
Abstract
Background:
The introduction of vaginal natural orifice transluminal endoscopic surgery (vNOTES) to the toolbox of gynecologic surgeons has the potential to reverse the trend of vaginal hysterectomy declines.
Methods:
This review discusses nuances of the vNOTES technique applied to hysterectomy; describes vNOTES hysterectomy, step-by-step (including tips and tricks for low- and high-complexity cases for surgeons who may want to incorporate vNOTES hysterectomy into their surgical repertoires); and examines evidence and research trends in this field.
Results:
The descriptions in the text, figures, tables, and videos all contribute to giving readers a clear understanding of vNOTES, its advantages, limitations, and research potentials.
Conclusions:
vNOTES hysterectomy is a unique blend of vaginal, laparoscopic, and laparoendoscopic single-site surgery (LESS) techniques and is not a new procedure, but rather another tool to use in minimally invasive gynecologic surgery. (J GYNECOL SURG 40:78)
Introduction
Before the emergence of laparoscopy, when open abdominal and vaginal hysterectomies were the only options, a large proportion of hysterectomies had the potential to be done vaginally. However, multiple barriers prevented widespread use of the vaginal route.1,2 The history of the vaginal natural orifice transluminal endoscopic surgery (vNOTES) evolution is tied closely to transabdominal laparoendoscopic single-site surgery (LESS), 3 which emerged as an alternative to popular multiport laparoscopy and robotics. However, the challenges of transabdominal LESS halted its widespread adoption, 4 and vNOTES emerged in the last decade as a way to revive vaginal surgery, which has been declining at a rapid rate, while laparoscopy and robotics gained acceptance.
This expert review (1) discusses nuances of the vNOTES technique as it applies to hysterectomy; (2) describes vNOTES hysterectomy, step-by-step, including tips and tricks for low- and high-complexity cases for surgeons who may want to incorporate vNOTES hysterectomy into their surgical repertoires; and (3) examines evidence and research trends in this field.
Patient Selection
Indications and contraindications to vNOTES hysterectomy as well as considerations for preoperative planning are listed in Table 1.5,6 While it is beyond the scope of this article to address the use of the vNOTES route for endometriosis, exploration of this route continues; however, the surgical community is not yet ready for wide adoption of this technique. 7
Patient Selection for Vaginal Natural Orifice Transluminal Endoscopic Surgery Hysterectomy
vNOTES, vaginal natural orifice transluminal endoscopic surgery; MRI, magnetic resonance imaging; US, ultrasound; PID, pelvic inflammatory disease; AUB, abnormal uterine bleeding; C-section, cesarean section.
The ideal candidate for low-complexity vNOTES hysterectomy is a patient with abnormal uterine bleeding with or without fibroids. There is no “size” cutoff as long as the physical examination and imaging are consistent with the above description. Uterine weight over 1 kg is commonplace and vNOTES hysterectomy over 3 kg has been documented.8–10 Adenomyosis is also often addressed via vNOTES hysterectomy; however, the possibility of coexisting endometriosis needs to be considered due to its high prevalence in this patient population. Surgical teams must have close collaborative relationships with radiologists and sonologists. 11
The “bottom-up” approach to anatomy and pathology offers several advantages. The surgeon controls the uterine blood supply at the beginning of the case, not at the end of it. 5 Bladder and ureters are mobilized early in the case, not later. While the incidence of bladder and ureteral injuries varies widely, as it depends on patient selection, practice setting, and surgeon skill set, this could explain why ureteral injuries have been less common in the vaginal compared to the transabdominal minimally invasive gynecologic surgery (MIGS) approach in some studies.12,13
In addition, the bottom-up approach is advantageous in cases requiring cesarian section scar adhesiolysis or cases of large fibroid burden (Videos 1 and 2).14,15 Larger studies and systematic reviews have shown that the vaginal route is most favorable in terms of reducing complications.16,17 Among surgeons with the highest level of skill (fellowship training and high volume) limited to a specific route, the risk of urinary-tract injury during a hysterectomy drops from 1% to 0.04%. 18 This highlights the urgent need for research on high-quality gynecologic surgical outcomes focused on nuanced patient- and surgeon-specific factors.
For obese patients, vNOTES, just like conventional vaginal hysterectomy, offers several advantages in comparison to the transabdominal route (Fig. 1).
