
Abstract
Roy, Steven, Inigo Soteras, Alison Sheets, Richard Price, Kazue Oshiro, Simon Rauch, Don McPhalen, Maria Antonia Nerin, Giacomo Strapazzon, Myron Allen, Alistair Read, and Peter Paal. Guidelines for mountain rescue during the COVID-19 pandemic: official guidelines of the International Commission for Alpine Rescue. High Alt Med Biol. 22: 128–141, 2021.
Background:
In mountain rescue, uncertainty exists on the best practice to prevent coronavirus disease 2019 (COVID-19) transmission. The aim of this work was to provide a state-of-the-art overview of the challenges caused by the COVID-19 pandemic in mountain rescue.
Methods:
Original articles or reviews, published until December 27, 2020 in Cochrane COVID-19 Study Register, EMBASE, PubMed, and Google Scholar were included. Articles were limited to English, French, German, or Spanish with the article topic COVID-19 or other epidemics, addressing transmission, transport, rescue, or cardiopulmonary resuscitation.
Results:
The literature search yielded 6,190 articles. A total of 952 were duplicates and 5,238 were unique results. After exclusion of duplicates and studies that were not relevant to this work, 249 articles were considered for this work. Finally, 72 articles and other sources were included.
Conclusions:
Recommendations are provided for protection of the rescuer (including screening, personal protective equipment [PPE], and vaccination), protection of the patient (including general masking if low risk, specific PPE if high risk), equipment hygiene (including disinfection after every mission), use of single-use products, training and medical measures under COVID-19 precautions, and psychological wellbeing of rescuers during the COVID-19 pandemic. Adapted COVID-19 precautions for low-and-medium-income countries are also discussed.
Introduction
Outdoor sports and mountain rescue have been severely affected by the coronavirus disease 2019 (COVID-19) pandemic. Early in 2020, first in East Asia and soon thereafter in Europe and America, countries introduced lockdowns to suppress the steep rise in infections. By mid-March 2020 in Europe and the United States, most ski resorts were closed. Dwindling mountain recreationalists resulted in fewer accidents. By June 2020, numbers of visitors in mountain areas bounced back and surged even above previous years. Consequently, mountain accidents have increased to record levels (BBC, 2020; BCSARA, 2020; Gawel, 2020; Hu, 2020; Scottish Mountain Rescue, 2020). In the northern hemisphere, the winter season has been severely affected by the pandemic, several skiing areas were shut down (e.g., Germany and Italy) or experienced a massive drop in visitors because of travel restrictions (e.g. Austria and Switzerland). It remains to be seen how the incidence of mountain accidents develops in the coming seasons.
In mountain rescue, uncertainty exists regarding best practice to prevent COVID-19 transmission. Regionally developed guidelines are mixed consensus and evidence-based owing to the limited data available for the mountain-specific context. The aim of this review was to provide a state-of-the-art overview on the challenges caused by the COVID-19 pandemic in mountain rescue. Guidelines are provided and graded according to evidence. In the following, suspected or confirmed COVID-19 patients will be named COVID-19 patients.
Methods
A group of members of the air, medical, and terrestrial commissions of the International Commission for Alpine Rescue (ICAR) was summoned by a call of interest. Rescuers from ICAR member organizations were surveyed to determine areas where rescuer guidance would be particularly valuable. Subsequently, pertinent COVID-19 literature was identified and selected through a scoping literature review in accordance with Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines (Tricco et al., 2018). This method was chosen as it was felt to be most appropriate for identifying and mapping the available evidence on this quickly evolving topic.
Two authors (S.R., P.P.) searched the literature with Cochrane COVID-19 Study Register, EMBASE, PubMed, and Google Scholar, using the following terms alone and in combination: “COVID-19,” “emergency medical services,” “mountain rescue,” “out-of-hospital,” “SARS-CoV-2.” The composite search string used was “emergency medical services” OR “out-of-hospital” OR “pre-hospital” OR “rescue” OR “transport” for the Cochrane Register, ((“COVID-19”) OR (“SARS-CoV-2”) OR (“pandemic”)) AND ((“emergency medical services”) OR (“out-of-hospital”) OR (“pre-hospital”) OR (“mountain rescue”) OR (“transport”)) for EMBASE and PubMed and ((“COVID-19”) OR (“SARS-CoV-2”) OR (“pandemic”)) AND (“mountain rescue”) for Google Scholar. The literature review was updated to include all publications until December 27, 2020. The bibliographies of included articles were hand-searched for additional articles that had not been identified through the literature search. Finally, a personal search among authors and a web search were performed to identify regional or national mountain rescue guidelines for the COVID-19 pandemic.
