
Abstract
Introduction:
Physician incentives have been shown to reduce socioeconomic disparities in health care. The impact on sex/gender inequalities, however, has rarely been investigated. Using population-based data, this study investigated sex/gender differences in depression care and the impact of physician incentives.
Methods:
Deidentified health data from physician claims, hospitals, vital statistics, prescription database, and insurance plan registries in British Columbia, Canada, were examined, retrospectively. Individuals with depression were identified and their use of mental health services was tracked for 12 months following initial diagnosis. The following indicators were assessed: (1) counseling/psychotherapy (CP), (2) minimally adequate counseling/psychotherapy (MACP), (3) antidepressant therapy (AT), and (4) minimally adequate antidepressant therapy (MAAT). Sex/gender differences in these indicators before (January 2005–December 2007) and after (January 2008–December 2012) the introduction of physician incentives were estimated using interrupted time series analysis.
Results:
Preintervention, the percentage of individuals with depression who received CP was higher among males (CP: 58.4%, MACP: 13.6%) than females (CP: 57.1%, MACP: 10.9%). In contrast, the percentage who received AT was higher among females (AT: 57.7%, MAAT: 47.4%) than males (AT: 53.6%, MAAT: 41.9%). These statistically significant sex/gender differences remain unchanged postintervention.
Conclusions:
Sex/gender differences in depression care persist despite the introduction of physician incentives.
Introduction
Financial incentives have long been used, often with modest results, to improve the quality of health care.1–3 An important component of health care quality is equity in access to and use of health services,4,5 although it is seldom examined as an end-point in many quality improvement initiatives that feature financial incentives as a core component.6,7 It is important to examine the impact of financial incentives primarily because of the huge public investments they entail,8,9 and also because of concerns that such interventions may exacerbate, rather than reduce existing health disparities.10–12
In previous studies, the disparities that have been examined in relation to the introduction of financial incentives include those based on age, sex, ethnicity, race, and socioeconomic status.13–15 These studies, mostly from the United Kingdom and the United States where financial incentives have been used extensively, showed that incentives have had modest or no impact at all on addressing existing disparities.13–15 Where it looked promising, the evidence points to a potential role for financial incentives in narrowing the gap between people residing in geographic areas that are low and high in measures of deprivation by facilitating increased use of health services in the latter group. 16
In Canada, the use of financial incentives as a tool for improving mental health care was tested via a “natural experiment” in the province of British Columbia (BC). As part of its overall strategy to improve primary health care, BC deliberately avoided changing the way primary health care services are delivered, in direct contrast to what other Canadian provinces, such as Quebec and Ontario, have done. 17 Instead of structural changes, BC rolled out a suite of financial incentives that target physicians who provide care to individuals with various health conditions, including mental health. Proponents of these operational enhancements believed that these will stem the decline in family practice that started in the mid-1990s and peaked in the mid-2000—a period marked by high levels of disenchantment among general practitioners (GPs) due to dissatisfaction with remuneration, workload complexity, and relationship with the provincial government. 17
A study that examined specifically the impact of introducing physician incentives in BC on mental health services delivered in primary care settings has shown that providing physician incentives can change the pattern of access to depression care at the population level, although the magnitude of the estimated impact was modest. 18 The study found that the proportion of individuals who accessed psychological therapy increased, while the proportion of those who filled antidepressant prescriptions declined over the study period. The study also found that physician continuity of care, an indicator that measures whether patients see the same physician for outpatient care, ceased to decline after the incentives were introduced. 18
Whether the introduction of physician incentives in BC has changed disparities in the use of mental health care has never been examined. Among the health inequities that can be examined are sex/gender disparities, which need to be examined given the robust association between gender and mental health. Of particular interest is depression, which has higher incidence and prevalence among women than men. 19 Sex/gender differences in the use of effective treatments for depression (i.e., psychological and antidepressant therapies) signal potential health inequities since existing evidence indicates that these treatment modalities are equally effective for both sexes/genders.20–22 Likewise, health inequities potentially exist if differences in patterns of use are incongruent with treatment preference, such as when women, for example, are found to be less likely than men to receive psychological therapy when most women actually prefer receiving psychological therapy to treat depression. 23
In this study, we investigated the impact of financial incentives on sex/gender disparities in depression care, using indicators that measure receipt of counseling/psychotherapy (CP); minimally adequate counseling/psychotherapy (MACP), defined as ≥4 sessions of CP; antidepressant therapy (AT); and minimally adequate antidepressant therapy (MAAT), defined as ≥84 days of AT.
