
Abstract
Purpose/Objective:
Mixed urinary incontinence (MUI) is the coexistence of stress urinary incontinence (SUI) and urge urinary incontinence (UUI). MUI can be a challenging condition to treat, and there continues to be a demand for successful nonsurgical interventions if possible. This study evaluates the efficacy of combining bipolar radiofrequency (RF) energy to the vaginal canal, electrical muscle stimulation (EMS) of the pelvic floor, and patient education in the treatment of MUI in females.
Methods:
A prospective study that evaluates RF and EMS in female patients with moderate MUI. RF and EMS treatments were administered three times, 2 weeks apart. Patients were also educated on exactly what MUI is and how to appropriately utilize their pelvic floor muscles. Outcome measures assessed included both objective (cough stress test to measure pad weight) and subjective (Incontinence Quality of Life [iQOL]; Medical, Epidemiological, and Social Aspects of Aging [MESA] Urge Incontinence [UI], MESA Stress Incontinence [SI], Female Sexual Function Index [FsFI]; and Urogenital Distress Inventory-6 [UDI-6]).
Results:
In total, 31 women underwent the combination of RF, EMS, and patient education, resulting in significant improvement in MUI symptoms (PGI: 82% indicated feeling improvement) after 3 months of treatment in all measures.
Conclusion:
RF and EMS in conjunction with patient education via a three-treatment protocol was found to be efficacious and safe for treating women with MUI. Future studies should be done to further elucidate optimal treatment protocols for MUI and patients followed up for longer periods of time to determine the durability of this regimen.
Introduction
Mixed urinary incontinence (MUI), characterized by a combination of stress and urge associated leakage, is a common problem, affecting 16% of women in the United States according to recent data from the National Health and Nutrition Examination Survey 1 and up to 30% of women worldwide according to the International Continence Society (ICS). 2 The economic, psychosocial, and health-related quality of life costs of urinary incontinence (UI) are substantial, with the burden of MUI greater than either pure stress urinary incontinence (SUI) or urge urinary incontinence (UUI) subtypes.3,4
Current guidelines from the American Urologic Association (AUA) and the Society of Urodynamics, Female Pelvic Medicine, and Urogenital Reconstruction (SUFU) consider SUI and UUI as independent problems. While the first line of treatment for both SUI and UUI includes pelvic floor muscle exercise, their treatment options otherwise commonly aggravate the other symptom complex. With treatments for SUI potentially aggravating urgency symptoms 5 and pharmacotherapy or bladder chemodenervation for UUI carrying significant side effects as well as risks of incomplete bladder emptying that can worsen SUI. 6 Pelvic floor exercise is a low-risk and potentially effective treatment option for SUI, UUI, and MUI. However, physical limitations, poor technique, and difficulty accessing guidance from a trained physical therapist can prevent patients from experiencing its benefits. 7
This pilot study aims to determine whether the combination of bipolar radiofrequency (RF) technology and electrical muscle stimulation (EMS) in conjunction with patient education is a safe and effective treatment for MUI. When applied to the vaginal skin, bipolar RF has been shown to increase collagen and elastin, improving connective tissue support and flexibility; 8 both of these are implicated in the pathophysiology of SUI and UUI. 9 Unlike conventional monopolar RF energy distribution, bipolar RF enables more targeted local application of energy, with a larger and more uniform thermal zone for more efficient treatment. 10 A recent study showed bipolar RF to be superior to monopolar RF in the treatment of SUI and stress predominant MUI. The FormaV (InMode, Lake Forest, CA) device used in this study uses a narrow probe to apply bipolar RF energy at an output frequency of 1 MHz to the vaginal epithelium (Fig. 1a).

The FormaV radiofrequency and vTone electrical muscle stimulation devices.
