
Abstract
Abstract
Harness hang syncope (HHS) is a risk that specifically affects safety of harness users in mountain climbing.
Aims:
To evaluate individual patterns of breathing resulting from deranged cardiovascular reflexes triggering a syncopal event when a mismatch between cerebral O2 demand and supply is present.
Results:
Forty healthy participants [aged 39.1 (8.2) years] were enrolled in a motionless suspension test while hanging in harness. Respiratory gas exchange values were analyzed to assess the pattern of breathing (EpInWel, respiratory elastic power) and cardiovascular parameters were monitored (BP, blood pressure). Four participants experienced HHS after 30.0 (7.6) minutes, with an early manifestation of loss of control of both a sustainable EpInWel and BP, starting after 10–12 minutes. Among the other participants, two different reactions were observed during suspension: (1) group G1 tolerated 32.7 (11.4) minutes of suspension by a favorable adaptation of the EpInWel and BP parameters and (2) group G2 showed significantly shorter time of suspension 24.0 (10.4) minutes with unfavorable increase in EpInWel and BP.
Conclusions:
Greater resistance to HHS occurs in people developing less marked fluctuations of both respiratory and cardiovascular reflex responses. Conversely, wider fluctuations both in control of EpInWel and BP were observed in the event of decreased suspension tolerance or in syncopal events.
Introduction
Awide knowledge gap exists regarding the risks of hanging motionless in harness, even among experienced users. The most distinctive effect is commonly known as suspension trauma, or more properly referred to as harness hang syncope (HHS). If prompt adjustment of posture/condition is not performed, a lethal multivisceral hypoxia arises even in the absence of a specific trauma leading to HHS (Seddon, 2002; Van Lieshout et al., 2003). Our recent study on the pathophysiology of HHS suggests that the condition that may jeopardize cerebral hypo-oxygenation develops within a few minutes after suspension (Lanfranconi et al., 2017b).
The most evident effect reported in this study is the existence of a critical amount of cerebral deoxygenation, as ascertained by a brain near-infrared spectroscopy investigation: cerebral deoxygenation eventually inhibits the cardiovascular reflexes while abruptly triggering syncopal event. Death due to syncope while hanging in harness could be the unwanted, predictable consequence of a delayed rescue in HHS.
The multifaceted HHS phenomenon and its consequences are not well known by veteran climbers. Awareness about HHS is limited, and the theoretical analysis of its effects is discussed only in a few scientific articles. The consequence is an underestimated risk of life-threatening events even among experienced members of the mountaineering community (Lee and Porter, 2007; Turner et al., 2008; Mortimer, 2011; Pasquier et al., 2011; Hsiao et al., 2012). The number of high mountain casualties is increasing in Alpine regions, and HHS could potentially affect more and more harness users. Indeed, the Alpine peaks are easily accessible by téléphériques (aerial tramway) that can take climbers up to the first 3000 m or so, and as a result in Mont Blanc region alone 20,000-plus people attempt to reach the summit yearly (Fig. 1).
Red arrow: people looking at the Mont Blanc du Tacul from Aiguille du Midi, 3842 m above sea level. In the small square, the last section of the téléphérique from Chamonix (France) (photography by Ugo De Berti).
Inexperienced climbers, relying on the skills of Alpine guides to get up and down the mountain safely, are quite substantial in this impressive number of summit hikers (Wallace, 2012). This circumstance seems far more significant than it is even thought because there is only a remote chance that knowledge about high-altitude health risks, including the HHS occurrence, and countermeasure skills could be part of the cultural heritage of the thousands of climbing apprentices. At least, improving the knowledge of experienced climbers by enlightening them about measures to counteract HHS will help reduce the risk and pave the way toward a sensible and balanced approach to high mountain climbing.
Examining metabolic impairments along the human O2 transport utilization chain by inducing syncope, while wearing harness, could provide important insights into the multivisceral hypoxia that distinguishes HHS itself. Included in the definition of syncope are the strong relationship between gravitational stress, vasomotor failure and/or bradycardia, reduced venous return, and fallen cardiac output with a definitive decrease in cerebral oxygenation before fainting (Moya et al., 2009). Microgravity effects on cardiovascular reflexes are new findings incorporated to the understanding of the HHS pathophysiology in our previous work (Lanfranconi et al., 2017b). The next phase, in this step-by-step approach to the intriguing complexity of HHS events, concerns the involvement of the respiratory system control in triggering a syncopal event when an incompatibility between cerebral O2 demand and supply is present (Convertino et al., 1994, 2009; Serrador et al., 2000, 2006).