Abstracts were imported into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). Abstracts were independently screened by two authors to identify articles that met the following inclusion criteria: (1) original article or review; (2) published in English, French, German, or Spanish; (3) article topic was COVID-19 (any setting), pandemics (any setting), or other infectious outbreaks (mountain setting); and (4) addressed aspects of transmission, transport, training, rescue, or cardiopulmonary resuscitation (CPR). Abstracts that met the initial screening criteria underwent subsequent full-text review and those that did not meet the screening criteria were excluded. Full-text review was then conducted to determine which articles were relevant. These articles were provided to the guidelines panel for consideration. The panel used a consensus approach to develop recommendations and graded each recommendation according to criteria stipulated by the Grading of Recommendations Assessment, Development and Evaluation guidelines (Table 1) (Guyatt et al., 2006). In the discussion we present the evidence informing our recommendations, supplemented by expert opinion and experience. Afterward the recommendations to the pertinent section are given in separate tables.
Classification Scheme for Grading Evidence
Results
The literature search yielded 6,190 articles. A total 952 were duplicates and 5,238 were unique results. In the initial abstract screening, 273 studies met the inclusion criteria for full-text review and 4,965 articles did not meet the inclusion criteria and were excluded. Full-text review revealed 6 duplicates that were not identified automatically by our systematic review software, leaving 267 original articles to review. On full-text review, 18 articles did not meet the inclusion criteria and were excluded. The remaining 249 articles were included for consideration. A total of 72 articles and other sources were referenced in the final manuscript. Selected results of the rescuer survey are included in the Supplementary Appendix S1.
Discussion and Recommendations
Specific challenges in mountain rescue related to the COVID-19 pandemic
Since the early stages of the pandemic, during the warm months rescue call volumes have increased substantially, straining resources for small rescue teams and creating constraints around training and staffing. In mountain compared with urban rescue, staff and equipment are limited, more so in terrestrial than in airborne missions. During terrestrial rescue, substantial physical efforts may be necessary. Often, mountain rescue has to be provided in an austere environment with limited material and staff in close proximity between victims and rescuers. The risk of contracting COVID-19 outdoors is thought to be low when acting prudently (Qian et al., 2021), but care should still be taken when in close contact with patients and other rescuers. During technical rescue activities, some forms of personal protective equipment (PPE) may introduce unacceptable communications or visibility risks or limit exertion and performance. Wet weather and sweating may decrease protection of PPE and threaten the safety of mountain rescuers from fogging of eye protection. Specific recommendations are given in Table 2.
Challenges in Mountain Rescue Related to the Coronavirus Disease 2019 Pandemic
COVID-19, coronavirus disease 2019.
Rescuer safety and infection prevention
The severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) is mainly transmitted through respiratory droplet. The evolving science on COVID-19 transmission is discussed in detail elsewhere (Berlin et al., 2020; Gandhi et al., 2020; Wiersinga et al., 2020). Specific recommendations for rescuer safety and infection prevention are given in Table 3.
Rescuer Safety and Infection Prevention
PPE, personal protective equipment.
General principles
Search and Rescue (SAR) is an essential function provided to recreationalists, workers, and travelers throughout the world in mountain and wilderness areas. SAR teams need to maintain training and fitness to be ready for these demanding activities and local COVID-19 infection rates affect their ability to train and respond. Following regional and national COVID-19 prevention guidelines is important to reduce community transmission. Rescuers who are at high risk for COVID-19 complications need to consider their suitability for the job during this pandemic. Although there are ways to reduce risk of viral exposure when caring for patients, it cannot be eliminated entirely.
Preventing viral transmission during SAR activities during the pandemic is vital and challenging. Best practices for PPE evolve, but as essential workers, it is recommended that rescuers protect themselves, maintain social distance whenever possible, provide facemasks for patients and bystanders, and limit the number of rescuers exposed to any possible SARS-CoV-2 source. Separating rescue and incident management teams into working bubbles provides a degree of infection prevention (Shaw et al., 2020). This may prevent entire teams from being taken out of service for quarantine after potential exposures. Detailed logs of personnel attendance at training and missions, including outside agencies, must be maintained for possible future contact tracing.