Percutaneous EMS induces involuntary muscle activity, which varies with the pattern of the stimulus applied: constant electrical stimulation can exhaust the muscle to promote its reflex relaxation, while alternating current promotes muscle tone and strength. 11 While this activity is involuntary, intravaginal EMS can improve patients’ purposeful pelvic floor exercise by helping them to identify the proper muscles to use and hastening improvements in muscle strength and flexibility beyond their volitional capability. 12 The vTone (InMode, Lake Forest, CA) device used in this study is placed intravaginally, to apply an alternating electrical stimulus to the adjacent muscles of the pelvic floor (Fig. 1b).
Finally, educating patients regarding what exactly MUI is and how to appropriately utilize their pelvic floor muscles can improve complaints of stress, urge, or mixed incontinence. The patient education can specifically focus on the synergistic relationship between the detrusor muscle and the pelvic floor muscles as well as training patients how to appropriately contract their pelvic floor muscles during bouts of increased intra-abdominal pressure. 13 The following study was undertaken with the objective of determining whether patients with MUI symptoms would show significant improvement after being educated on their condition and undergoing bipolar RF treatment of the vaginal canal as well as EMS stimulation of the pelvic floor.
Materials and Methods
This study was approved by the Sterling Institutional Review Board (IRB) (Atlanta, GA) (IRB number: 8485, IRB approved 12/08/2020). It represents a prospective case series of 31 women recruited at two sites between July 6, 2021, and April 20, 2023. The inclusion criteria included age 20–74 years old with moderate-to-severe MUI based on the Medical, Epidemiological, and Social Aspects of Aging (MESA) UI questionnaire; this means a 7–18 in the urgency incontinence category or 10–18 in the stress incontinence (SI) category. The exclusion criteria included severe concurrent conditions, such as cardiac disorders (including a history of implanted pacemaker or artificial defibrillator), epilepsy, uncontrolled hypertension, history of coagulopathy or use of anticoagulants, immunocompromise, liver or kidney diseases, history of genital Herpes Simplex Virus (HSV), and a current diagnosis of or a history of cancer or premalignant condition in the treatment area. Permanent implants in the genitourinary region were treated as exclusion criteria including vaginal metal piercings, intrauterine contraceptive devices (IUCD or ICD or coil or any other device made of metal), metal plates and screws, silicone implants, or an injected chemical substance. Active genital dermatologic conditions such as sores, psoriasis, eczema, and rash along with a history of HSV were treated as exclusion criteria. Subjects were not enrolled if they had a history of skin disorders, keloids, abnormal wound healing, as well as very dry and fragile skin. Pregnancy and breastfeeding were also treated as exclusion criteria. To participate, patients needed to be 6 months removed from isotretinoin treatment as well as treatments such as light, CO2 laser, or RF in the vulvovaginal area.
All patients were educated verbally about the condition of MUI and instructed on how to appropriately utilize their pelvic floor muscles. This included instructions on contracting their pelvic floor muscles 10 times per day for 10 seconds each time. Also instructed on contracting their pelvic floor when they experience urgency or bouts of increased intra-abdominal pressure.
Enrolled patients were treated with InMode’s FormaV RF device (Fig. 1a) followed by the vTone EMS device (Fig. 1b) in the same visit (see Supplementary Appendix Fig. S1 for treatment and follow-up timeline). A baseline medical history, including a detailed medication list, and physical examination were completed. Demographic data, including gender, age, and race, were collected. All subjects had their baseline pad weight determined by a standardized cough stress test (CST) at baseline and after 3- and 6 months post treatment. During the CST, subjects were requested to void 30 minutes prior and then drink 0.5 L of water. A pre-weighted pad was then applied, and the subject was asked to cough three times in a standing position—after which the pads were weighed. All subjects also completed the Incontinence Quality of Life (IQOL) (Supplementary Appendix Fig. S2); MESA-UI Questionnaire (Supplementary Appendix Fig. S3), Urogenital Distress Inventory-6 (UDI-6) (Supplementary Appendix Fig. S4), and Female Sexual Function Index (FsFI) questionnaires (Supplementary Appendix Fig. S5) at baseline, 3 months, and 6 months. UDI-6 was also completed at 1 month. A Patient-Reported Global Impression of Improvement (PGI) (Supplementary Appendix Fig. S6) and an assessment as to the satisfaction with the cost of the procedure (Supplementary Appendix Fig. S7) was completed at 3 and 6 months.
