
Abstract
Objective:
To evaluate the safety and effectiveness of transcervical fibroid ablation (TFA) for symptomatic uterine fibroids in real-world settings.
Design:
Multicenter observational pragmatic study in the United Kingdom.
Methods:
Women with symptomatic uterine fibroids underwent TFA at two centers. TFA is an incision-less, uterine-sparing procedure that utilizes radiofrequency energy to reduce fibroid volume. Changes in symptom severity and health-related quality of life (HRQL) as measured by the Uterine Fibroid Symptom and Quality of Life (UFS-QoL) questionnaire (0–100 scale) were analyzed using linear mixed models at 3, 6, 9, 12, and 15–24 months of follow-up. Safety outcomes included 30-day readmissions, adverse events, and fibroid-related reinterventions.
Results:
Among 166 women (mean age 44 ± 6 years; range: 24–55 years), a mean of 1.7 ± 1.2 (range: 1–9) fibroids per patient were treated, with a maximum fibroid diameter of 4.7 ± 1.5 cm (range: 2–10 cm). Most (70%) procedures were performed in an outpatient clinic (analogous to in-office in the United States) under local anesthesia, with the remainder (30%) as a day-case procedure in an operating room under general anesthesia. All outpatient procedures were well-tolerated, with none abandoned due to pain or discomfort. The median follow-up duration was 6 months (range: 3–24 months). Symptom severity scores improved from 63 (95% CI: 59–66) at baseline to 32 (95% CI: 28–36) at 3 months (p < 0.001) and 31 (95% CI: 20–43) at final follow-up (p < 0.001). HRQL scores increased from 37 (95% CI: 33–41) at baseline to 70 (95% CI: 64–75) at 3 months (p < 0.001) and 74 (95% CI: 61–87) at final follow-up (p < 0.001). Freedom from event rates were 98.2% for 30-day readmission, 94.0% for adverse events, and 92.8% for fibroid-related reinterventions. No significant differences in outcomes were observed between patients treated in outpatient clinics under local anesthesia versus in an operating room under general anesthesia.
Conclusions:
This study provides real-world evidence that TFA is well-tolerated, has a favorable safety profile, and improves fibroid-specific symptom severity and quality of life over mid-term follow-up, irrespective of procedure setting and anesthetic approach. Given typical patient preferences for less invasive, uterus-sparing fibroid procedures, TFA merits consideration as a first-line interventional option for women with symptomatic uterine fibroids.
Introduction
Uterine fibroids (leiomyomata) are monoclonal benign tumors affecting most women by the time of their menopause, with a cumulative incidence of nearly 70% in White women and over 80% in Black women by age 50. 1 Uterine fibroids are responsible for substantial health burdens, with approximately two-thirds of affected women experiencing moderate or severe symptoms that impair quality of life, 2 and nearly one-third ultimately requiring surgical or interventional treatment. 3 The clinical manifestations may include heavy menstrual bleeding, painful periods, abdominopelvic pressure or pain, bladder dysfunction, dyspareunia, subfertility, and early pregnancy loss, which collectively compromise physical, social, and emotional well-being.4,5 This burden is further magnified by considerable diagnostic delays, with an average interval of 4 years between symptom onset and diagnosis, 6 while more than one-third of women with severe symptoms never seek medical evaluation. 7 Yet fibroids continue to grow at a median rate of 35% annually, making timely intervention crucial, especially for larger fibroids that may cause more severe symptoms and complications. 8
Initial management of uterine fibroids typically involves conservative approaches such as analgesics or lifestyle modification, though these rarely provide adequate long-term symptom control. 6 Pharmacological options such as hormonal contraceptives, gonadotropin-releasing hormone modulators, selective progesterone receptor modulators, and antifibrinolytics often fail to provide durable relief, with most women eventually opting for procedural treatment. 9 When symptoms persist despite conservative management, surgical interventions such as hysterectomy, myomectomy, and uterine artery embolization may be considered. However, these procedures frequently misalign with patient preferences, as surveys indicate that 79% of women with symptomatic fibroids prefer noninvasive treatment options, 51% prioritize uterus-preserving treatments, and 43% of women under 40 years prefer fertility-preserving approaches. 6 The discordance between available treatments and patient preferences represents a critical gap in uterine fibroid care.