Certainly, while hanging in harness, two main conditions can interfere with the individual pattern of breathing: (1) thoracic constraint due to mechanical limitation of either the rib cage or the abdominal wall and (2) cerebral hypoxia impacting the respiratory control centers in the brain. This article is a further analysis of data originating from the same participants of our already mentioned experimental set (Lanfranconi et al., 2017b). It aimed on the capacity of the human body to cope with the effects of motionless suspension from the respiratory control's perspective. Our investigation is intended to verify if the pattern of breathing varied among participants hanging in harness. Additionally, the individual strategy to cope with cerebral hypoxia was explored to evaluate possible factors of resilience to make O2 available to the cerebral cortex.
Methods
Participants
The study conformed to the standards set by the latest revision of the Declaration of Helsinki, and all procedures were approved by the ethics committee of the University of Milano-Bicocca (approval number: 4566/2010). Personal data were treated according to standard principles of confidentiality. Participants were informed about the risks of developing HHS and the ability of the medical team to manage possible emergency. All participants signed an informed consent to be part of the project.
Forty adults participated in this study with a mean (SD) age of 39.1 (8.2) years, body mass index of 24.2 (3.03), and 85% were males and 15% females. Six additional young, healthy, and sedentary participants (gender matched, body mass indexes within the normal range) participated in an extra spirometric evaluation to estimate the impact of different mechanical loads on the respiratory system (LOAD group). See the Respiratory Evaluation section for further information. Smokers were not included in this research program.
Suspension protocol
An extended version of the suspension test (ST) protocol has already been described in our previous article (Lanfranconi et al., 2017b). Pulmonary ventilation (
Participants who developed syncope were kept in a supine position by passively raising both their legs above cardiac level (Bridges and Jarquin-Valdivia, 2005; Kweon et al, 2012). No time limit was previously set. In the case of syncope, the end time of the ST was when the unconscious participant laid down on the examination table.
Respiratory evaluation
Pulmonary function tests
Each participant was asked to perform a spirometry test, sitting and in resting condition (Vmax Spectra 229; SensorMedics, Yorba Linda, CA). The variables measured were as follows: the volume from a maximal forced expiratory effort (FVC, the forced vital capacity), the forced expiratory volume in the first second (FEV1), the forced expiratory flux at 25%–75% (FEF25–75), and the peak expiratory flow rate. A visual evaluation of the expected spirometry curves was performed, and the average of three consecutive and repeatable measures was used. All variables were expressed with respect to predicted values according to age, sex, and anthropometric values.
On another day, the LOAD group performed extra spirometry measures to estimate the impact of different mechanical loads on the respiratory system: (1) in resting and sitting orthostatism; (2) in clinostatism, lying on the examination table; (3) while hanging in the harness; and (4) while sitting and applying a pneumatic tourniquet cuff (15 cm height, 120 cm length) around the upper abdomen/lower chest, inflated at progressively increased pressure (25–50–75 mmHg).
Respiratory power
A simple approach to estimate the inspiratory elastic power was recently proposed and proved useful to compare the energy expenditure when changing the pattern of breathing due to respiratory diseases or environmental conditions (Dellweg et al., 2008; Passoni et al., 2015; Beretta et al., 2017). Considering the linearity of the overall volume–pressure relationship of the respiratory system, between the resting respiratory capacities up to the end-inspiration, the elastic/resistive work performed by the inspiratory muscles (InWel) can be defined as the area of the right triangle where one leg (cathetus) is the change in lung volume or tidal volume (V
(1) InWel = ½(V
Being the hypotenuse, the total respiratory compliance or Cres = V
(2) InWel = ½(Cres)−1*Vt2
and knowing the respiratory rate (Rf), the InWel per minute becomes the inspiratory elastic power (Ep):
(3) EpInWel = ½(Cres)−1*V
Arbitrarily assuming the factor Cres unchanged during suspension, the product ½V
Study design and statistical analyses
This was a single-center, analytic observational study, with cross-sectional design. Values are expressed as mean (SD). Sample size calculation determined that a sample of 34 subjects would be adequate to detect a difference of 8 minutes in suspension time between the participants, with a power of 0.80 (α = 0.05). D'Agostino and Pearson omnibus normality test was used to check if the values come from a Gaussian distribution: all the variables passed the normality test. The statistical significance of the difference between mean values, considering the different circumstances, was evaluated by: (1) ordinary one-way ANOVA, followed by Tukey's multiple comparison test, with a single pooled variance and (2) unpaired t test, two-tailed. Regression analyses were performed using the least squared residuals method. The level of significance was set at p < 0.05.