Three identical treatment regimens of FormaV and vTone were performed. Subjects in this study first underwent treatment with the Intravaginal FormaV RF system. The external genitalia were shaved, and the bladder was emptied prior to treatment. Treatment temperature cutoff was set to 43°C and energy level was set to 20 W–25 W with a frequency of 80 Hz and pulse width of 200 μs. Water-based ultrasound gel was applied to the FormaV probe as it was inserted into the vagina to the apex of the vaginal canal. Proper contact between the probe and the vaginal epithelium was ensured during the entire delivery of bipolar RF energy in a circumferential manner. The vaginal canal was divided into four quadrants, and RF energy was delivered equally to all four quadrants proximally to distally until the entire length and circumference of the vaginal canal had adequate treatment time of 15 minutes at the optimal temperature of 43°C. Immediately after receiving the RF energy treatment, the subjects were treated with vTone EMS. The EMS probe was inserted into the vaginal introitus until only the plastic rim at the base of the probe was visible. It was ensured that the metal electrodes conducting the electrical pulses were in continuous contact with the tissues. Electrodes were aligned to the sides of the vaginal canal by positioning the probe handle vertically. This ensured that EMS contractions would optimally target the pelvic floor muscles. As per protocol, the EMS settings gradually increased to an intensity setting of 50 with a pulse width of 200 and frequency of 80 Hz based on the patient’s comfort and intensity of pelvic floor muscle contractions. The same settings for both RF and EMS were used on all patients. Treatment time was 30 minutes for a full, effective treatment with the EMS alternating between the two sides with a 2-second on-time and 2-second off-time. After both procedures were completed, each patient was assessed for adverse effects and provided posttreatment instructions.
Results
A total of 31 women were enrolled in the study from July 6, 2021, to April 20, 2022, across two sites. The average age of the subjects was 54.68 years (range, 31–74).
A post hoc power analysis was conducted to ensure the study was sufficiently powered to detect statistically significant differences that were considered moderate (effect size f = 0.25). Results indicated that the required sample size to achieve 80% power for detecting a medium effect and at a significance criterion of α = 0.05 would be 28 patients.
All data was analyzed via paired-samples t-tests or repeated samples ANOVAs with three or foue repetitions.
The PGI instrument, which was administered at 3 months and 6 months post treatment, displayed scores ranging from 2 to 5, with higher scores denoting improvement after the treatment. The mean PGI was 4.04 (±0.74) at 3 months and 3.79 (±0.88) at 6 months (Fig. 2, Table 1). The paired-samples t-test was not statistically significant, indicating that PGI scores did not differ from 3 months to 6 months after treatment (p = 0.14).