Methods
Data
We examined deidentified and individual-level health data from virtually everyone in BC, excluding a small percentage (4%) of individuals whose health care is covered under federal jurisdiction (i.e., registered status Indians/aboriginals, veterans, federal penitentiary inmates, and members of the Royal Canadian Mounted Police). The databases we analyzed include the government-sponsored provincial health insurance registry, physician claims database, hospital database, outpatient prescription database, and the provincial death registry. A common study identifier generated by Population Data BC linked all these databases (Table 1). Permission to access data was provided by the BC Ministry of Health and the BC College of Pharmacists. The Behavioral Research Ethics Board of the University of British Columbia granted ethics approval for the study (UBC BREB No. H14-00847).
Data Sources and Data Fields Used in the Study
BC, British Columbia.
Study cohort
We identified cohorts of males and females, older than 18 years, who received new major depressive disorder diagnoses in each of the months between January 2005 and December 2012. Depression diagnoses were ascertained through the primary diagnoses associated with a physician visit or hospital discharge. This is a valid method of identifying depression cases, especially when used in a population-level analysis.24,25 Details of how the monthly cohorts were derived from the linked data have been previously described.18,26
Outcome variables
To investigate changes in mental health service use over a period of 8 years, we examined receipt of the following: (1) one or more sessions of counseling or psychotherapy; (2) MACP, defined as 4 or more CP sessions; (3) one or more filled prescriptions for an antidepressant; and (4) minimally adequate AT, defined as 84 or more days of AT. Criteria for these indicators were deemed met if services were received within 12 months following initial diagnosis of depression. 18
Explanatory variables
A primary variable of interest in this study is sex/gender. Currently, there are no definitive and universally accepted definitions of “gender” or “sex.” 27 Gender is typically regarded as a social construct defined by the roles, relationships, and behaviors of women and men, whereas sex is considered to be a physical construct linked to the biology or physiology of females and males. 27 Sex and gender are intricately and significantly related, and both are important when studying health outcomes. 28 In this study, we used the sex field (male/female) of the linked health administrative databases as a construct that captures aspects of both sex and gender.28–30 We used the term sex/gender throughout the article to underscore the large overlap between the two constructs and to indicate that the disparities we studied cannot be attributed solely to sex.
Another explanatory variable of interest is the introduction of physician incentives, which putatively influences population-level changes in the use of mental health services. Known as the Mental Health Initiative, 31 the policy was introduced in BC in January 1, 2008, with an initial budget of $8 million. 32 The overall aim of the policy was to remove the financial barriers that family physicians or GPs experience when managing patients with mental health issues. 33 The financial incentives were embedded in a revised fee-for-service schedule, allowing GPs who prepare comprehensive treatment plans to receive compensation for being a patient's major source of care. The revised fee schedule increased the number of billable CP sessions from 4 to 8 sessions per year, and introduced fee codes for coordinating with other health care providers or for conducting follow-ups by e-mail or telephone. 31