All statistical analyses were performed using a commercially available software package (Prism 6.0; GraphPad, La Jolla, CA).
Results
Pattern of breathing during the ST
Four participants experienced syncopal event after 30.0 (7.6) minutes (SYN). Within SYN, one person was a regular user of harness.
A posteriori, the other participants were divided into two groups, based on the time course of
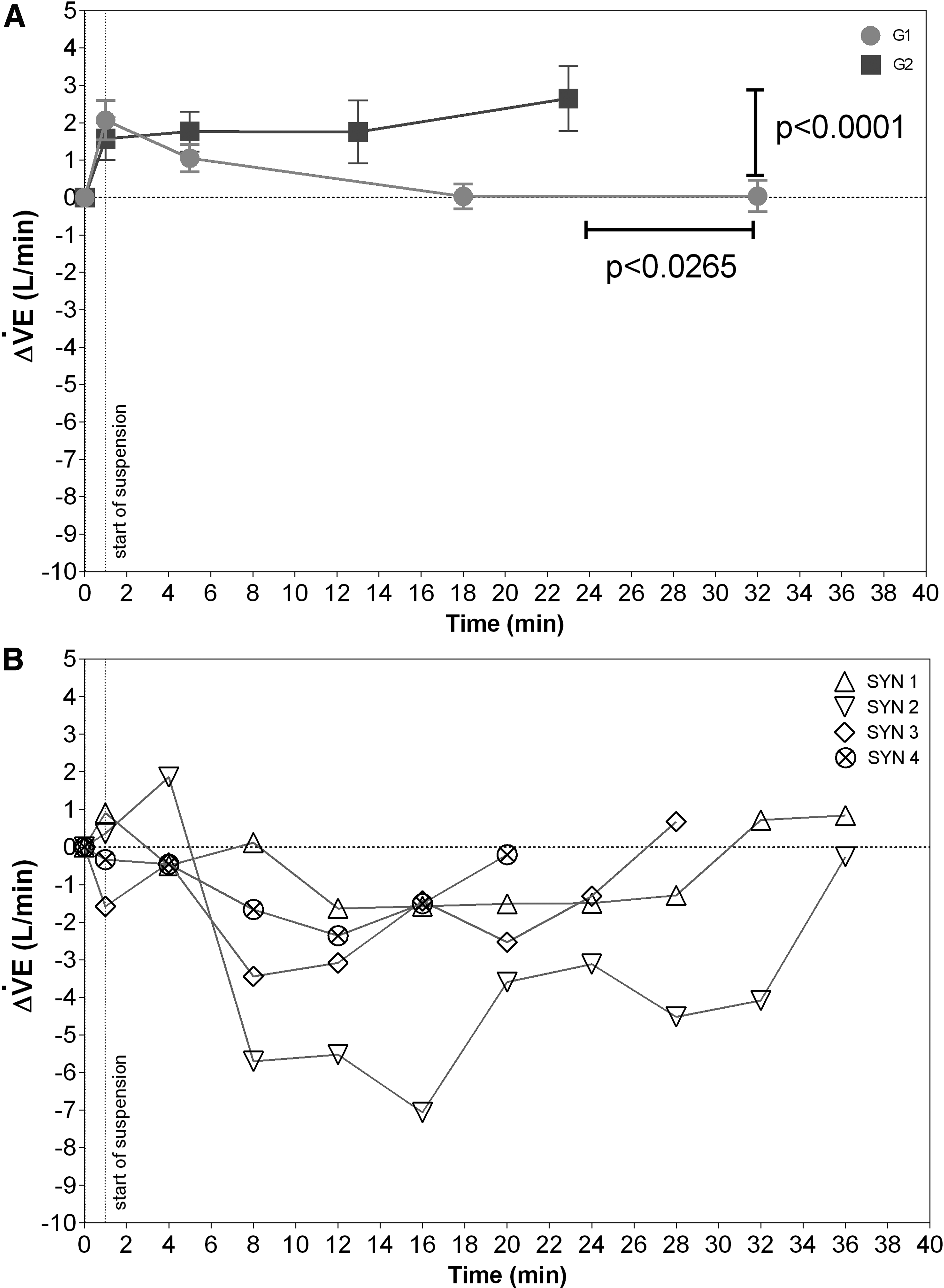
Time courses of changes in ventilation (
Suspension time was significantly shorter in G2 [24.0 (10.4) minutes] compared with G1 [32.7 (11.4) minutes]. At the end of the ST,
An initial variable response of
Figure 3 presents the changes in the pattern of breathing among the groups, during the ST, as described by the plot of
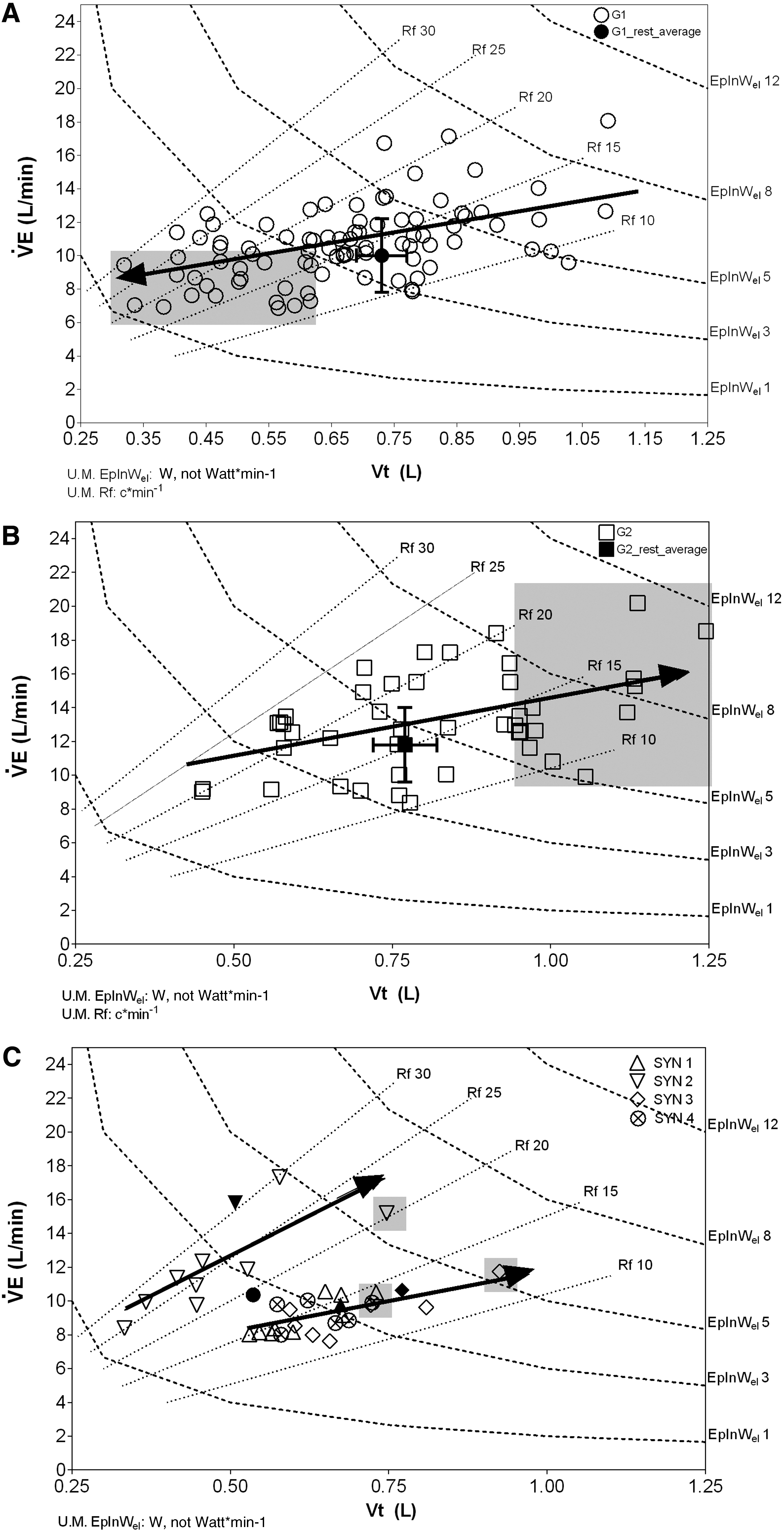
Pattern of breathing during the suspension test in G1
In G1 (Fig. 3A), due to the initial increase in
A different pattern of breathing in response to suspension was observed in G2, as suggested by the arrow's direction (Fig. 3B): indeed,