Prevention includes maintaining social distance at trailheads and staging areas, limiting the number of rescuers in huts, tents, snow shelters, caves, crevasses, aircraft, vehicles, and gear caches (Knibbs et al., 2012). Scenes should be approached with at least 2 m of separation between individuals on trails whenever possible. The minimum airborne-precaution PPE includes gloves, long-sleeves, and pants, a N95 or FFP2 respirator or equivalent, and eye and face protection. Wearing a facemask has been shown to reduce the dispersion of respiratory secretions and, therefore, reduces risk of SARS-CoV-2 transmission. Wearing PPE of appropriate type and fit can be cumbersome when doing strenuous activity leading to fogging of eye protection, difficulty breathing, overheating, decreased exercise capacity, and problems in verbal communication.
Rescuers may lower masks on trails when social distancing can be maintained. Similarly long sleeves, pants, and eye protection can be kept off until it becomes necessary to get close to patients, teammates, or other subjects on scene. Once rescuers are within 2 m of the patient, PPE should be maintained on rescuers unless it compromises the safety of the operation. Patients must have facemasks placed as soon as possible, a higher protection level should be considered (e.g., N95/FFP2), if COVID-19 is suspected or confirmed. Rescuers should stay upwind of the patient.
If a rescuer has had a high-risk exposure or COVID-19 positive test, they should quarantine according to regional or national guidelines before returning to duties (CDC, 2020a, CDC, 2020b; WHO, 2020a). Care should be taken to avoid cross-contamination and cleaning protocols for rescuer and team equipment should include equipment cleaning at end of mission. Rescuers should carry spare PPE and a biohazard disposal bag. During rescue and when donning and doffing PPE the buddy check system should be endorsed. The waste produced during the rescue has to be managed and disposed of properly.
Specific principles
Masks
Masks are highly effective in reducing SARS-CoV-2 transmission and are advised (Chu et al., 2020; Leung et al., 2020; Liang et al., 2020). In particular, surgical and medical grade masks demonstrate superior performance in the clinical environment and are preferred over cloth masks, bandanas, or commercially available neck gaiters. Nonsurgical masks should have at least two layers of fabric (CDC, 2020c), although some authorities suggest three layers (WHO, 2020b) if medical grade masks are unavailable. A proper fit over the nose, mouth, and chin are necessary for any type of mask. When aerosol-generating procedures (AGP) such as suction, high flow oxygen, intubation, or chest compressions are needed, rescuers attending to a patient should use at least a N95/FFP2 respirator to prevent viral spread. Simple surgical masks are reported to be both inferior in risk reduction (MacIntyre et al., 2013; Chou et al., 2020; Chu et al., 2020; Wang et al., 2020) and equivalent (Radonovich et al., 2019; Bartoszko et al., 2020; Long et al., 2020) when compared with N95/FFP2 respirators. Medical masks and respirators are critical supplies that should continue to be reserved for health care workers and other medical first responders depending on local supply. Masks with expiratory valves are not recommended, as they do not prevent aerosolized particles from spreading. Small children, patients with trouble breathing, unconscious, or incapacitated patients may require careful consideration around mask utilization to reduce potential viral spread.
Masks and respirators are associated with increased respiratory rate and perceived effort (Jones, 1991), impaired cardiopulmonary exercise capacity (Chen et al., 2016; Fikenzer et al., 2020; Epstein et al., 2021), potential user discomfort (Lan et al., 2020; Mushtaq et al., 2021), and may interfere with communication (Burton et al., 2020). Some studies suggest that physically demanding tasks may be impeded by the mask (Chen et al., 2016; Fikenzer et al., 2020). Others suggest that while perceived respiratory effort may be increased, vigorous exercise and CPR quality are not affected by masking (Hopkins et al., 2020; Kienbacher et al., 2021). Mask performance may be reduced by moisture from sweating or heavy breathing. Medical masks are designed for a relatively dry, indoor, controlled environment and replacements could be necessary for some environments. Medical masks lose their physical integrity or their ability to effectively prevent transmission of microbes when wet (Andersen, 2019).
Eye protection
Eye protection when performing SAR activities is generally appropriate to prevent injury, snow blindness, and so on. Eye protection, especially “wrap around” or goggle type eyewear may confer additional benefit to the mask (Lindsley et al., 2020) in reducing the risk of viral transmission (Chu et al., 2020; WHO, 2020c). Face shields are an option and may be part of helmet assembly facilitating ease of use.