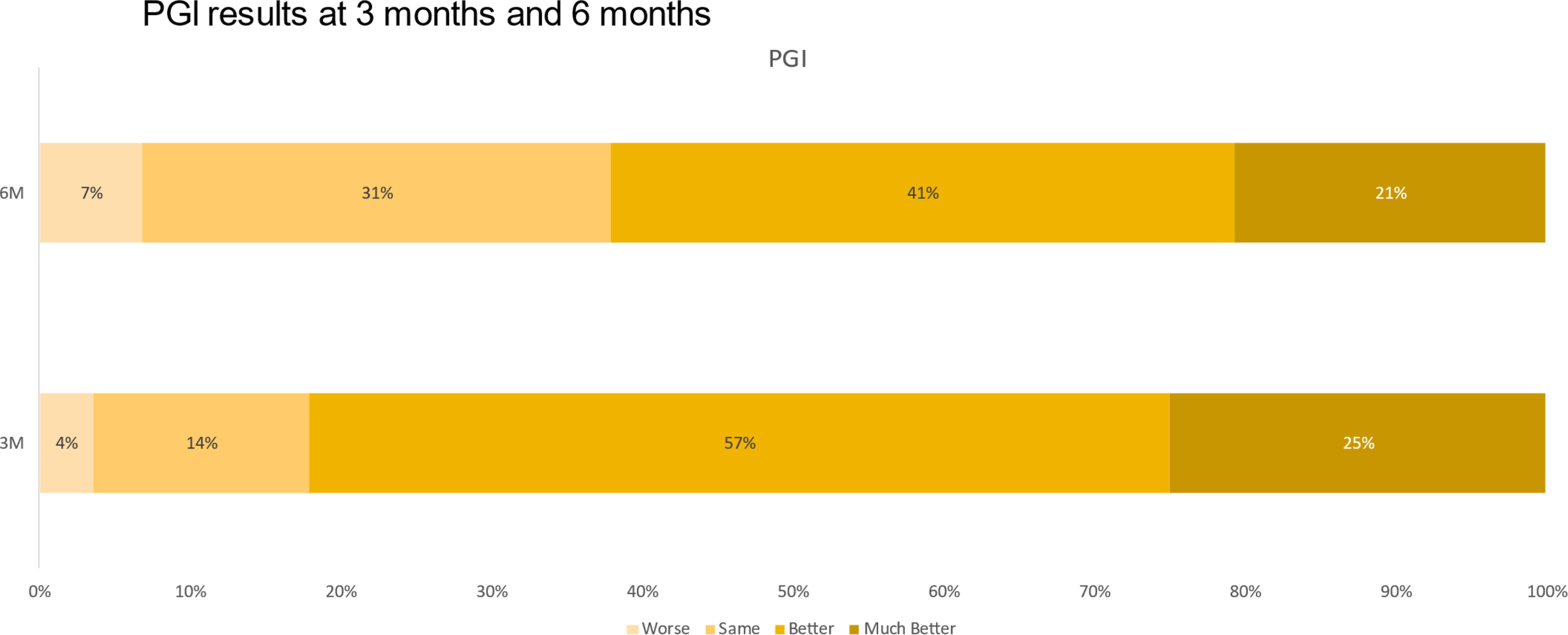
Patient-Reported Global Impression of Improvement results at 3 months and 6 months.
Patient-Reported Global Impression and Pay for Procedure Statistical Information of the Paired-Samples t-Test
3- and 6-month mean and paired-samples t-tests from patient global impression of improvement and pay for procedure data. The paired-samples t-tests were not statistically significant, indicating that these data did not differ from 3 months to 6 months after treatment.
PGI, Patient-Reported Global Impression of Improvement.
At 3 months and 6 months, patients were also asked what they would be willing to pay for the procedure; a higher average indicates the patient was willing to pay more money, with the lower average indicating willingness to pay less. There was no difference in what the patients were willing to pay at 3 months and 6 months (p = 0.28). In general, patients were most likely to say they would be willing to pay between $250 and $500 at both follow-up intervals (Fig. 3). Table 1 displays the relevant statistical information of the paired-samples t-test.