Analysis
We constructed monthly indicators for each of the four measures. Values for these indicators were calculated by dividing the total count of individuals who met criteria for an indicator in a given month by the total number of individuals with new diagnoses of depression in the same month, multiplied by 100.
To estimate the changes in the levels and trend before and after the intervention, we used ordinary least squares regression with Newey–West standard errors to account for potential autocorrelation.
34
The regression model has the following general form:
where
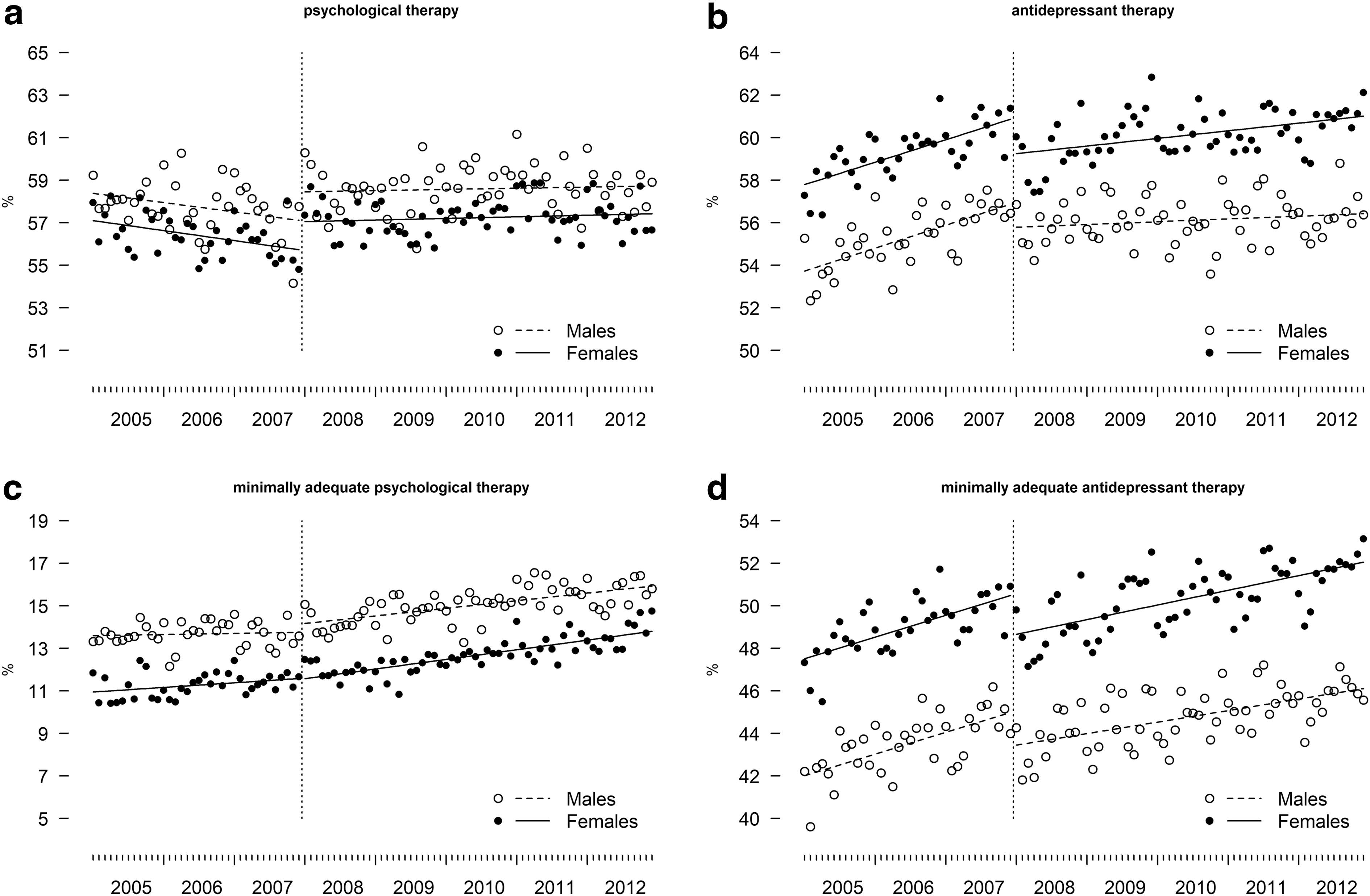
To facilitate understanding of the sex/gender disparities and any potential postintervention changes that occur either immediately or over time, we complemented our analyses with figures. For each indicator, we plotted data points, superimposed with separate regression lines for females and males. In these figures, distinct and clear separation in data points and regression lines between females and males are indicative of sex/gender differences. Parallel lines suggest persistent differences, while converging or diverging lines suggest decreasing or increasing differences.
We used SAS/SQL software version 9.4 to extract, link, and manage the multiyear data from multiple databases; Stata version 14.2 to run the regression analyses and obtain postestimation values; and R version 3.4.1 to generate the plots.
Results
During the study period, the mean number of individuals diagnosed with depression each year was 106,277 (standard deviation [SD]=5027; min=97,760; max=112,458). On average, about 65% of those diagnosed with depression were females (mean=69,529; SD=2447; min=65,070; max=72,723), while 35% were males (mean=36,749; SD=2744; min=32,690; max=39,735).
Counseling/psychotherapy
Sex/gender disparity in the receipt of CP was present and unaffected by the introduction of physician incentives. Results from the interrupted time series analysis did not show evidence of postintervention change in sex/gender disparities, either immediately (
Model Estimates of the Impact of Physician Incentives on Sex/Gender Disparities in Depression Care
The reported values represent percentages and 95% CIs. The regression formula with Newey–West standard errors is:
where
CI, confidence interval.
Figure 1a shows that the proportion of those who received at least one CP was higher among males than females in most of the months before the introduction of the intervention. There was also a decreasing trend in both gender groups, which was disrupted by the intervention. Despite the disruption, however, the parallel regression lines, representing the predicted average for males and females postintervention, indicate that the intervention had no impact on the prevailing disparities in the receipt of CP.
Sex/gender differences in
Minimally adequate counseling/psychotherapy
There was no evidence that the introduction of physician incentives changed the existing gender disparity (i.e., favoring males) in the receipt of CP. No meaningful change occurred immediately (
Compared with Figure 1a, the plot for this indicator (Fig. 1c) clearly showed a higher proportion of males receiving MACP throughout the study period. Preintervention there was a slight increasing trend for females but not males. Postintervention the trend was virtually the same for both groups. Overall, the parallel regression lines throughout the study period indicate the intervention's lack of impact on the existing disparities in the receipt of MACP.