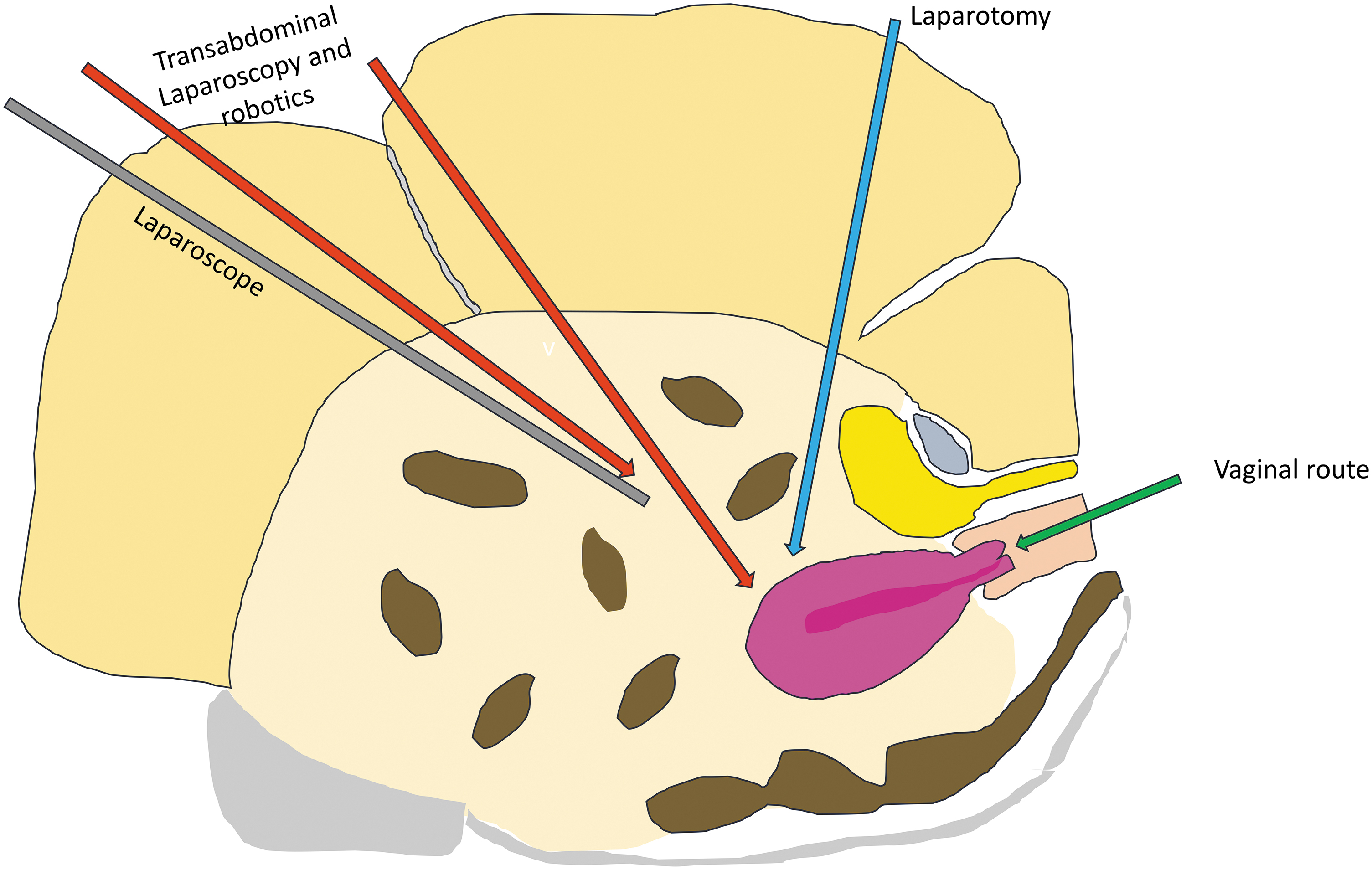
Vaginal natural orifice transluminal endoscopic surgery approach to hysterectomy in comparison to transabdominal laparoscopy and robotics in obese patients. Color images are available online.
