
Abstract

The Secretary of Health and Human Services recently outlined a powerful vision for transformation of the healthcare system. 1 The Center for Medicare & Medicaid Services (CMS) plans to move 50% of spending to alternative payment models (i.e., Accountable Care Organizations [ACO]) by 2018. While policy makers debate ways to reduce healthcare expenditures, and industry searches for ways to increase profit, we must remember that from the patient perspective, the most important aspect of healthcare is easy access to care at an affordable cost. 2 Patients have demonstrated their priorities and preferences with their feet and their wallets. While primary care visits are falling, patients made more than 130 million emergency department and 160 million urgent care visits last year; retail pharmacies have entered the healthcare space; and telemedicine is expected to grow to a $30 billion industry by 2020.3–5
Let's Move Past the “Appropriateness” Debate
This growth of “convenience care,” in which undifferentiated or infrequent patients are opting out of the traditional primary care system, coincides with increasing attention to reducing “inappropriate” use. Payors have expanded their focus from the individual (e.g., targeting those with high-cost conditions or utilization patterns) to the care setting (e.g., discouraging the use of high-cost settings, such as the emergency department, for anyone with noncritical illness or injury). Developing novel tools to manage patients with complex and costly conditions, however, fails to increase healthcare's accessibility for the majority of Americans.
Conceptual Model for the Path Forward
In an ideal world, medical advice and healthcare would be available whenever and wherever patients are sick, injured, or scared. We present one conceptual model that provides patient-centered, easily accessible care throughout the whole continuum of health (see Figure 1). Although this model originated at a single hospital system, we feel that it has wide applications. Nationally, most efforts focus on the right side of the model—areas that are high cost for payors, but that are less common for patients. The left side has the potential to make a larger impact on day-to-day life and healthcare experience for the majority of Americans.
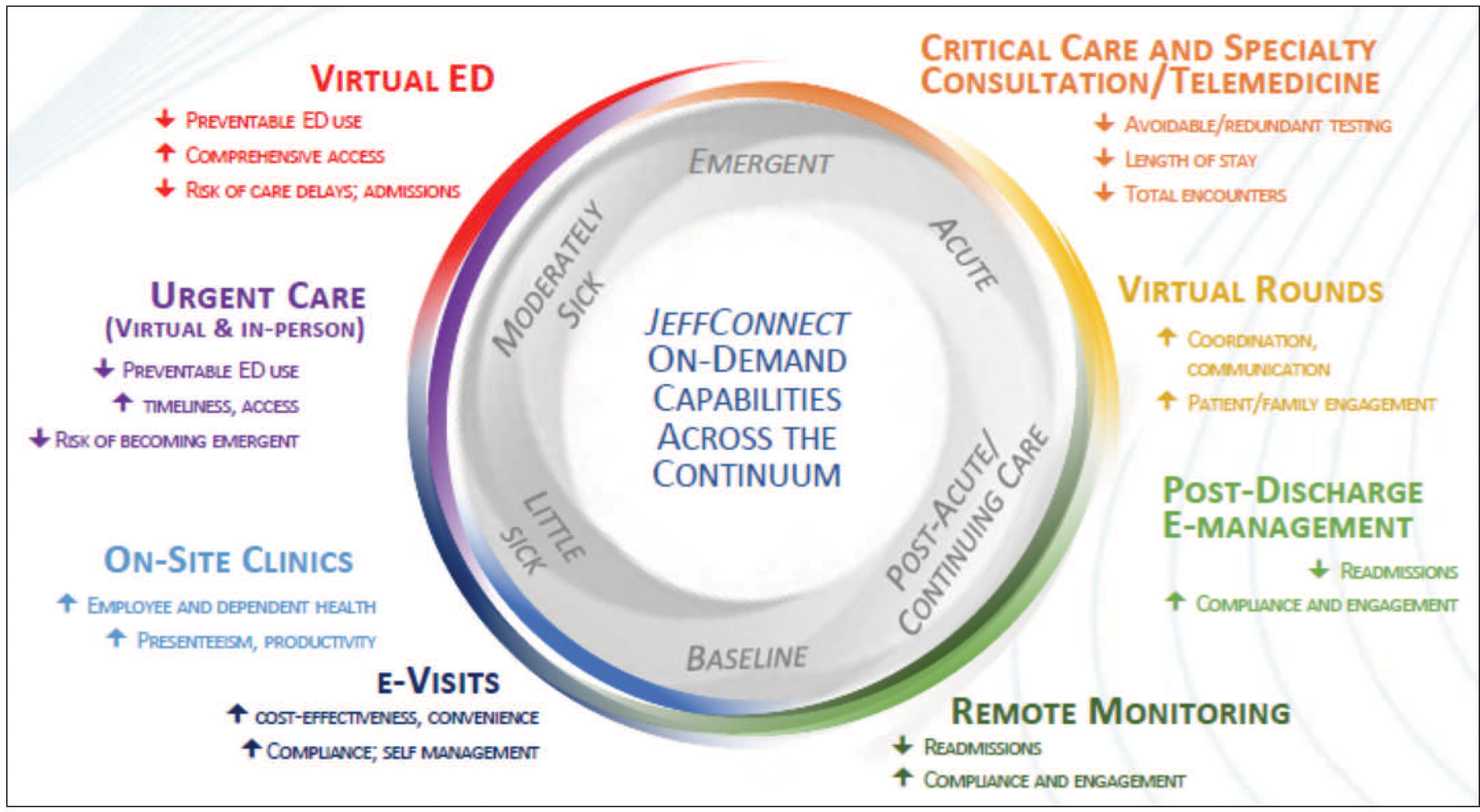
Model of patient-centered care across the care continuum. Patients previously well or at their baseline begin to feel a little sick. Solutions to enhance the likelihood of patients receiving earlier interventions exist throughout the continuum. ED, emergency department.