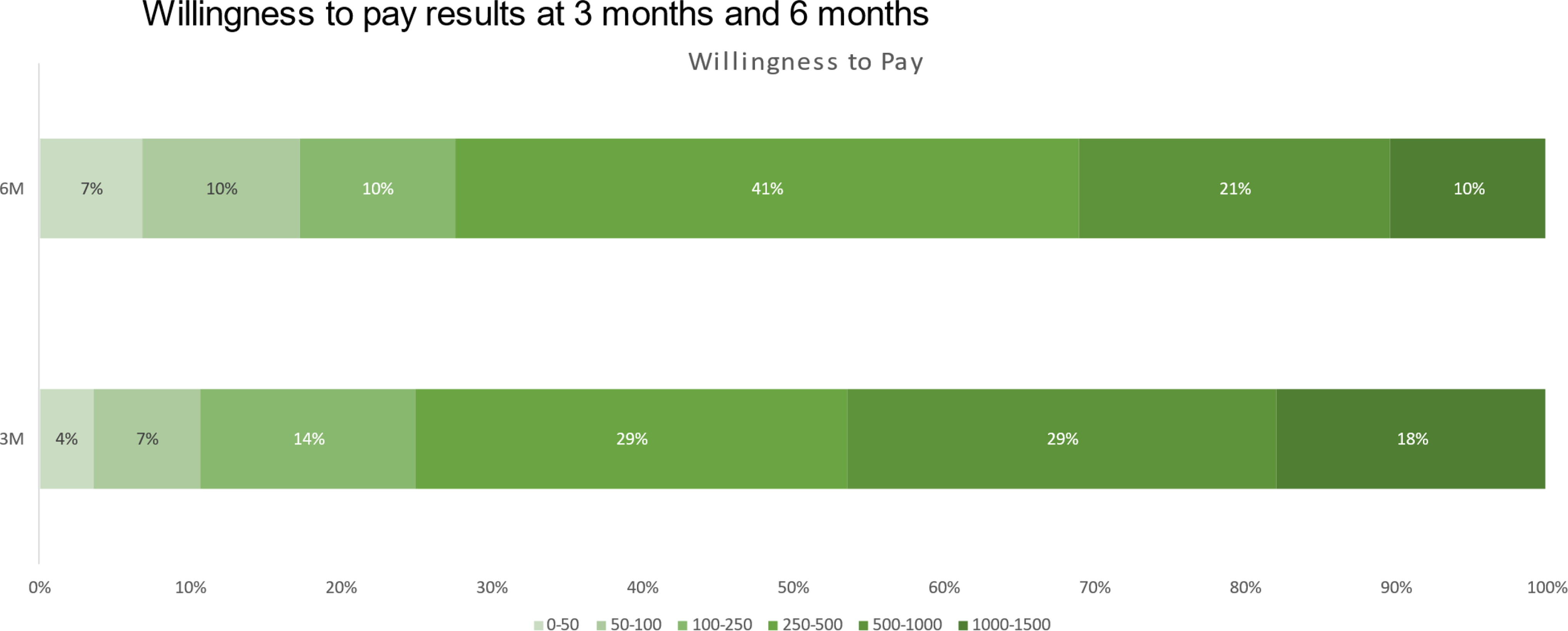
Results of patients’ willingness to pay for procedure at 3- and 6-month follow-up intervals.
The remainder of the data were analyzed via repeated-samples Analysis of Variance (ANOVA) tests. The follow-up time period mean values, standard deviation values, and pairwise comparison p-values (i.e., the paired-samples t-tests) are reported in the tables after the paragraphs reporting the results of the ANOVA test results.
The pad weight after CST ranged with actual scores from 0 to 91 g. Measurements were taken at baseline, 3 months, and 6 months. The ANOVA test was statistically significant, and the baseline average was significantly higher than both the 3-month and 6-month averages, indicating that CST scores improved from baseline to 3 months, then stayed improved at 6 months; F(2, 54) = 6.97, p = 0.002 (Table 2). Seventeen percent of patients had no change from baseline to 6 months and 2 patients had an increase in CST pad weight. Among those who experiences a decrease, no patients had a <50% decrease. Ninety-six percent of patients had a ≥50% decrease from baseline to 6 months post treatment, and 72% of patients no longer leaked urine with CST at 6 months.
Clinical and Self-Reported Outcomes Before and After the Three-Treatment Regimen
Measurements of cough stress test pad weight, iQOL, MESA SI, MESA UI, FSFI at baseline, 3, and 6 months. MESA urinary incontinence questionnaire separated into stress and urge sections for the purposes of this data analysis. ANOVA testing results indicated for baseline to 3 months, baseline to 6 months, and 3 months to 6 months.