The decision-making process of a surgeon who opts to keep or add a vaginal approach to the surgical repertoire differs from that of a surgeon limited to the transabdominal laparoscopic or robotic route. First, a vNOTES surgeon must go through the preoperative evaluation required during patient selection to triage the patient to the appropriate route. Second, a vNOTES surgeon needs to have a lower threshold for a higher conversion rate to laparoscopy, compared to a surgeon whose only route is a transabdominal route, when conversion means a laparotomy. In general, all surgeons will have a conversion rate that depends on their skill set, pathology, patient factors, and resources in the surgeon's local practice settings. All surgeons strive to minimize that rate, as conversions prolong operating room time and increase complication rates. However, when a vaginal route is converted to a transabdominal laparoscopic or robotic route, this conversion remains within the minimally invasive realm.
When discussing the vaginal versus the transabdominal MIGS approach with patients, it is important to explain the benefits of avoiding the transabdominal route: less pain and no abdominal incisions; avoidance of the risk of injury at the time of laparoscopic entry; avoidance of nerve injury and nerve entrapment; and avoidance of incisional hernias (in case of minilaparotomy when transabdominal tissue extraction is utilized).
Other factors, such as patient and surgeon preferences, surgeon skill, learning curves, teaching trainees, implementation in different practice settings, and adoption rates are beyond the scope of this review.
vNOTES Hysterectomy Surgical Technique
Learning the technique of vNOTES hysterectomy requires adoption of LESS techniques while continuing to utilize the conventional vaginal surgery skill set. Tables 2 and 3, Figures 2 and 3, and Videos 1–8 describe vNOTES hysterectomy steps and techniques in detail. Preparation, setup, and instrumentation were described in a 2022 article. 1 It is beyond the scope of this review to cover the vaginal portion of this procedure for novice surgeons. Numerous resources (textbooks, articles, surgical videos) are available on this topic if more indepth understanding is desired.19,20
Comparison of multiport, transabdominal laparoendoscopic single-site surgery (LESS) and vaginal natural orifice transluminal endoscopic surgery (vNOTES) techniques.
Optimizing working space by minimizing external collisions.
Vaginal Natural Orifice Transluminal Endoscopic Surgery (vNOTES) techniques applied to vNOTES hysterectomy
Based on these characteristics, the most commonly used device is the 5 mm LigaSure™ Blunt Tip (Medtronic, Dublin, Ireland). A LigaSure (Maryland, USA & Medtronic) tip can also be used in cases of extensive C-section scar adhesions due to its shape. Applied Medical (Rancho Santa Margarita, CA, USA) manufactures the Voyant® Intelligent Energy System, a popular advanced bipolar energy device in settings where it is available due to its ability to articulate without restriction. Any of the ultrasonic devices (HarmonicACE™ [Ethicon, Raritan, NJ, USA], the Thunderbeat® [Olympus, Center Valley, PA, USA], the Sonocision™ [Medtronic]) are not suitable options, as they need to be activated off the tension, are not designed for grasping & take longer to cool. The Enseal™ (Ethicon) device has a wider jaw that does not seem to work as well in LESS surgery due to space restriction.
LESS, laparoendoscopic single-site surgery; vNOTES: vaginal natural orifice transluminal endoscopic surgery; FOV, field of view; C-section, cesarean section.
Vaginal Natural Orifice Transluminal Endoscopic Surgery: Hysterectomy Step-by-Step with Tips and Tricks.
Self-assembled vaginal LESS ports made of any small wound retractor, glove & ports can be used off-label in settings where a GelPOINT V-Path Transvaginal Access Platform is not available. Self-assembled vaginal LESS ports and use are beyond the scope of this article.
LESS, laparoendoscopic single-site surgery; vNOTES: vaginal natural orifice transluminal endoscopic surgery.
