
Abstract
Background:
Urban African American adolescents and young adults (AYAs) face multiple barriers to effective engagement in health care, including access to primary and specialty care services resulting in significant disparities in care.
Purpose:
To conduct a needs assessment to enhance service delivery of AYAs at an urban federally qualified health center (FQHC) organization in Detroit.
Methods:
Semistructured interviews were conducted among pediatric staff members (N=11) using the community needs assessment approach specified for FQHCs.
Results:
The needs assessment determined the following priorities for AYAs seeking care at this FQHC organization: (1) mental health (e.g., depression and anxiety), (2) obesity, and (3) sexual health (e.g., sexually transmitted infection testing).
Conclusion:
When analyzing a population to learn about community-based issues, a needs assessment is a valuable tool. The information here has been used as supplemental information to address the health inequities that African American youth face within Detroit.
Introduction
Urban African American adolescents and young adults (AYAs) face multiple barriers to effective engagement in health care, resulting in significant disparities in care. For example, sexually transmitted infection (STI) rates are disproportionately high among African American AYAs aged 15–24 years.1,2 They also face many barriers to reproductive health care and health education, including inadequate STI screening by health care providers, lack of transportation, and limited access to insurance coverage.3–6 The purpose of this brief is to define high-priority issues of an AYA community, describe the community needs assessment (CNA) process, determine the resources available to address these problems, and enhance service delivery among this population at an urban school linked federally qualified health center (FQHC).
A CNA is a useful tool for identifying the strengths and resources a community has for addressing the social and health care needs of its members and must be culturally sensitive.7,8 FQHCs must perform a CNA every 3 years to accurately document the needs of the communities they serve and to receive federal designation funding for this purpose.9,10 According to Health Resources and Service Administration (HRSA) guidelines, these health centers may also focus on underserved subsets of their overall populations (e.g., children, elderly people, and people with HIV/AIDS); as well as their mission that is to improve the health status of marginalized communities and advocate for high-quality care.8,9,11
Methods
The information gathered here was a part of a more extensive organization-wide CNA comprising seven FQHC ambulatory health centers in the city of Detroit, serving medically underserved populations. From the larger CNA, a total of 42 employees were interviewed by medical specialty as well as 460 patient satisfaction surveys were included to look at the population's health priorities, preferences regarding care, and the vital role that FQHCs play within the community. The interview guide was developed from the HRSA Compliance Manual 9 and the University of Kansas Community Tool Box. 10 The questions were reviewed by the executive leadership and partnering faculty for content to ensure that they met HRSA requirements. A semistructured interview method was used. Open-ended questions were asked, with 19 items covering the history of the organization and community, the health care services offered, the leading health problems, the unique issues faced by adolescents, resources, assets, and the sustainability of the community. The voluntary interviews lasted ∼60 to 90 min. Responses were manually coded, then summarized for thematic analysis. The themes from the interviews were used to describe AYA-prioritized health issues, provider-perceived health issues of the AYAs community, resources needed at the clinic, utilization, barriers, and social determinants of health from a staff member perspective. IRB review was not required as the assessment was a requirement by HRSA and did not include any interaction with human subjects or access to identifiable private information.
Results
Eleven health care providers and staff members were interviewed. A summary of the predominant themes and notable responses from the staff are highlighted in Table 1.
Results from the Community Needs Assessment Interviews
CDC, Centers for Disease Control and Prevention; LGBTQ+, lesbian, gay, bisexual, transgender and queer/questioning +, OBGYN, obstetrics and gynecology; STI, sexually transmitted infection; WIC, women, infants, and children.
Top three perceived health care problems of adolescents
The three most prioritized health issues included mental and behavioral health, obesity, and sexual health (see Fig. 1). These problems were reported to be the most prevalent in African American, low-income, and sexual minority (lesbian, gay, bisexual, transgender, and queer/questioning) AYA populations. The number of AYA males who obtained these services was also disproportionate in comparison with AYA females. Approximately 70–75% of adolescents were stated affected by sexual health issues, and more than half are affected by obesity or related chronic conditions such as hypertension.
