical terms, and always stating that the decision lies “in God's hands.” Sharing the prognosis in an insensitive, disrespectful manner or sharing it with a patient when the caregiver asks for it not to be shared by the physician were concerns raised in the White focus groups. Recommendations, therefore, included physicians respecting privacy and not sharing prognosis in a public space and/or in front of non-family members, and asking family whether they wanted to know the prognosis and then respecting their choice.
Although the word “hospice” was associated with death in both ethnic groups, in the AA group it also raised fears of strangers, White people coming into their home, and taking over. There was recognition that the AA community could benefit with education about hospice and what it offered. The AAs that had used hospice services in the care of their loved ones found some of its services, especially the support of the patient and caregiver, very beneficial. In addition to these two areas of support, the White group reported receiving support by the hospice chaplain, and support by hospice staff after the death of their loved ones. In the AA group, support was provided by the family church's pastor and family members.
Because of the concerns in both groups about the association of hospice, CAG recommendations included not using the word “hospice.” In the AA group, the physicians were asked not to raise the issue of home care unless the family asked for assistance and even then, were requested to provide reassurance that the hospice staff are not there to take over, and the family will remain in charge of taking care of their loved ones (Table 9).
Confusion between the various documents such as Advanced Care Planning, Advance Directive, Health care Power of Attorney, and Do Not Resuscitate occurred in both groups. Although only a few White focus group members had an Advanced Directive, several had seen or been asked about one. This was not the case in the AA group; here was an expressed understanding of knowing what the loved one wanted in terms of care, because the loved one had often shared it verbally with a family member, and that family member wanted to do whatever the loved one had expressed (Table 10).
An issue of concern that arose among members of both ethnic groups was lack of clarity about the administration of morphine, especially the dosage since that did not always follow usual medication regimens, as well as the possibility of lack of consciousness, and even death. The CAG members therefore made recommendations that would clearly explain this to the caregivers.
Table 11 indicates the perceived lack of needed services for those living in the rural South, such as need for specialized services for military personnel. Although the need for financial assistance for those in need was present in both groups, it was clear that in the AA group there was a lack of awareness about services that were already available in the community. This inspired the AA CAG members to create a booklet describing available services, designed specifically for older AAs, using large font and photographs of AAs using these services. These booklets were widely distributed in the AA community.
Table 12 summarizes all the recommendations for the culturally based PC consult, and it is presented side by side with the National Palliative Care Guidelines for a PC consult. 20 It includes all the themes and clearly specifies which culturally based aspects are relevant to White or AA patients and families or to both groups. This is the guiding protocol that was used by the PC physician (as well as the study coordinator) to guide the PC consult in Phase 3.
Consult Guidelines: Culturally Based Compared to National Consensus Project Guidelines
Numbering listed per NCP guidelines.
ACD, Advance Care Directives; W, White.
Phase 3: implementation
Phase 3 Study Flow is illustrated in Figure 3.

Protocol implementation.
Although 6 months were originally allotted for Phase 3, reluctantly we had to half this to 3 months as a result of the unexpected delay before the PC physician, who is from another state, received his SC medical license. (At the time of study implementation, there were no PC physicians in SC.)
Program implementation: structure-process-outcome
Structure
(1) Support from Hospital Leadership was high as indicated by permitting the study to be conducted at the BMH and by receiving IRB approval from the hospital IRB; and (2) referral by hospitalists: only 18 out of 28 eligible patients were referred to the study by hospitalists.
When several calls from the Study Coordinator to hospitalists informing them of an eligible patient were either not returned and/or a consult was not prescribed, we identified this as a barrier. After a discussion between the PC physician and the chief hospitalist, the protocol was changed. The hospitalist granted permission to text them directly to let them know a patient was eligible, requesting that they opt out if they did not want to patient to be included. After this protocol revision, (a) there was an increase in referrals (in the 14 weeks pre-protocol change, there were 8 referrals [
Process
(1) Implementation fidelity: adherence to the study protocol by the PC Physician was determined based on a checklist of 30 protocol-determined items that were to be adhered to during the tele-PC consult. The PC physician scored 30 out of 30 for six consults and missed one item only on three consults (once was not acknowledging the telemedicine, and twice not asking the patient whether they would like to speak to a pastor). (2) Follow through by the patient's physician on the PC physician's recommendations: The PC physician made specific recommendations for patient care in four instances (in five other cases there were no additional recommendations in addition to the care the patient was already receiving). Hospitalists followed recommendations in three of the four instances.