Transcervical fibroid ablation (TFA) addresses this treatment gap as an incision-less, uterine-sparing procedure utilizing radiofrequency energy to induce coagulative necrosis within fibroids while preserving surrounding myometrium. Clinical studies of TFA have demonstrated fibroid volume reduction, significant symptom improvement, and high patient satisfaction across diverse populations.10–15 Additionally, TFA preserves fertility potential without adversely impacting subsequent pregnancy outcomes. 16 The procedure has gained endorsement from major professional organizations, with the American Association of Gynecologic Laparoscopists (AAGL) confirming its effectiveness in reducing fibroid volume, decreasing uterine bleeding, and improving quality of life, 17 and the National Institute for Health and Care Excellence (NICE) reporting that TFA provides effective treatment of uterine fibroids with high patient satisfaction and no major safety concerns. 18
Despite growing adoption, no studies have compared TFA outcomes when performed in an outpatient clinic versus an operating room. The objective of this pragmatic study was to generate real-world evidence on the safety and effectiveness of TFA for symptomatic uterine fibroids. We hypothesized that TFA would safely provide clinically meaningful improvements in patient-reported symptoms and health-related quality of life (HRQL), with comparable outcomes between procedures performed in an outpatient clinic under local anesthesia versus those performed as a day-case procedure in an operating room under general anesthesia.
Materials and Methods
Ethics
This study utilized de-identified data collected during routine clinical care in accordance with institutional policies. All patients were fully informed of the potential risks and benefits associated with TFA and provided written informed consent prior to participation. All study procedures were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. This article was prepared following the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 19
Design and setting
This was a multicenter observational pragmatic study of patients treated with TFA for symptomatic uterine fibroids at two National Health Service (NHS) hospitals in the United Kingdom (Manchester University NHS Foundation Trust; West Middlesex University Hospital, Chelsea and Westminster NHS Foundation Trust). Both centers had expertise in minimally invasive gynecological procedures and maintained facilities equipped for fibroid interventions in both outpatient clinics and operating room settings. The study enrolled consecutive eligible patients treated between September 2021 and November 2024.
Participants
The eligibility criteria reflected real-world clinical practice by including a heterogeneous sample of women (≥18 years) with symptomatic fibroids. Potential participants underwent transvaginal ultrasonography during screening to characterize the fibroids and confirm anatomical suitability for the procedure. Exclusion criteria included Fédération Internationale de Gynécologie et d’Obstétrique (FIGO) type 0 (pedunculated intracavitary) or type 7 (subserosal pedunculated) fibroids, cervical fibroids, current pregnancy, active pelvic infection, suspected gynecological malignancy, or metallic implants in the pelvis or hip. No restrictions were imposed on symptom severity or desire for future fertility.
Procedure
Four consultant gynecologists (two per site) performed TFA in outpatient clinics (analogous to in-office in the United States) using local anesthesia or in hospital-based operating rooms using general anesthesia. All investigators had minimal prior TFA experience, with each having performed 0–3 cases before enrolling patients in the study. The choice of procedure setting and anesthetic protocol was individualized based on patient characteristics and clinical judgment. Antibiotic prophylaxis was administered at the physician’s discretion based on patient risk factors. Patients received premedication with a nonsteroidal anti-inflammatory drug (typically diclofenac 100 mg rectally or ibuprofen 400 mg orally), plus misoprostol 400 mg per vaginum if difficult cervical dilatation was anticipated.
The TFA procedure (Sonata System, Hologic, Marlborough, MA, United States) has been previously described. 20 Briefly, the system integrates a high-resolution intrauterine sonography probe with a radiofrequency ablation handpiece in a single delivery system that enables real-time visualization, targeting, and ablation of uterine fibroids. The system provides a graphical overlay on the live ultrasound image that delineates both the target ablation area and thermal safety border. This visualization ensures that ablation remains confined within the fibroid while maintaining the thermal safety border within the uterine serosa. Although a single ablation may sufficiently treat a fibroid, multiple ablations could be performed during the same procedure depending on fibroid number, size, location, and geometry.