Gloves
Medical grade, waterproof gloves should be used when providing patient care. Availability of gloves is generally good, and cost is low. Some gloves used by rescuers for rope work and warmth do not provide the same level of protection but may be placed over medical gloves or may replace medical gloves once patient care is complete.
Clothing/body covering
Because medical gowns are not practical in alpine rescue, clothing that covers the full upper and lower torso and limbs may be used to avoid contact transmission. Watertight long-sleeved garment and trousers are suitable. One-piece suits (e.g., Tyvek® 800J) may also be worn; however, rescuers should be mindful of their condition during hot or strenuous activities as overheating may occur. Gowns can be used during airway management to protect providers' skin and clothing from contamination. Be aware of variable permeability of gowns depending on rating. Clothing should be doffed and stored in a reusable or disposable bag at the end of a mission. A change of clothes and doffing bags for contaminated outerwear should be available at the end of a mission to prevent vehicle contamination.
Equipment cleaning and return to service
Once used, equipment with risk of contamination should be decontaminated before return to service. Treatment with soap and warm water or isopropyl alcohol are effective in removing detectable virus from equipment (Chin et al., 2020; Pradhan et al., 2020) and may be used when they will not damage equipment. Ropes, cord, webbing, and other life-safety soft goods should be cleaned according to manufacturers' recommendations. Smooth hard surfaces appear to harbor detectable viral material longer than textiles, but are also more easily cleaned (Chin et al., 2020; van Doremalen et al., 2020). For equipment that cannot be cleaned for logistical or safety reasons, quarantine of the equipment has been proposed (Black Diamond Equipment, 2020; DMM Wales, 2020; Greatbatch et al., 2020; Kong Italy, 2020; Maxim Ropes, 2020; Petzl America, 2020; Singing Rock, 2020). Recommendations for quarantine of equipment vary from 3 to 7 days (BEAL, 2020; Black Diamond Equipment, 2020; DMM Wales, 2020; Kong Italy, 2020; Mammut, 2020; Petzl America, 2020; Singing Rock, 2020). Quarantine of equipment results in equipment being inaccessible for rescue, and therefore may be impractical (Greatbatch et al., 2020).
Vaccination
Vaccinations are now available against the most common strain of COVID-19 (Sahin et al., 2020; Baden et al., 2021), although individual strain prevalence is changing. Vaccinations should be offered according to vaccine manufacturers guidelines and national guidelines as early as possible to all rescuers involved in patient care. Local and regional protocols may determine availability.
Psychological support
The global pandemic has caused considerable stress to many rescuers and nonrescuers alike. Acute stress injury may exacerbate preexisting anxiety, depression, and other psychological illnesses and result in more serious stress disorders (Miguel-Puga et al., 2021). Education and increased awareness of stress injuries could be valuable to build resilience and prevent adverse psychological consequences in mountain rescuers (Krystal, 2020).
Terrestrial and airborne rescue
Specific recommendations are given in Table 4.
Treatment and Rescue Recommendations
AED, automatic emergency defibrillator; AGP, aerosol-generating procedure; CPR, cardiopulmonary resuscitation; VF/pVT, ventricular fibrillation or pulseless ventricular tachycardia.
Patient treatment
During the COVID-19 pandemic it must be assumed that any patient is potentially infected with SARS-CoV-2. Asymptomatic individuals can transmit the virus. Therefore, precautionary measures have to be adopted to reduce risk of infection. Some have suggested that during ground rescue operation, screening of any conscious patient with a COVID-19 questionnaire should be performed (Massullo et al., 2021). Known or likely COVID-19-positive patients should be treated with extra caution. The consensus of our group is that every patient is considered as potentially COVID-19 positive. Because the SARS-CoV-2 infection rates vary worldwide, the recommendation regarding PPE while treating patients without confirmed or likely COVID-19 should be adjusted according to local protocols and regional risk assessment (Chu et al., 2020).
During difficult technical operations (e.g., rope maneuvers, hoisting, canyoning rescue), it may be challenging to keep PPE in place. Rescue organizations should choose PPE compatible with the use of technical equipment such as helmets and harnesses. Their use might be limited during complex technical rescues and in harsh environments where mountain rescuers are exposed to factors like water, wind, rain, and snow. Rescuer exercise capacity and comfort may be impaired by disposable medical respirators during exercise and can increase CO2 rebreathing (Chen et al., 2016; Fikenzer et al., 2020; Epstein et al., 2021; Mushtaq et al., 2021). Optimal face coverings depend on the patient, terrain, and specific rescue characteristics. PPE should be selected to balance performance limitation and impaired communication with the benefit of reducing potential viral exposure. An approach to selecting appropriate face coverings is given in Figure 1.