Outcome
(1) Participation rate: All 16 eligible patients approached were too ill or non-communicative and unable to provide consent; therefore, family caregivers were invited to participate in the study. Nine caregivers (six AA and three White) consented, and seven declined (three AA and four White), that is, the reach was 9 out of 16 (56%). (2) Family satisfaction was assessed by using the FAMCARE-2 (family members) 85 designed to assess family member satisfaction with care received by PC teams. This 17-item instrument is designed to measure family satisfaction with a PC program; since this was only a consult, many of the questions were not applicable (e.g., speed with which symptoms were treated, way in which physical needs for comfort were met, etc.). We therefore present responses to the 10 questions that were applicable (Table 13). Patient satisfaction was not assessed, as almost all the patients were non-verbal or non-communicative during their hospitalization. In all the applicable questions, there was a high degree of satisfaction (either satisfied or very satisfied) with the PC consult. Additional comments made by family members included “He helped her to respect herself”; “How can I say it? He is just wonderful, I am so thankful”; and “talking with him gave us peace of mind.”
Modified FAMCARE-2: Selected Questions
S, satisfied; VS, very satisfied.
Discussion
The aim of this study was to develop a culturally based PC tele-consult for and by rural, southern AA, and White communities and to test the feasibility of implementation. The program was feasible to both develop and implement. The main implementation challenge was the lower than expected referral by hospitalists. Although this improved after a change in protocol in which they were texted when a patient was eligible, it is clear that getting full buy-in from hospitalists, in addition to leadership and nurses, is essential in conducting hospital-based studies in small, rural hospitals.
This study is the first in the United States to have developed an ethnic-group specific, culturally based palliative consult intervention by and for rural, southern White and Africans elders with serious illness. In contrast to the existing model of end-of-life care that is based on White, middle class cultural and religious values,1–3 this model was designed to address the unique cultural values, beliefs, frame of reference, and preferences for communication and care of each ethnic group.
Differences between the two groups were evident in most of the themes (8 of the 10). Based on their ethnic group's themes, community members from that group specified ethnic-group-appropriate communication strategies, later incorporated into an ethnic-group-specific protocol, which the consultant used when conducting PC consults.
Two key cultural values in caring for a loved one with a serious illness emerged: (1) the integral role of faith, religion, and church; and (2) the role of family in caregiving, with both similarities and variations between the two ethnic groups. The South is commonly referred to as the land of the Bible belt, a place where the population is profoundly religious, with widespread religious practice and deeply held beliefs 86 ; however, the separation between the White and AA church that began with the creation of separate AA churches in the 1880s after the Civil War remains in effect today. 87
Although both groups reported on the importance of religion and church, for the AA community the church was considered the source of all comfort and learning, and the center of community life, spiritually, socially, and culturally, a finding widely acknowledged by Southern religious study experts 87 who consider the church as the most important institution in the AA culture. 88 In both ethnic groups, it was the pastor who played a key role in helping the patient and family accept impending death.
In the AA community, the pastor is traditionally considered the leader of the community, to whom community members look for guidance. 89 The need to have the presence of a spiritual leader actively present to participate in treatment decision making and in discussing end-of-life issues with the patient and families has been reported in a prior study. 56 “Living your life in faith, each and every day,” as expressed by the AA pastor on this study's CAG highlights the key role of faith and trust in the power of God in the AA community, at all times, especially during the final stages of life. A similar finding was described by Johnson et al. 90 in which three aspects of faith during the dying process were described by an AA participant: (1) trust in the power of God to take care of the person, (2) recognition that death is the beginning of a new life, and (3) belief in a better life with Jesus after death. Based on this faith, AA CAG members highlighted the importance of the clinician saying, “It's in God's hands” when discussing prognosis with an AA patient and/or family members.