Following the procedure, patients were monitored until meeting discharge criteria, including stable vital signs, adequate pain control, independent ambulation, spontaneous micturition, and absence of significant vaginal bleeding. Post-procedural analgesia was individualized based on pain severity. Patients were instructed to report post-procedural adverse events including excessive bleeding, malodorous vaginal discharge, fever >38°C, worsening abdominal pain unresponsive to prescribed analgesics, or general malaise. Additionally, investigators conducted follow-ups during clinical visits and via telephone according to institutional protocols to assess adverse events and determine changes in fibroid-specific symptoms and quality of life.
Outcome measures
Symptom severity and HRQL were assessed using the Uterine Fibroid Symptom and Quality-of-Life (UFS-QOL) questionnaire administered before the procedure and during follow-up. 21 This disease-specific questionnaire comprises the symptom severity score (SSS) and HRQL subscales. The SSS evaluates bleeding severity, pelvic pressure, and urinary symptoms, while the HRQL assesses concern, activities, energy/mood, control over health/life, self-consciousness, and sexual function. Both subscale scores were transformed to a 0–100 scale, with lower SSS values indicating less severe symptoms, and higher HRQL values indicating better quality of life. Safety outcomes included procedural and post-procedural adverse events, 30-day hospital readmissions, and reinterventions for persistent or recurrent fibroid-related symptoms.
Statistical analysis
Continuous variables were presented as means with standard deviations for normally distributed data or medians with ranges for non-normally distributed data. Categorical variables were presented as percentages. Changes in SSS and HRQL scores from baseline were analyzed using linear mixed models for repeated measures at 3, 6, 9, 12, and 15–24 months of follow-up, and reported as least squares means with 95% confidence intervals (95% CIs). Subgroup analyses compared patients treated in outpatient clinics under local anesthesia versus those treated in operating rooms under general anesthesia using linear mixed models for continuous variables and Fisher’s exact tests for categorical variables. Statistical significance was defined as p < 0.05 for all analyses. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
A total of 166 women (mean age 44 ± 6 years; range: 24–55 years) were treated with TFA. One investigator from each site performed the majority of procedures (96 and 64 cases), while the other two performed four and two cases, respectively. Baseline UFS-QoL subscale scores were 63 ± 18 for SSS and 37 ± 23 for HRQL, indicating substantial symptom burden and reduced quality of life. Most (70%) procedures were performed in an outpatient clinic (referred to as in-office in the United States) under local anesthesia via intracervical block. Supplemental inhaled analgesia with a 50:50 nitrous oxide/oxygen blend or methoxyflurane was administered in 36% of cases. The remainder (30%) were day-case procedures performed in hospital operating rooms under general anesthesia. A wide range of fibroid types were treated, with the most common being intramural (56%) and submucosal (26%). A mean of 1.7 ± 1.2 (range: 1–9) fibroids were treated per patient, with a maximum treated fibroid diameter of 4.7 ± 1.5 cm (range: 2–10 cm) per patient (Fig. 1). Each fibroid received a median of 2 (range: 1–7) ablations. Baseline characteristics were similar between patients treated in the outpatient clinic versus operating room settings (Table 1). The procedure was well-tolerated with a mean subject-reported pain severity of 3 (0–10 scale) among patients treated in outpatient clinics, with no procedures abandoned due to pain or discomfort. In one patient with two fibroids, one ablation was discontinued because it was an inaccessible type 7 fibroid. Nevertheless, the patient reported satisfaction with the results at follow-up.

Uterine fibroid characteristics in patients treated with transcervical fibroid ablation. Histograms represent the frequency of treated fibroid types (top panel) and diameters (bottom panel).
Patient Characteristics and Procedural Details in Women Receiving Transcervical Fibroid Ablation a
Values are mean ± standard deviation [range], or percentage unless otherwise noted.
Comparison of outpatient clinic versus operating room.
Values are median [range].