Antidepressant therapy
The magnitude of the sex/gender disparity in the receipt of AT was greater than the sex/gender disparity in the receipt of counseling or psychotherapy. The results also did not indicate any meaningful change in disparity that occurred immediately (
Figure 1b shows that throughout the entire study period, the proportion of those who filled at least one prescription for antidepressants was higher among females than males. Postintervention the levels have decreased appreciably and the upward trend slackened. However, these changes occurred with about the same magnitude in both groups. The disparity in the receipt of AT between females and males remained virtually unaffected by the intervention.
Minimally adequate antidepressant therapy
Similar to the indicator for the receipt of AT, there was no evidence of postintervention change in the disparities between females and males in the receipt of MACP. Specifically, there were no meaningful changes in the magnitude of the disparity that occurred immediately (
Compared with Figure 1b, d shows a clearer and wider separation of the data points and regression lines that represent the proportion of females and males who receive MAAT. These suggest that the magnitude of gender disparity associated with receipt of MAAT is slightly greater than that found in the receipt of AT. Virtually identical changes in females and males, with respect to the postintervention levels and monthly trend, suggest that the impact of the intervention on gender disparity in the receipt of MAAT has largely been inconsequential.
Discussion
We sought to determine and estimate the impact of physician incentives on sex/gender differences in the receipt of psychological and antidepressant therapies. Our results show that although modest changes in the pattern of use for psychological and AT have occurred after physician incentives were introduced in 2008 in BC, sex/gender disparities in the use of these therapies were hardly impacted by the incentives. The proportion of those with depression who receive psychological therapy remained higher in males than females, while the proportion that receives antidepressants remained higher in females than males.
As this is the first study we know of that specifically examined the impact of financial incentives on sex/gender differences in depression care, direct comparison with previous findings is not possible. Generally, studies that assessed the impact of physician incentives on other sex/gender-based health inequities are scarce and the few that are published suggest no consistent pattern of impact. 13
In this study, we did not observe any significant exacerbation of sex/gender differences in the use of depression care after physician incentives were introduced. In previous studies, physician incentives have been reported to have the unintended consequence of increasing sex/gender-based health inequities. For example, the introduction of physician incentives under U.K.'s Quality and Outcomes Framework (QOF) in 2004 has been shown to result in women being less likely than men to be included in the recording of quality indicators for coronary heart disease 35 and diabetes. 36
While it may be argued that the physician incentives implemented in BC were not specifically intended to address health inequities, it would not be entirely unrealistic to expect physician incentives to have measurable effects toward reducing sex differences in depression care. Under certain circumstances, financial incentives can have a meaningful impact on reducing sex/gender-based health inequities, as shown, for example, in QOF studies that examined the impact of financial incentives on sex/gender differences in a number of care processes for stroke/transient ischemic attack, 37 and in indicators of success for smoking cessation/prevention programs. 38
A number of recommendations in the literature have been offered to help ensure that substantial public investments, such as physician incentives, contribute to better health care not just for the general population but also across subpopulations. It has been emphasized, for instance, the importance of not assuming that financial incentives intended to improve the quality of care overall will automatically result in equal benefits for everyone. 39 Health inequities can be impervious to the effects of financial incentives, as findings from this study illustrate. In some cases, financial incentives can exacerbate existing health inequities.7,35,36 Another recommendation is to include specific targets for reducing disparities, which may require collecting data stratified by subpopulations and reporting robust health inequity measures.6,39 Last, financial incentives could be designed to address patient-, provider-, health system-, and population-level factors that promote and sustain various types of health inequities. 6 In the case of sex/gender-based health inequalities, this requires a concerted, deliberate, and systematic approach to understanding the underlying processes or pathways that give rise to these disparities. 40
A few points warrant consideration when interpreting the study findings. First, our data on depression care represent services that are covered by public health insurance. Second, we were unable to examine the appropriateness of CP provided by physicians due to lack of relevant data. Third, the results regarding the use of AT were based on records of prescription fills, which can underestimate prescribing rates or overestimate actual use. Last, we were limited to using sex as a variable for assessing sex/gender differences because sex is the closest representation of gender that we can derive from health administrative data. As a consequence, our analyses considered gender as a dichotomous variable, even though it is more appropriately examined as a spectrum 41 particularly in the context of health care inequalities.
Footnotes
Acknowledgments
Permission to use the linked health administrative data was granted by the BC Ministry of Health, Data Stewardship Committee, and BC Vital Statistics Agency. Data access was facilitated by Population Data BC.
Disclaimer
All inferences, opinions, and conclusions draw in this article are those of the authors and do not reflect the opinions or policies of the Data Stewards and any of the other agencies mentioned.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Dr. J.H.P. was supported by a Banting and Best Doctoral Research Award from the Canadian Institutes of Health Research, and a UBC Four-Year Fellowship Award.