Figure 3C shows the pattern of breathing of the SYN: three participants displayed the same pattern of breathing and a common arrow is shown, whereas one participant was considered individually (another arrow was displayed). In all the SYNs, there was an initial decrease in
Oxidative metabolism
Figure 4A (right) shows a sudden increase in
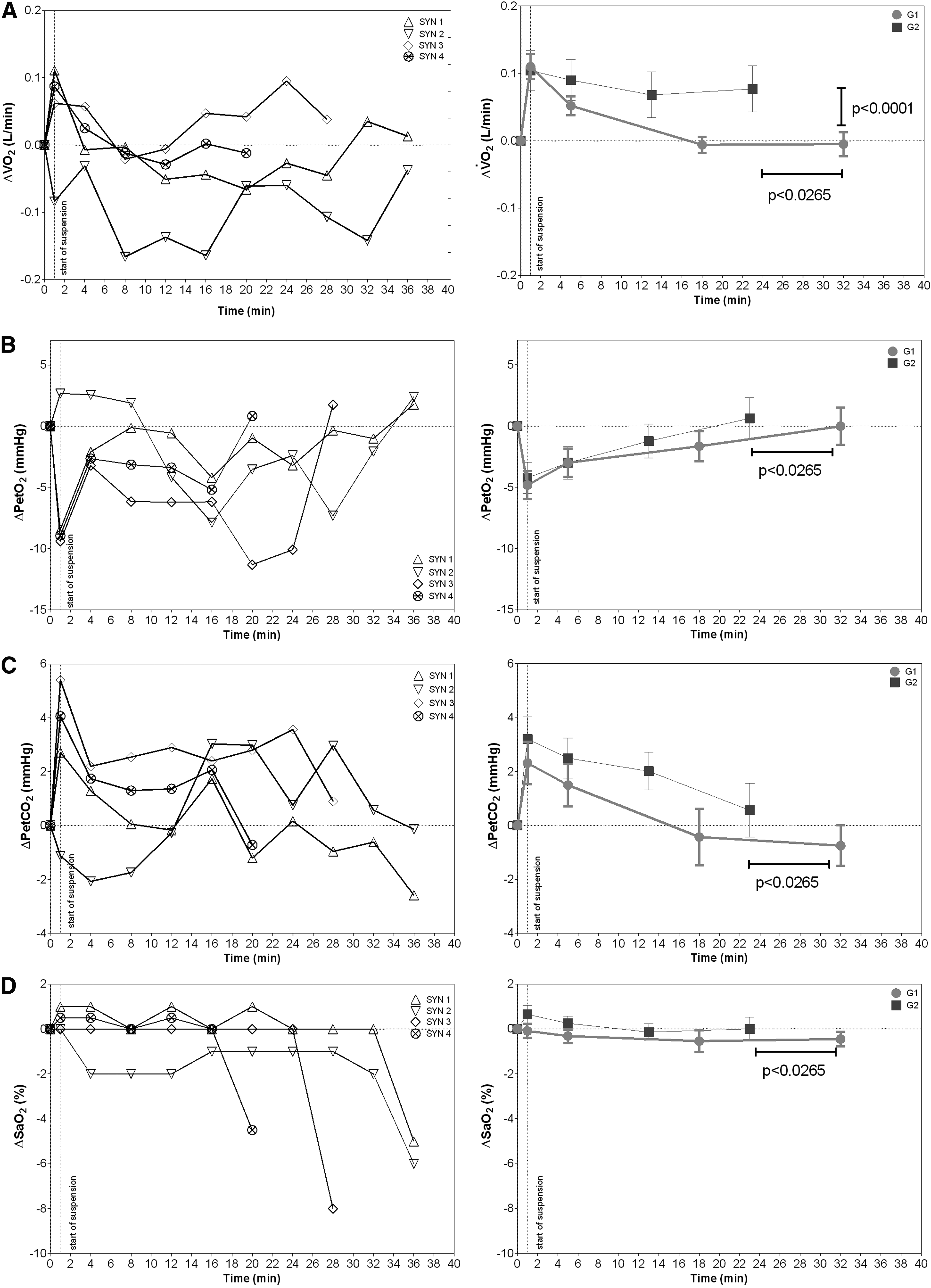
Time courses of changes in gas exchange values during the suspension test in SYN (left panels) and G1 and G2 (right panels). In
In SYN, a variable response at the onset of suspension was documented on average; a decrease in
Pulmonary volumes and lung diffusion capacity during suspension
Table 1 shows spirometry measures in resting condition (before wearing the harness), which did not differ among groups (SYN, G1, G2, and LOAD). Table 1 also shows the same variables, for the LOAD group, when the impact of chest loads was due to change in posture (clinostatism), suspension (
Pulmonary Function Test Parameters for Groups G1, G2, SYN, and LOAD
Orthostatism: sitting at rest; clinostatism: lying on the examination table; suspension: while hanging in the harness; chest/abdominal strap: while sitting and applying a pneumatic tourniquet cuff inflated at progressively increased pressure (25–50–75 mmHg).