FIGO, Fédération Internationale de Gynécologie et d’Obstétrique; HRQL, health-related quality of life; SSS, symptom severity score; UFS-QoL, Uterine Fibroid Symptom and Quality-of-Life.
Patients were followed for a median of 6 months (range: 3–24 months). The SSS scores improved from 63 (95% CI: 59–66) at baseline to 32 (95% CI: 28–36) at 3 months and 31 (95% CI: 20–43) at the final follow-up. The change from baseline was −31 points (95% CI: −35 to −26; p < 0.001) at 3 months and −31 points (95% CI: −42 to −20; p < 0.001) at the final follow-up interval, representing a 50% decrease from baseline. The HRQL scores increased from 37 (95% CI: 33–41) at baseline to 70 (95% CI: 64–75) at 3 months and 74 (95% CI: 61–87) at the final follow-up. The change from baseline was 33 points (95% CI: 27–38; p < 0.001) at 3 months and further improving through the final follow-up interval (37 points; 95% CI: 24–51; p < 0.001), representing a 101% increase from baseline (Fig. 2).
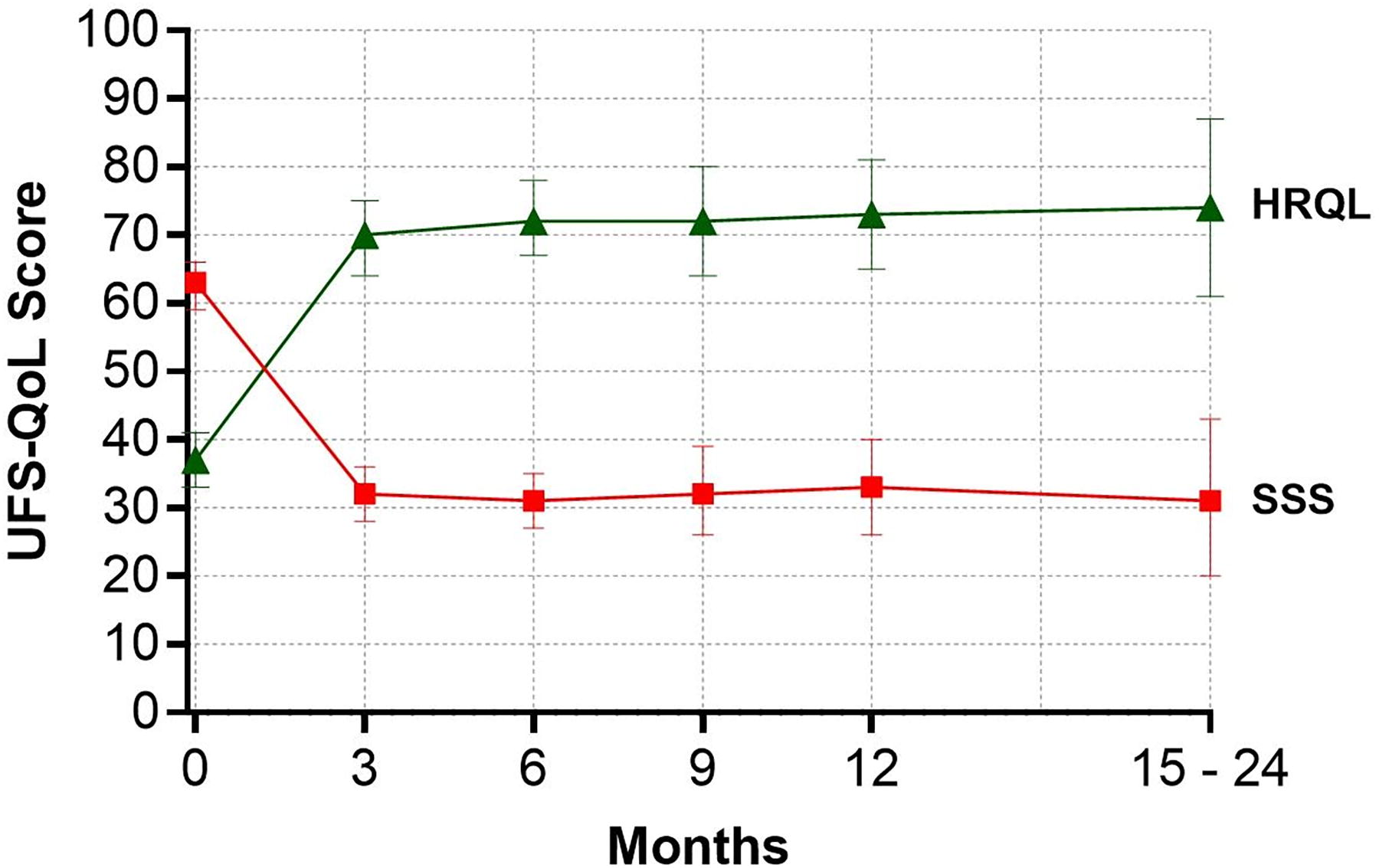
Change in symptom severity score (SSS) and health-related quality of life (HRQL) subscales of the Uterine Fibroid Symptom and Quality-of-Life (UFS-QoL) Questionnaire following transcervical fibroid ablation. Lower SSS scores indicate less severe symptoms. Higher HRQL scores indicate better quality of life. Plotted values are least squares mean and 95% confidence interval. The change from baseline was statistically significant for SSS and HRQL subscales (both p < 0.001).
Freedom from an adverse event was 94.0% (156/166). Three patients required readmission within 30 days of TFA for sepsis (1), fever (1), and heavy vaginal bleeding (1), resulting in a 98.2% freedom from 30-day readmission rate. The patient readmitted with sepsis received intravenous antibiotic therapy and was subsequently discharged without further complications. Additional adverse events included postoperative pain (5), uterine perforation during cervical dilatation that did not affect procedure completion or result in complications (1), and dysmenorrhea (1). During follow-up, 92.8% (154/166) of patients remained free from fibroid-related reintervention. Reinterventions included hysteroscopic myomectomy (5), hysterectomy (4), laparoscopic myomectomy (1), endometrial ablation (1), and repeat TFA (1). Among patients undergoing reintervention, only one experienced an adverse event (postoperative pain), which necessitated laparoscopic myomectomy. All other adverse events occurred in patients who did not require reintervention. Reintervention was generally performed for inadequate symptom relief.