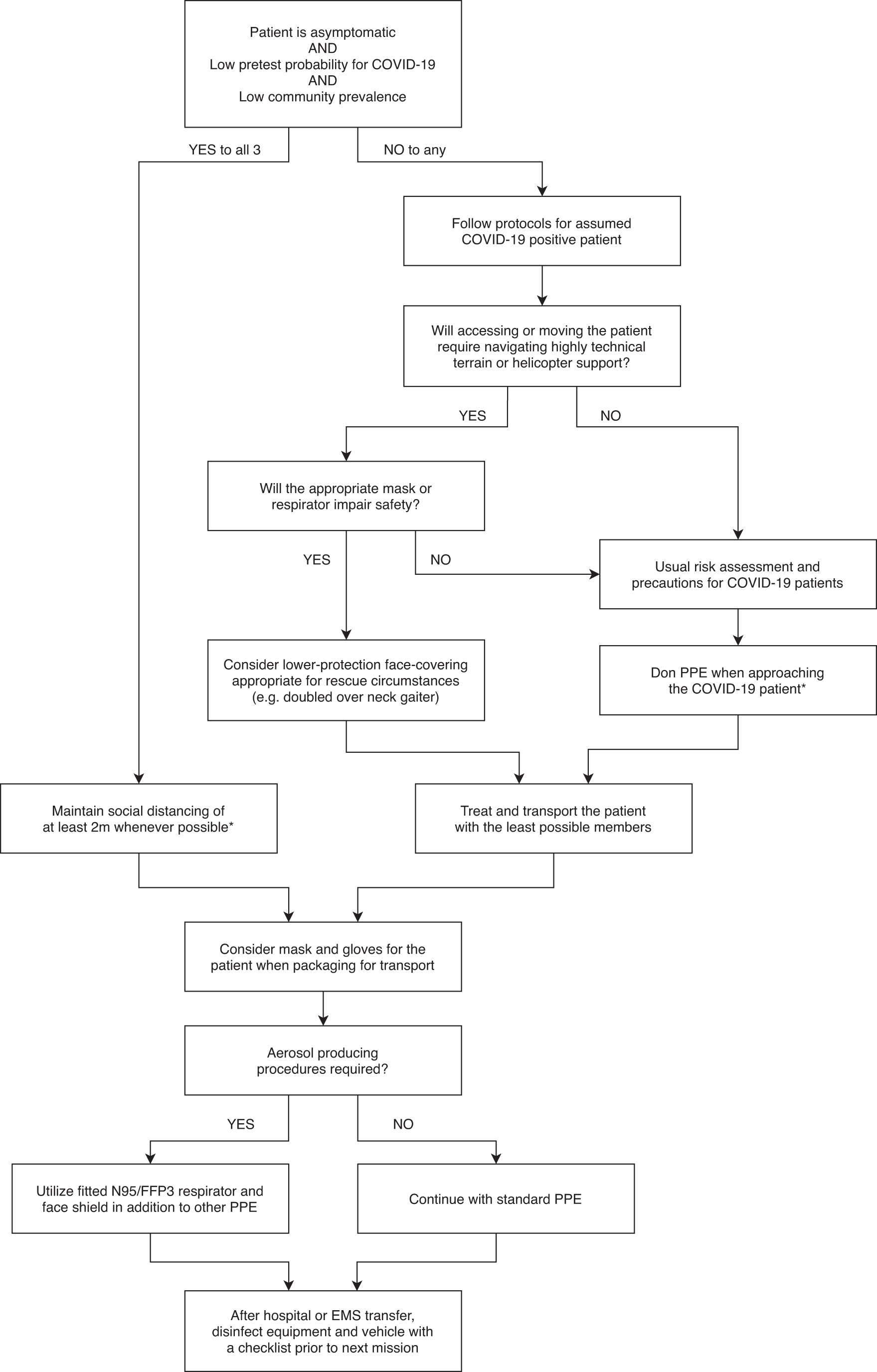
Treatment algorithm in mountain rescue for an ill or injured patient during the COVID-19 pandemic. *In accordance with any local and national guidelines. COVID-19, coronavirus disease 2019.