p < 0.05 with respect to orthostatism in the LOAD group.
FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; FEF25–75, forced expiratory flux at 25%–75%; PEF, peak expiratory flow rate.
Cardiovascular and respiratory control
Figure 5 shows the average fluctuations in SBP plotted versus
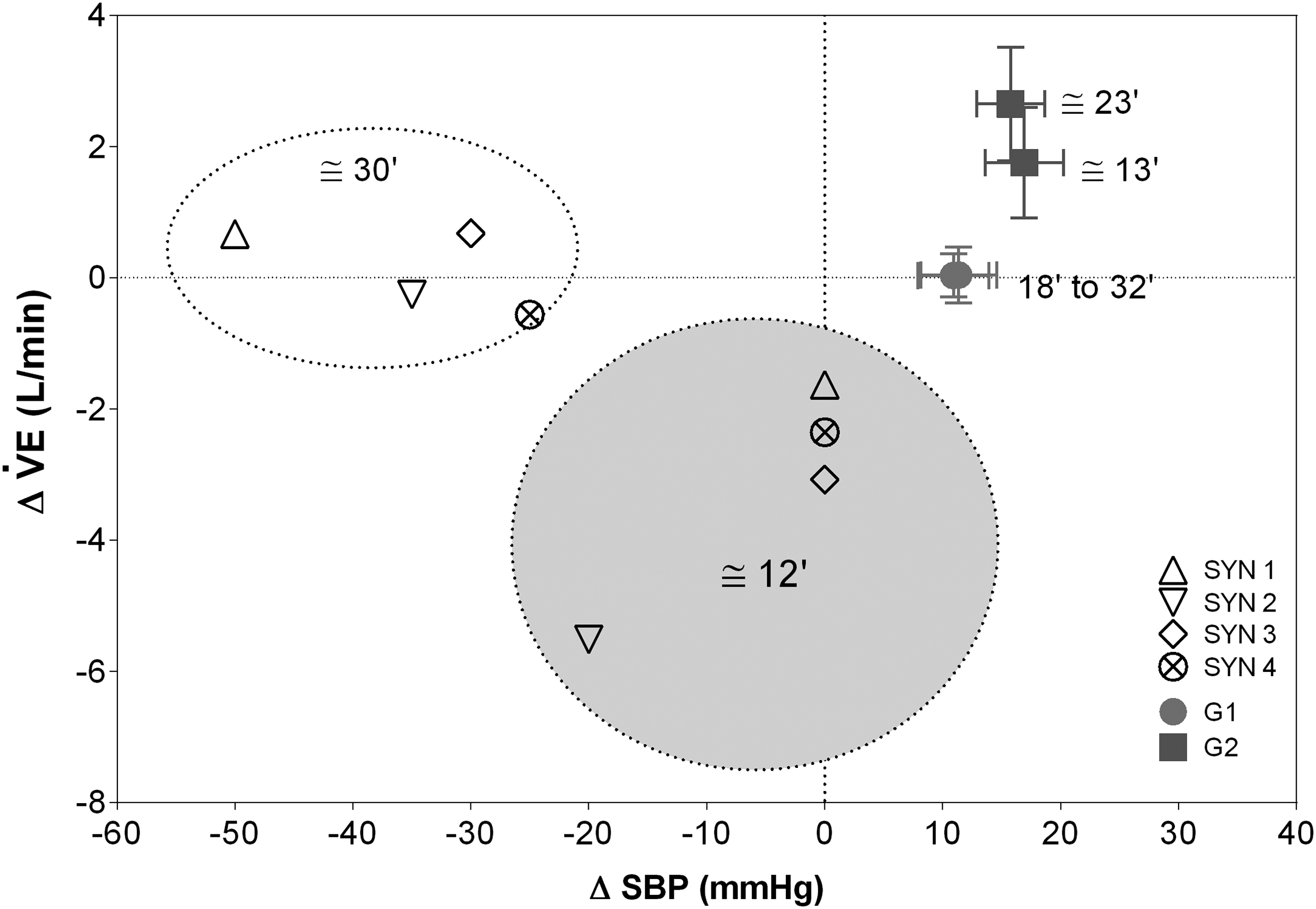
Relationships between variation of ventilation (Δ
Discussion
The pathophysiology of HHS depends on factors interfering with cerebral oxygenation, including the gravity-dependent pooling of blood and interstitial fluid in the lower parts of the body along with the deterioration of cardiovascular reflexes. This experiment helps us expand our knowledge about the potential effects of cerebral hypoxia by evaluating the impact of HHS on the pattern of breathing and respiratory reflexes. The study was performed on a relatively large number of healthy individuals, compared with previous studies on HHS, which gave us the opportunity to evaluate the individual variability in the pattern of breathing during the ST.