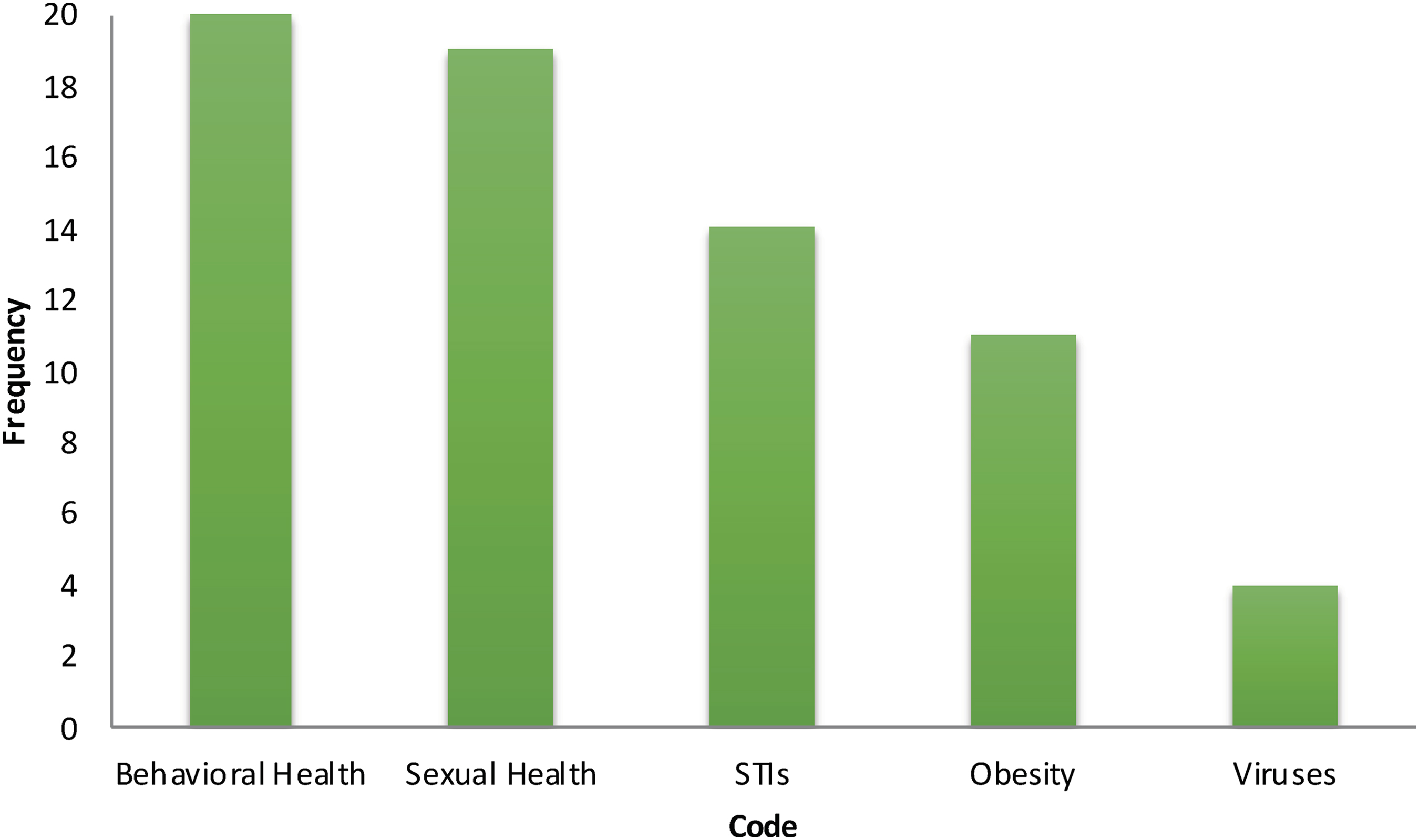
Adolescents and young adults prioritized health issues. STI, sexually transmitted infections.
Behavioral health screenings were a priority for providers. Anxiety and depression were diagnosed frequently in AYA patients, which is said to be due to a number of social determinants. Conversations about mental and behavioral health between patients and providers were usually initiated after results are reviewed from screening tools such as the Patient Health Questionnaire (PHQ)-2, PHQ-9, and rapid assessment for adolescent preventive services survey.