No statistically significant differences were observed in the clinical outcomes of patients treated in an outpatient clinic versus operating room settings. Both groups reported clinically important improvements in SSS and HRQL scores through the final follow-up (all p < 0.001), and freedom from adverse event, 30-day readmission, and reintervention rates were comparable (Table 2).
Outcomes by Procedure Setting in Women Receiving Transcervical Fibroid Ablationa
Values are mean change (95% CI) or percentage.
Between-group p-value derived from linear mixed model with time-by-procedure setting interaction.
Derived from Fisher’s exact test.
*p < 0.001 for change over time.
HRQL, health-related quality of life; SSS, symptom severity score; UFS-QoL, Uterine Fibroid Symptom and Quality-of-Life.
Discussion
This pragmatic study demonstrated that TFA can be safely and effectively performed in real-world clinical settings to treat symptomatic uterine fibroids, with comparable outcomes whether performed in an outpatient clinic under local anesthesia or as a day-case procedure in an operating room under general anesthesia. We observed approximately 50% reductions in SSS scores and 100% improvements in HRQL scores early in follow-up, which were sustained beyond 1 year. The magnitude of these improvements substantially exceeded established clinical success thresholds. The 31-point reduction in the mean SSS score was more than triple the 10-point minimal clinically important difference (MCID), 22 while the 37-point HRQL improvement nearly doubled the 20-point MCID. 23 These outcomes were achieved with a favorable safety profile, as evidenced by low rates of adverse events, 30-day hospital admissions, and fibroid-related reinterventions. The ability to safely achieve clinically meaningful symptom improvement with TFA in a heterogeneous sample of women treated in diverse, real-world settings supports its consideration as a first-line treatment option for women with symptomatic uterine fibroids.