FsFI, Female Sexual Function Index; iQOL, Incontinence Quality of Life; MESA SI, Medical, Epidemiological, and Social Aspects of Aging Stress Incontinence; MESA UI, Medical, Epidemiological, and Social Aspects of Aging Urge Incontinence.
The iQOL ranged with standardized scores from 1 to 100; it is a composite score of 22 questions, each was assessed via a 1 (extremely) to 5 (not at all) scale. Thus, the higher the value of the score, the better the patient’s assessment is of improvement after treatment. Measurements were taken at baseline, 3 months, and 6 months. The ANOVA test was statistically significant, indicating that iQOL scores improved from baseline to 3 months, then stayed improved at 6 months; F(2, 54) = 43.14, p < 0.001 (Table 2). In addition, 86% of patients had a 2.5-point improvement from baseline to 6 months, indicating a clinically meaningful improvement.
The MESA additive SI instrument ranged with theoretical scores from 1 to 27, with lower values (1–9) indicating mild symptoms, and higher values (19–27) indicating severe symptoms. Measurements were taken at baseline, 3 months, and 6 months. The ANOVA test was statistically significant, indicating that MESA-SI scores improved from baseline to 3 months, then stayed improved at 6 months; F(2, 54) = 23.36, p < 0.001 (Table 2). Moreover, from baseline to 6 months, 47% of patients had a score improvement of at least five, indicating a clinically meaningful improvement.
The MESA additive UI instrument ranged with theoretical scores from 1–18, with lower values (1–6) indicating mild symptoms, and higher values (13–18) indicating severe symptoms. Measurements were taken at baseline, 3-months, and 6-months. The ANOVA test was statistically significant, indicating that MESA-UI scores improved from baseline to 3 months, then stayed improved at 6 months; F(2, 54) = 24.09, p < 0.001 (Table 2). Moreover, from baseline to 6 months, 66% of patients had a score improvement of at least 3 units, indicating a clinically meaningful improvement.
The FsFI final instrument ranged with scores from 1 to 36, with a score <26 indicating sexual dysfunction. The ANOVA test was statistically significant, indicating that FsFI scores improved from baseline to 3 months, then stayed improved at 6 months; F(2, 52) = 13.15, p < 0.001. In addition, the 3-month and 6-month mean values were above the 26-value threshold (28.66±8.06 and 27.78±6.92, respectively), indicating that after the treatment, on average, the patients were considered not sexually dysfunctional (Table 2).
Finally, patient UDI-6 scores were captured at four measurement periods. Lower values indicate symptom improvement, with the cutoff value of 33.33 being considered the top of the normal range. Measurements were taken at baseline, 1 month, 3 months, and 6 months. The ANOVA test was statistically significant F(3, 81) = 33.33, p < 0.001. UDI-6 scores decreased from baseline to 1 month, then stayed flat at 3 months and 6 months. However, the 1-month values were significantly lower than the 6-month values, indicating some degradation at 6 months compared with that at 1 month (Table 3). In addition, 82% of patients had a minimum of 10 points of improvement from baseline to 6 months. Table 3 presents the four time period means and corresponding pairwise comparison p-values.
UDI-6 Outcomes Before and After the Three-Treatment Regimen
UDI-6 data from baseline to 6 months.
UDI-6, Urogenital Distress Inventory-6.
Discussion
This study demonstrates the safety, efficacy, and short-term durability of treatment for MUI in women using a combination of patient education, transvaginal bipolar RF energy with the FormaV device, and EMS pelvic floor rehabilitation with vTone. Following a series of three treatments, each administered 2 weeks apart, clinically and statistically significant improvements from participants’ pre-treatment baseline were seen at 3 and 6 months post treatment for in pad weight, CST, and various validated measures of UI and associated quality of life, including the UDI-6, iQOL, MESA-SI, and MESA-UI questionnaires. Overall, the symptom improvements from baseline that was appreciated at 3 months remained stable at the 6-month point, with the slight upward trend of the UDI-6 over time between intervals not statistically significant.