Airway management
Airway management is an AGP, it should be avoided whenever possible. Full PPE should be used if airway management is required. Specific guidelines have been published on airway management. In a hypoxic patient with sufficient respiratory effort, a nasal cannula may be used with an N95/FFP2 mask on top. Only a negligible difference in FiO2 was found when an oxygen mask was placed over a surgical mask (Binks et al., 2020).
Basic life support and advanced life support
CPR is an AGP. CPR has to include COVID-19 precautions. The International Liaison on Committee on Resuscitation (ILCOR) and the European Resuscitation Council (ERC) published COVID-19 guidelines for basic life support and advanced life support (Nolan et al., 2020; Perkins et al., 2020).
Other medical maneuvers
Insulation
A casualty should be protected against further heat loss with a whole-body insulation covered by a vapor barrier outer shell (Paal et al., 2016). Placement of insulation requires being in close proximity with the casualty, but it is not considered an AGP.
Management of fractures and dislocations
Splinting and immobilization are common on-site medical interventions in mountain rescue operations (Ellerton et al., 2009). Splinting requires close contact with the casualty, but this is not an AGP.
Fluids and drugs
Intravenous access remains the cornerstone of drug administration in emergencies. Establishing intravenous access may be particularly difficult or impossible during mountain rescue operations in casualties with a collapsed vascular bed (e.g., in cardiac arrest or hypovolemic shock). A recent review compared the use of intravenous and intraosseous access in providers wearing high-precaution PPE, and suggested that in this context intraosseous access is achieved faster (Drozd et al., 2021). Intraoesseous access may have limitations during prolonged rescues or in aqueous environments (Strapazzon et al., 2018). Additional routes of drug administration have been suggested in mountain rescue. Intranasal, transmucosal, and oral are minimally invasive and are generally good choices for rescue in harsh environments. However, in casualties with suspected or confirmed COVID-19, intramuscular and subcutaneous administration may be preferable routes of administration compared with oral and transmucosal routes as they avoid potential exposure to mucous membranes.
Handling bodies of deceased persons with COVID-19
It is thought that transmission of SARS-CoV-2 is possible through contact with contaminated surfaces or direct contact with human remains or bodily fluids where the virus is present (Yaacoub et al., 2020). At present, there is no evidence of transmission of SARS-CoV-2 through the routine handling of bodies of deceased persons, and the potential risk of COVID-19 transmission in this setting is considered low (Yaacoub et al., 2020). Bodies should be packaged for transport in a manner that minimizes the risk of spray of bodily fluids. Postmortem examinations should be undertaken with PPE appropriate to the type of examination being undertaken (Table 5).
Handling of a Deceased Person
Transportation
Specific recommendations are given in Table 6. The integration of mountain rescue, emergency medical services (EMS), and hospital services is crucial to ensure appropriate management and safe transport of suspected or confirmed COVID-19 patients (Bredmose et al., 2020). Responsibilities may differ, good communication is key; COVID-19 patients have to be identified in a timely manner. Mountain rescue teams should be prepared to safely transport COVID-19 patients. The transport of COVID-19 patients should be conducted by experienced teams utilizing appropriate equipment (Bredmose et al., 2020).
Transportation Challenges
Some organizations may consider the use of “isolation pods” with appropriate air filtration where cabin separation is not possible. Minimize members involved in patient transport and care (Albertch et al., 2020).
Patient packaging consideration
Patients should wear PPE including surgical mask and nonsterile gloves. Consider packaging the patient for technical rescue even if the injury does not require it to reduce the risk of transmission. Packaging means wrapping the patient into a plastic sheet before placing him on the stretcher (Bredmose et al., 2020).
Vehicle decontamination after a suspected or confirmed COVID-19 case
Immediately after a patient transport, all exposed surfaces of the vehicle should be disinfected before it returns to normal operational duties. Universal sanitizing wipes or a chlorine-based solution at 1,000 parts per million (or approved equivalent) should be used. When AGP have been performed, work from top to bottom in a standardized systematic process. A checklist of areas to be cleaned can be used to improve coverage (Bredmose et al., 2020). Any exposed equipment, which was not sealed off during transport, requires disinfection. Finally, the vehicle floor requires cleaning and disinfection (CDC, 2020d).
Disinfection should be performed by the staff involved in the patient transport. Staff cleaning the vehicle should wear PPE for infection precautions (including a long-sleeved impervious gown, surgical mask, goggles, and nonsterile gloves). Therefore, it may be prudent to clean the vehicle at the receiving hospital, before doffing their PPE (especially with PPE shortages). Cleaning is specific to each vehicle type and includes wiping of all surfaces with a cleaning product followed by a disinfectant or a combined product. If the vehicle is cleaned at the garage or hangar, a PPE disposal system must be present (CDC, 2020e).