Our findings align with and extend previous research on TFA. We observed a mean 31-point decrease in SSS and a 37-point increase in HRQL, which are comparable to previous systematic reviews of radiofrequency fibroid ablation performed across diverse treatment settings where SSS decreased by 33–43 points24–27 and HRQL increased by 29–42 points.24–27 Similarly, the 7.2% surgical reintervention rate in the current study is comparable with the 2.7%–11.5% rates reported in prior reviews of radiofrequency fibroid ablation. For context, surgical reintervention rates of up to 23.5% have been reported for other surgical fibroid treatments.28–31 The successful use of TFA in outpatient clinics using local anesthesia contrasts with the predominant use of general anesthesia for traditional fibroid interventions, suggesting potential advantages in patient choice, recovery time, and resource utilization. By achieving comparable clinical outcomes to operating room settings with simplified resource requirements, the option to perform TFA in outpatient clinics addresses well-documented barriers to fibroid care, especially for underserved populations who face disproportionate access challenges. 32
The favorable clinical outcomes observed in this study are likely attributable to several key elements in the procedural approach and periprocedural protocols. First, procedural safety was facilitated by integrating real-time intrauterine sonography with radiofrequency ablation to provide operators with immediate visual feedback to maintain optimal safety margins. Second, performing multiple ablations within a single procedure allows clinicians to address multiple fibroids of varying sizes and anatomical locations. Third, local anesthesia protocols developed for TFA in the outpatient clinic provided adequate pain control while enabling rapid recovery and discharge. Finally, dedicated outpatient procedure rooms with appropriate staffing and monitoring capabilities facilitated efficient care delivery without compromising safety standards. Collectively, these elements enabled effective fibroid treatment with TFA regardless of procedural setting.
The feasibility of performing TFA in the outpatient clinic has important implications for health care delivery systems that are increasingly constrained by capacity limitations and cost pressures. Offering TFA outside traditional operating rooms may significantly improve access to care by reducing scheduling delays and lowering geographic barriers to specialty care. From the patient perspective, treatment in outpatient clinics may reduce pre-procedure anxiety, allow faster return to normal activities, and improve the overall care experience, which are considerations important for women balancing caregiving and professional responsibilities. These advantages position TFA as a patient-centered treatment option that enhances accessibility by expanding patient choice and better aligning with typical patient preferences for less invasive, uterus-sparing interventions. 6
Several limitations of this study warrant consideration. First, the observational study design without a concurrent control group limits the ability to directly compare outcomes with alternative treatments. However, indirect comparisons with prior studies of radiofrequency fibroid ablation suggest similar safety and effectiveness.24–27 A randomized trial comparing TFA to minimally invasive myomectomy is underway 33 and will provide more definitive comparative data. Second, this study reports mid-term outcomes of TFA, while longer-term follow-up would help determine the durability of the observed treatment effects. Multiple studies have already demonstrated sustained effectiveness and quality of life benefits of TFA over the long-term,14,34,35 which suggests the potential for long-term benefits in our patient population. Third, while all procedures were performed by consultant gynecologists who attained TFA experience during the study period, data from their initial cases are included in this analysis, which supports the generalizability of results to operators with limited prior experience. Finally, while economic models indicate that health care payer costs with TFA are lower than those for myomectomy and hysterectomy, 36 our study did not collect cost data, which limits direct assessment of potential economic benefits of this approach.
Conclusion
This study provides real-world evidence that TFA is well-tolerated, has a favorable safety profile, and improves fibroid-specific symptom severity and quality of life over mid-term follow-up, irrespective of procedure setting and anesthetic approach. Given typical patient preferences for less invasive, uterus-sparing fibroid procedures, TFA merits consideration as a first-line interventional option for women with symptomatic uterine fibroids.
Footnotes
Acknowledgments
The authors are grateful to the subjects for their participation in this study.
Authors’ Contributions
R.G.: Conceptualization, data curation, investigation, resources, writing—review and editing. L.M.: Formal analysis, methodology, project administration, software, writing—original draft. N.N.: Conceptualization, data curation, investigation, resources, writing—review and editing.
Author Disclosure Statement
R.G. reports no conflicts of interest. L.M. reports consultancy with Hologic. N.N. reports no conflicts of interest.
Funding Information
No funding was received for this study.