The results of the investigation suggested that participants who did not develop HHS were able to activate remedial responses through the O2 transport and utilization chain of various intensities to defend brain oxidative metabolism needs. Conversely in SYN, suspension triggered an imbalanced response of respiratory and cardiovascular reflexes leading to critical cerebral hypoxia.
The pattern of breathing
Severe hypoxia can be individually sustained by gas exchange and pH compensation, until a critical point of cerebral hypoxia is reached causing syncope (Subudhi et al., 2007; Convertino, 2014; Lanfranconi et al., 2017b). A crucial point in control of
In G1, the strategy allowing alveolar gases to be kept unaltered was characterized by a progressive shift of
Metabolic cost of the pattern of breathing
Indeed, the sharp increase in
This event, on a larger scale, is otherwise observed in the very first phase of an incremental exercise test when the rising of V
Otherwise, on the subsequent phases of the ST (after
Essentially, no such excitatory respiratory reflex was observed in SYN where a full inhibition of respiratory drives was found.
Mechanical constrains during suspension in harness
There is a general misinterpretation that wearing a harness, also when it perfectly fit the size of the climber/worker, limits the physiological lung ventilation by generating an external thoracic restriction. On the contrary, we are not prone to consider the harness by itself as cause of a potentially degenerated pattern of breathing. It seems that the ST caused a reflex respiratory response implying the intervention of respiratory centers, at brainstem level, due to specific sensory inputs. More to the point, it was not the harness model by itself the cause of an inconsistent pattern of breathing, but the sudden postural orthostatism with changes in the force distribution applied to the chest wall that payed a tribute in term of thoracic distortion. In case one is sitting on a chair with the harness, he/she does not experience any mechanical limitation of the chest wall. In fact, since spirometry forced dynamic air flow measurements were essentially unaffected by the ST (Table 1), one may otherwise speculate about a potential role of prolonged chest wall distortions as sensory triggers (from chest wall mechanoreceptors) affecting the reflex pattern of breathing during the motionless suspension (Van Noord et al., 1986; Nishino et al., 1992).