Airframes
In most medical helicopters used in mountain rescue, the cabin is a single, shared environment between pilot, medical staff, and patient. In such airframes, it is not possible to isolate the pilot from the patient compartment. The helicopter staff may not doff PPE until the cabin has been decontaminated. It is essential to consult aircraft engineers, as some cleaning products may damage the aircraft. The aircraft will require additional down time to be adequately cleaned and dried before a subsequent mission. Wiping the cabin is estimated to take an hour; additional time may be needed for fumigation and drying.
Ground vehicles
Isolation of the patient compartment from the passenger compartment and filtration of the air may be possible in ground transport vehicles (Osborn et al., 2020). Separation creates a safer environment for the rescue teams. Limit the number of providers in the patient compartment to essential personnel to minimize possible rescuers exposures. Ground vehicles will be decontaminated after transfer of care at the receiving facility. A minimum number of persons should decontaminate the inside of a vehicle to avoid incidental contamination (WHO, 2020d).
Mountain rescue training
Specific recommendations are given in Table 7.
Mountain Rescue Training Challenges
General challenges
Recommendations around rescue team training are based largely on rescue team members' comments and observations. The risk of COVID-19 exposure during mountain rescue training has generally made all training exercises slower, more difficult, and more expensive. Teams need to review and prioritize training activities over time to focus on essential training activities only for the time being. Alternative training methods can be used such as virtual first aid training and some training activities can be carried out with minimal group sizes or within training group bubbles. Records of training attendance should be retained to facilitate contact tracing in case a team member becomes symptomatic.
COVID-19 precautions including PPE use during training may introduce additional risks as discussed in previous sections. Team leaders should manage these risks in the context of other important training hazards.
Distancing during active mountain rescue training exercises can be challenging. Careful attention to precautions during travel and training should be practiced and evaluated as a normal part of training exercises. Training equipment should be handled, decontaminated, and/or quarantined according to team protocols. Teams may wish to modify rescue techniques in some situations (e.g., coaching a subject and their partners to self-package) and any modified procedures should be part of training exercises. Teams should receive regular medical direction regarding the use of COVID-19 testing within the group and vaccination to help guide training activities.
Specific training challenges
In the context of mountain rescue, AGP may be modified with appropriate medical direction. Modified procedures should be practiced during training using safe alternative training devices such as airway mannequins. First aid training can be enhanced to regularly practice PPE donning and doffing procedures with rescue clothing and gear, PPE use in the mountain environment, and to provide updated COVID-19-related medical information. Water and canyoning rescue may have to be substantially modified during the pandemic owing to the inherent problems of using PPE and training in wet environments where close contact and coughing are common and may be unexpected.
Challenges in low-and-middle-income countries
Specific recommendations are given in Table 8. There is growing concern about the impact of the pandemic on low- and middle-income countries (LMICs). Of the 107 LMICs assigned a COVID-19 preparedness capacity level by the WHO, almost all (94) are at Level 3 (capacity is ≤60%) or below, with more than half (57) designated as Level 3, a third (36) as Level 2 (capacity ≤40%), and one as Level 1 (capacity ≤20%) (Kates et al., 2020). The WHO COVID-19 Strategic Preparedness and Response Plan acknowledges that rural and remote populations are vulnerable populations that deserve preparedness planning (WHO, 2021). Predicting the development of the outbreak and fighting the virus in the countryside is an ongoing challenge. In LMICs, most rescue operations are carried out by first responders or villagers from impoverished areas, before professional rescue arrives. The quality of provided medical support depends upon the available resources, including knowledge of COVID-19 prevention measures, PPE, EMS, testing kits, disinfectants and wastage treating, clean water. It has been stated that, “medical care in the wilderness is the art of the possible” (Zafren et al., 2012). This is true even more so when care has to be provided in an LMIC.
Challenges in Low- and Middle-Income Countries
PPE for low resource countries
Rescue teams must adapt PPE according to the situation and implement means of circumstances (or fortune) to cover COVID-19 prevention measures. When rapid diagnostic testing is not possible, health care providers should consider recommending that the individual isolate for possible COVID-19 based on the current guidance and level of suspicion. Health care providers and rescuers should consider having patients wear a mask or cloth face covering and glasses for source control to prevent the spread of COVID-19. Being ill with an infectious disease, for example, malaria, dengue, or tuberculosis does not exclude coinfection with COVID-19. To cope with increased staffing demand during this pandemic, active recruitment and training of health care personnel should be carried out concurrently. For specific recommendations, see Table 7.