The Left Side of the Wheel
The “little sick”
In this conceptual model, individuals are usually at their baseline (bottom of Fig. 1). Patients who fall off their baseline and become “a little sick”—a sore throat, a new pain—can be treated either by (a) their own provider, through asynchronous communication, telephone consultation, or scheduled e-visit; or (b) an on-demand physician who is available 24/7 to provide virtual care. To avoid fragmenting care, these “available-ists” should coordinate care with a patient's other providers, and should have access to the patient's medical record regardless of where they typically receive their healthcare. In theory, patients who utilize the emergency department or urgent care because of the convenience may choose less costly options if these options were as convenient. Adding imaging and laboratory testing onto on-demand video visits (thereby creating a virtual emergency department[ED]) could further align patient and payor goals. Easy availability of evidence-based expert care when patients are afraid or uncertain is more likely to shift patient behavior than focusing solely on financial disincentives for health systems.

Emergency department care
Despite innovation in the approach to caring for those who are “a little sick,” some patients will have acute exacerbations of their chronic condition or suffer an acute injury, and will require treatment in an emergency department. The majority of these patients, even under this new model, likely will not require admission. For these patients, particularly those with multiple chronic conditions or behavioral health problems, physicians need tools to help coordinate outpatient care and to improve transition plans. Patients who understand their discharge instructions and are connected to outpatient services are more likely to return to their baseline. Mobile tools to integrate healthcare can both encourage medication compliance and behavior change after a visit, and can link patients back to their usual source of care.
Some acutely ill or injured patients will need highly specialized care (i.e., stroke care). When critical care capabilities are not available at the hospital closest to the patient, physician-to-physician telemedicine consultation through remote monitoring enables more patients to stay in their community. Regional care coordination exchanges, in which networks connect patients to needed resources across health systems, can assist patients who require admission as well as those who will go home. 6
The Right Side of the Wheel
Hospital-based care
In the acute care setting, patients can benefit from improved engagement of their families and caregivers. The timing of physician rounds may not be conducive to having family members physically present. “Virtual rounds,” which connect caregivers and family members with patients and their providers real time through a secure video platform, increases patient and family engagement while also increasing care coordination and communication.
Transitions of care
To improve patients’ transition home after an acute healthcare visit, communication options include videoconferencing, ideally with all providers, the patient, and their family at the time of discharge or shortly thereafter. Utilization of telemedicine solutions by transition of care coordinators prior to scheduled outpatient visits provides the opportunity to re-engage and enhances understanding and compliance with discharge recommendations.
When not a patient
Lastly, we need to empower people to take care of their own health during the time that they aren't “patients.” 7 Mobile apps and on-demand virtual consults can enhance medication compliance, behavior change, and health and wellness.
Conclusion
Ultimately, whether the ACA remains the law, regardless of CMS policies, regardless of whether ACOs are mandated, in order to improve the health of Americans, the focus cannot be on technology, payment, or the provider. It must be on the patient. We need to allow patients to get the care they want, when they want it, in the manner they want it. Technology cannot replace empathy, human interaction, or thoughtful care coordination, but the proposed model incorporates innovative solutions into a traditional framework, while acknowledging patients’ and families’ individual preferences and needs, so that we don't leave any patients behind.
Footnotes
Author Disclosure Statement
No financial conflicts of interest exist.