Certainly, the response to this sustained postural chest wall distortion in G1, that is,
The respiratory centers located in the brainstem, especially at the level of catecholaminergic neurons projecting to the paraventricular nucleus of the hypothalamus, might contribute to modulate the cardiorespiratory and neuroendocrine responses to hypoxia (Dampney et al., 2003; King et al., 2015).
An interesting consideration is related to the reduced spirometry values when the 50 and 75 mmHg chest–abdominal wall strappings were applied (Table1): from ergonometric perspectives, given the relatively short time for developing HHS, we might recommend that harnesses should be designed to assure full rib cage and diaphragmatic expansion to minimize upper abdominal and lower chest wall constriction. Indeed, in case one wears a harness that do not fit his/her size being too tight, the effect of suspension adds up to the consequence of postural harness restriction (i.e., augmented V
Suspension marks respiratory and blood pressure controls
The heterogeneity of the pattern of breathing in response to significant progressive cerebral hypoxia during the ST supports the fact that monitoring both cardiovascular and respiratory responses might provide useful predictors of individual trends toward less stable conditions of hemodynamic resiliency (Fig. 5). One may hypothesize that the difference in reflex cardiorespiratory response mostly reflects a change in sensory input as well as in brainstem processing and integration. The corresponding cardiac and respiratory control centers are anatomically in close proximity and physiologically widely interconnected. Convertino et al. (2009) suggested that although respiration is usually associated with gas exchange, acid–base balance, endocrine, and immune functions, a less appreciated function is the increase in venous return and cardiac filling due to a “respiratory vacuum pump” effect, resulting from the negative intrathoracic pressure created during inspiration.
This compensatory heart–lung interaction appears to be a natural mechanism in response to circulating volume reduction as seen in heart attacks: exacerbation of the respiratory pump by spontaneous gasping (elevated pattern of breathing) has been reported to occur in response to cardiac pump arrest and hypovolemia, where it has been associated with successful clinical outcome (Bobrow et al., 2008). Indeed, metaboreflexes originate from gasping, when a diminished cardiac output is present, leading to a vasoconstriction activation (via sympathetic stimulation). This response generates an increased blood pressure able to maintain sufficient perfusion to the active tissues (i.e., respiratory muscles) (Miller et al., 2002). Thus, in G2 and SYN, the hyperventilation response seems to be a reaction to cope with critical levels of cerebral hypoxia and may represent an important compensatory mechanism to optimize cardiac filling and prevent BP decrease.
The case of G1 participants is consistent with the notion that peripheral vasoconstriction plays a central role in maintaining BP: Convertino (2014) found that the control of systemic vascular resistance was greater in high tolerant orthostasis participants compared with low, in line with greater elevations in the circulating vasopressor hormones (vasopressin, angiotensin, and norepinephrine). An overdriven control of both vascular and respiratory centers can lead conversely to an intolerable stress of the systems and a rapid increase of energy expenditure of respiratory muscles to maintain
Contrarily to Convertino et al. (2009), in HHS, the failure in control of both
Conclusion
The present findings suggest that the ability to cope with hanging motionless in harness occurs in people developing less marked as well as more rapidly fading of fluctuations in both respiratory and cardiovascular reflex responses. Conversely, wider fluctuations in control of
Finally, based on our results, we recommend the more fairly term “harness hang syndrome” rather than “suspension trauma” for defining this potentially fatal condition.
Authors' Contribution Statement
Substantial contributions to the conception or design of the work: F.L., M.B., L.P., G.D., M.N. Substantial contributions to the acquisition and analysis of data: F.L., M.B., L.P., G.C., M.N. Substantial contributions to the interpretation of data: F.L., A.F., E.B., G.D., L.T. Drafting the work or revising it critically for important intellectual content: All authors. Final approval of the version to be published: All authors. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: all Authors.
Footnotes
Acknowledgments
We applied the “first-last-author emphasis” (FLAE) approach for the sequence of authors. We thank the brave participants for their cheerful cooperation. We sincerely thank Mr. Bejitual Berhanu as knowledgeable native speaker.
Author Disclosure Statement
No competing financial interests exist.