Masks with at least two layers of washable and breathable fabric reduce the spread of SARS-CoV-2 (CDC, 2020c). When resources are limited, WHO guidelines recommend three layers of cloth for protection (WHO, 2020b). Novel strategies, such as plexiglass shields, may be considered to minimize health care worker exposure and preserve PPE during transport as well as plastic or fabric aprons. Many of the disinfectants will not be available in the least developed countries. Bleach or alcohol after washing with soap and water are an alternative; however, most rescue equipment and mountain clothes may not be disinfected with bleach. Equipment that cannot be cleaned for logistical or safety reasons, may be quarantined when feasible (see Equipment Cleaning and Return to Service section).
During prolonged rescue and in case of extended or overnight rest, all individuals must respect as much as possible the hygiene, distancing, and barrier measures to avoid COVID-19 owing to the increase of time exposure, close situation, and closed place.
Nutrition during prolonged rescue
In 2001 the WHO introduced the Five Keys to Safer Food (World Health Organization, Department of Food Safety, Zoonoses and Foodborne Diseases, 2006). It is highly unlikely that people can contract COVID-19 from food or food packaging (WHO, 2020e). Good hygienic practices include the following: (1) mask, (2) hand hygiene, washing with soap and water for at least 20 seconds or frequent use of alcohol-based hand sanitizers; (3) respiratory hygiene (cover mouth and nose when coughing or sneezing; dispose of tissues and wash hands); (4) restricting nonessential physical contact; (5) cleaning and disinfection procedures for equipment, contact surfaces at least with soap; and (6) that patients should use their own utensils to drink and eat. In case of low disponibility, utensils are disinfected before being used by another person.
In LMICs, medical and rescue teams work with little equipment and often have to improvise. All solutions have to be assessed for feasibility, cost, and appropriateness. All planning, implemented steps, procedures should be documented safely for future endeavors. Every plan can fail thus a plan B should be ready as backup. LMICs need immediate support from the international community as they often lack the productive capacity and financial resources to obtain necessary health equipment.
Knowledge gaps
The contagiosity of asymptomatic carriers has been documented but has not been quantified. The specific risk for transmission in air and on surfaces continues to be delineated. Infection prophylaxis after exposure, immunity after a previous COVID-19 infection and vaccination, vaccination modalities, treatment, and the hazard posed by SARS-CoV-2 mutations require further research.
Outlook
Since the 1918/19 influenza pandemic, COVID-19 is the disease, which has claimed most victims in a given period. Unprecedently quick improvements in medical care have been achieved since COVID-19 appeared in late 2019. A return to a pre-COVID-19 life seems only possible with vaccinations. Experts have warned since several years of pandemics. It was not the question if/but when a pandemic would strike humankind. More than 20 pathogens are known to have a pandemic potential. Dense population, environmental change, globalization and habitat loss make the spread of further pathogens with pandemic potential more likely. The COVID-19 pandemic can teach the world several lessons, which should be learned and implemented before the next pandemic strikes humankind.
Limitations
Several parts in this work are based on expert opinion and experience rather than pure science. Despite a low level of evidence, recommendations were graded as strong if they were considered important for safety reasons. This approach is consistent with other guidelines (Guyatt et al., 2006). Required social distancing and requirements for masks vary between areas. Knowledge of SARS-CoV-2 and COVID-19 is developing rapidly. The content of this article has to be seen within this rapidly changing science. Updates of this content are required as soon as major scientific breakthroughs are made.
Conclusions
This article covers several important topics pertaining to mountain rescue and provides recommendation for mitigating key risks. Evidence-graded recommendations are provided for rescuer safety and infection prevention, protection of the patient, equipment disinfection and selection, training, and medical measures under COVID-19 precautions, and psychological wellbeing of rescuers during the COVID-19 pandemic. Adapted COVID-19 precautions for specific challenges in low-and-medium-income countries are also discussed. Finally, knowledge gaps are identified and an outlook is given.
Footnotes
Acknowledgment
The authors thank ICAR MedCom for critical discussion of this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The publication as an open-access article was facilitated by the International Society for Mountain Medicine (ISMM) Open Science Grant as well as funding from ICAR MedCom.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.