Marijuana and vaping were indicated to be one of the most frequently used drugs among patients. It was noted that marijuana was having a more significant impact on this population than anticipated. It was also reported through community forums, and discussions with patients, family members, teachers, and coaches, that are securing employment had been affected by positive screening results. Reduced performance on school examinations, difficulty maintaining attention, and delayed problem-solving abilities were also evident. The interviews also indicated that increased risk-taking, poor judgment, and consent problems arose with marijuana use.
Risk factors for health problems in AYAs
Risk factors found from the interviews in this community, poor public transit systems, safety, and assistance having prescriptions filled at local pharmacies minutes away from the clinic, are among the social determinants of quality of care for this population. The assessment also indicated that anxiety and depression are heightened in adolescents who live in poverty or are economically disadvantaged. AYAs who live in shelters and are consistently unsure when they will have money or food undoubtedly experience higher levels of stress. The interviews indicated that living in the urban environment of downtown Detroit was also not conducive to AYA health and contributed to risky behavior. One individual stated “adolescents are faced with the absence of jobs, failing schools, peer pressure, bullying, and gang-related violence, among other factors.” AYAs who must deal with anxiety, stress, and depression “often try to escape these feelings through engaging in risky behaviors like unsafe sex, unhealthy eating, and marijuana use.”
The CNA indicated that the lack of fresh food is a risk factor for obesity in this community. There are no grocery stores for miles around other than convenience stores that carry mainly snack foods and a supermarket chain store that specializes in organic food. The store above has been centrally located since 2013 and does offer a variety of healthy food choices; most people in the community cannot afford to shop there.
Staff perceptions
Providing holistic care, focusing on interpersonal and behavioral health of adolescents, and collaborating with individuals and organizations that are equally engaged and dedicated to community health were important to staff members. Solutions included additional staff training, partnering with Lyft or Uber to improve attendance at appointments; reinitiating the youth advisory council for feedback and advice; sharing case studies in pediatric provider meetings; interviewing the AYA population to tailor programs to them; and developing educational and health promotional materials to improve the health of this population.
Discussion
The CNA process provided an opportunity to be exposed to interprofessional teams and service-learning experience to undergraduate and graduate students in public health and nursing. Through conducting semistructured interviews, students were able to (1) understand the role structure and function of, and the population served by the health center and (2) evaluate experiences and approaches to working with diverse communities. 12 It also uncovered risk factors, health problems, and unhealthy behaviors among the AYA population that were similar to the current AYA health literature such as depression, homelessness, and nutrition and weight issues.1,13–15 A strength of the assessment is that the organization that this school-linked clinic provides services with extended hours and intensive care for sexual, reproductive, and fertility health, and behavior health, such as substance-abuse planning. Also, AYAs have access to care at this center regardless of their ability to pay. The center has a program that is funded to cover these costs, with a broad range of sliding scale health services, of which most patients utilize.
Our CNA does have limitations that include (1) small sample size, (2) perspectives from only providers and staff; AYAs themselves were not interviewed, and the results might have been different if AYA perspectives and opinions were incorporated, and (3) these results are not be generalizable to other populations. 14 CNAs are context specific and valid only for a given population, location, and time, so the results of this assessment may not be applicable to other populations. 14 To remedy these limitations, larger sample should be interviewed in the future. In addition, AYAs in the community should be interviewed to ensure that their perceptions of the community's needs align with those of the health care providers and staff members.
Conclusion
FQHCs play a significant role in improved geographic access in delivering comprehensive primary health services to individuals of all ages in underserved settings. 16 This assessment, along with future research, will serve as a guideline for the development and implementation of interventions aimed at promoting the use of community health centers and reducing gaps in care, specifically among young people in Detroit. The creation of this interview guide has helped to highlight a specialized population with unique needs, identify barriers that match the literature, as well as strengths and available resources within the organization and community: a process that may be replicated by staff within this larger FQHC organization. The results of this CNA have been disseminated to community members and stakeholders. Funding and IRB approval have been received to look at the data through a mixed-methods lens, specifically at young men's reproductive health called the Stay Safe Project.
Footnotes
Acknowledgments
A special thank you to the Detroit Community Health Connection staff and executive leadership for their service and commitment to this project.
Implications and Contributions Statement
This information is crucial as FQHCs play a pivotal role in shaping our health care system and address the public health needs that may impact the care of under-resourced populations. The findings identified from this community needs assessment have helped to define high priority issues among urban adolescent and young adults.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.