In addition to being asked to describe their symptom burden, study participants were asked to quantify the financial value of these treatments to them—that is, what they would be willing to pay to receive them. This is an important question, because novel technologies like bipolar RF are not typically covered by any health insurance plans, and many plans provide little-to-no coverage for EMS and other physical therapy interventions. Participants indicated a willingness to pay between $250 and $500 per treatment session throughout the study, for a hypothetical anticipated cost of treatment totaling $700–$1500 over 6 weeks. This outcome compares favorably with the potential financial costs of pelvic physical therapy, certain overactive bladder medications, and/or surgery. Also, the authors feel there are significant advantages to providing multiple therapies at the same location by the provider who understands the condition being treated as well as the patient’s expectations.
The combination of bipolar RF and EMS was well tolerated without adverse events, allowing for patients to return to their day-to-day activities without requiring downtime for recovery.
This pilot study has several significant limitations. Some of these are structural: its small size and the absence of any control group or blinding limit the conclusions that can be drawn. We also have very limited data regarding the comorbidities of the participants—while significant medical problems precluded participation in the study, there are various relatively minor conditions (e.g., hair loss, hypertension) and treatments (e.g., diuretic medication) that were not among the exclusion criteria and are known to aggravate lower urinary tract symptoms and incontinence. It is uncertain to what extent these or other factors might have contributed to the case of the2/31 study participants who reported worsening of their symptom burden on the PGI at 3 and 6 months.
Very few studies to date have evaluated the use of more than one intervention to treat stress, urge, or mixed incontinence. A significant potential advantage of this study is that it utilized patient education and pelvic floor rehab in addition to RF therapy. Preliminary data on this treatment regimen seem to indicate that it can successfully address incontinence in a very safe and minimally invasive fashion.
Further study is needed to better characterize the patient population with MUI that is likely to benefit from transvaginal bipolar RF and EMS, and to determine the durability of symptomatic improvement achieved by the studied regimen of three treatment sessions administered bimonthly. It is possible that a different pattern of administration, whether a change in the frequency and/or number of treatments administered, might optimize their beneficial effect. Additional study is also indicated to determine whether the combination of FormaV with vTone treatment is essential, or if similar symptom improvements might be achieved by either intervention alone, with associated savings of time and money for the patient.
Conclusions
This is the first study, to the best of our knowledge, to report the use of FormaV RF and vTone EMS treatment in the vaginal canal. Preliminary data would seem to indicate that such intervention in addition to patient education can result in improvement of MUI symptoms. In addition to symptomology improvement, this treatment protocol may improve women sexual health. This procedure has a high patient satisfaction and improvement in quality of life.
Footnotes
Acknowledgments
The data were analyzed by statistician, J.J. De Simone who was provided with raw data from InMode.
Authors’ Contributions
Dr. Mickey Karram acted in conceptualization and methodology, resource and funding acquisition, project administration, investigation, supervision, validation, and writing. Drs. Rodger Rothenberger and Lanna Cheuck acted in data curation, investigation, and writing. Drs. Tracy Blusewicz and Yanilis Diaz acted in project administration, investigation, supervision, validation, and writing.
Author Disclosure Statement
Dr. Lanna Cheuck has accepted paid travel expenses/honoraria from GAIN/Galderma and holds a position of influence in InMode. Dr. Tracy Blusewicz has received shares from InMode. Dr. Mickey Karram has accepted paid travel expenses/honoraria and is a consultant for InMode. Drs. Rodger Rothenberger and Yanilis Diaz have no conflicts of interest.
Funding Information
This study was funded by InMode (Lake Forest, CA).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.