“It's the way we was taught. We just take care of one another,” as explained by a CAG member, highlights another core value in the AA group. In her review of the caregiving field, comparing AAs and Whites, Dilworth-Anderson et al., 2002, found that experiences and outcomes of caregiving varied across racial and ethnic groups. 91
Reasons for providing care to older relatives also differed between the groups, leading to the conclusion that cultural values and beliefs serve as the lens through which caregiving is experienced.92–94 Suggested reasons for the high value that AAs place on care of family members are rooted in history where no outside care was available, and family networks served as systems of social service, welfare, and community-based interventions. 95
Study strengths and limitations
Relying on CBPR as our study's guiding principle, with community members from each ethnic groups being integral to all phases of the study, resulted in the shaping of the study in ways that enhanced the study. The unequivocal recommendations by the AA members of the CAG to conduct separate focus groups (Phase 1) permitted a detailed comparison between the two groups. The ethnic-group-specific recommendations for the tele-PC consult (Phase 2) resulted in the creation of first ethnic-group-specific PC consult protocol; and in Phase 3 the initial introduction of the study to patients and family by CAG members who had created and shaped the consult to meet the cultural values of each group was warmly received by patients and family in both groups.
The dedication of the CAG members to the lengthy commitment (program design required monthly meetings over 28 months) was remarkable; only 1 of the 12 CAG members missed a meeting (a recent widow, her marriage to a widower overlapped with a meeting). The CBPR process also resulted in a strong sense of both community's commitment to, and ownership of, the process, as well as the development of friendships among CAG members. 96
This study has several limitations. First, it took part in one site in one southern rural state, and only focused on White and AA communities, therefore limiting generalizability beyond the rural south or to other ethnic groups. The period for testing the culturally based protocol (Phase 3) was shorter than anticipated and limited the testing of the short-term efficacy of this model.
However, the effectiveness of this model is now being tested in a randomized clinical trial (RCT; R01NR017181) in rural hospitals in three Southern states (Mississippi, Alabama, and South Carolina) in which this culturally based program, in addition to standard care, is being compared with standard care alone. Additional outcome measures are included in this trial—patient symptom burden, patient and caregiver quality of life, family satisfaction with PC, patient feeling heard and understood, caregiver burden, and resource utilization. Since referral of patients by hospitalists was the main challenge in this study, in the RCT we have partnered with hospitalists at each of the three rural sites. Beaufort CAG members play a critical role in the trial; they have trained the four PC physicians who will be using the culturally based PC intervention and have provided guidance and inspiration to the CAG members at each of the three participating sites.
Health equity implications
The first culturally based PC consult program in the United States was developed by using CBPR, in partnership with AA and White southern rural community members. This three-phase method can serve as a model that can be replicated and adapted to other settings and with other ethnic groups; replication studies of Phase 1 are currently underway in Ghana and in Puerto Rico to determine the cultural values and preferences for care of loved ones with serious illness, of people living in those countries and cultures, another first step toward designing culturally based PC interventions by using the model developed in this study.
Footnotes
Acknowledgments
The authors with to express their deep appreciation to all the members of the two CAGs: Gardenia Simmons-White, Kenneth Clyburn, Gerald Dawon, Heidi Owen, Sara Nolette, Nancy Stewart, Peggy Hitchcox, Dixie Slichter, Kevrin Simmons, Gloria Ward, Debbie Covington, Jonnie Grant, Rachel Martin, Barbara Copeland, Burton Sauls, Marius Payne, Pastor Michael Williams, and Shawnell Williams—without whom this work would not have been possible. Special thanks are due to Cynthia Coburn Smith, MS, Manager of Community Health Improvement Program, Life Fit Wellness Services, BMH, and Connie Duke, RN, Director of Cancer Services, BMH and Keyserling Cancer Center, both of whom served as CAG members and collaborated on all the logistics of this study; and to BMH, who opened the doors to permit the authors to conduct this study at their hospital. The authors are grateful to Laura Reparaz, study coordinator, whose patience and kindness was appreciated by all; to Dr. Kristen Allen Watts, for her meticulous attention to detail and accuracy in drafting this paper's tables and figures. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by National Institutes of Health (National Institute on Aging [R21AG046772]), SCTR (South Carolina Clinical and Translational Research [Medical University of South Carolina]), and ASPIRE (Advanced Support for Innovative Research Excellence). National Institutes of Health (National Institutes on Nursing Research [R017181]) is based on the findings of this study.