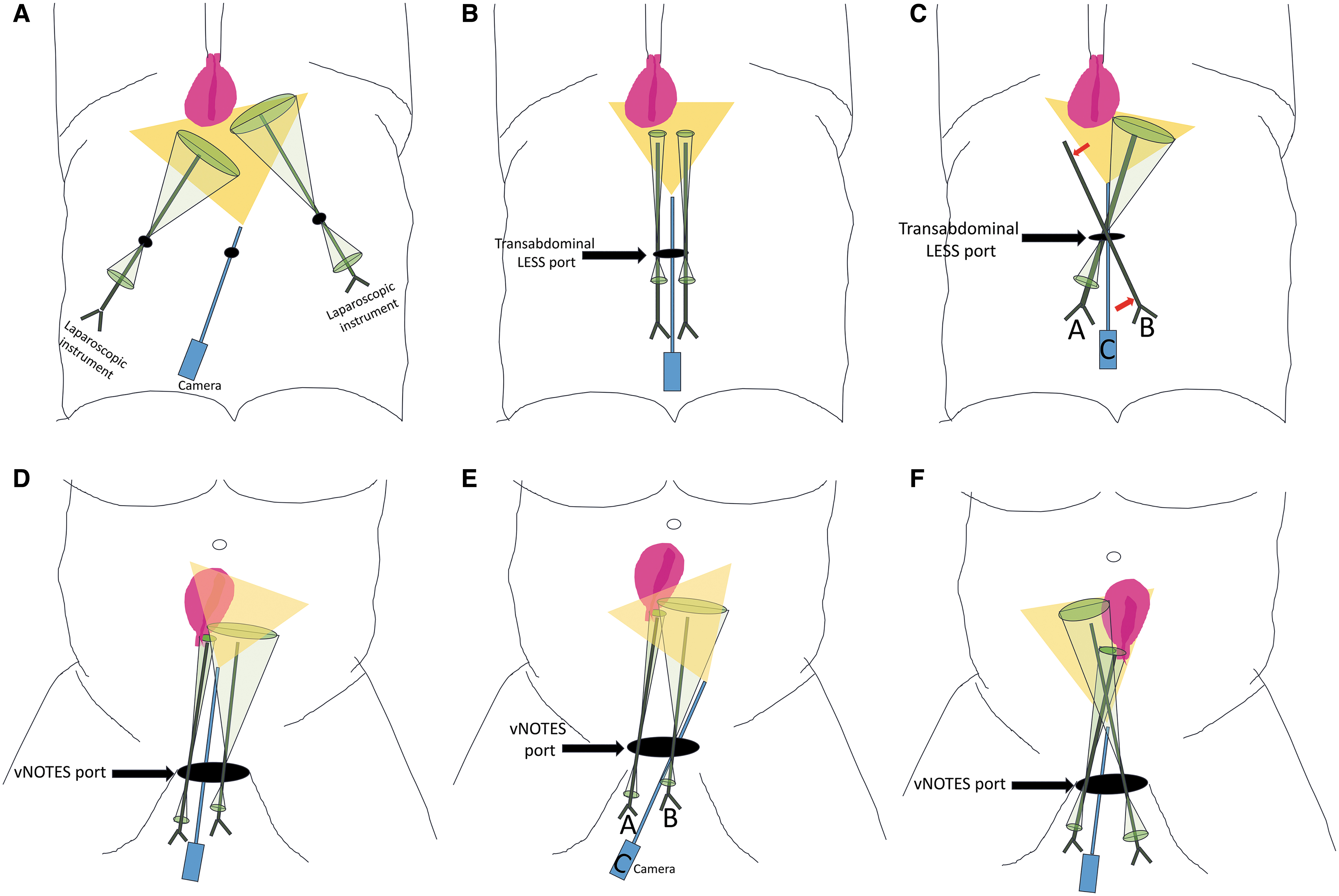
One challenge of any LESS procedure, including vNOTES, is restricted movements and their sequelae, such as loss of triangulation and limited visualization. While multiport laparoscopic and robotic surgeons are used to manage movement restriction resulting from an instrument confined to a transabdominal port, LESS surgery, including vNOTES, results in unique movement restriction because all instruments are confined to the same port. (Fig. 2A–C).
A nuance specific to vNOTES hysterectomy is that the LESS incision in vNOTES is the vaginal colpotomy. By default, the vaginal colpotomy is going to be a larger, more-flexible, and less rigid incision than the most commonly utilized 2–3 cm transabdominal incision (Fig. 2D–F). Another consideration in vNOTES hysterectomy is that, at the beginning of the case, the inner ring is bent in a narrower configuration, but, as the surgeon transects cardinal ligaments and moves cephalad along the broad ligament, the inner ring opens and unfolds, and restriction is reduced. Yet, as the surgeon moves cephalad along the broad ligament from the distal to the proximal portion of the pelvis, the surgeon moves farther and farther away from the inner ring. Thus, movements become more restrictive again.
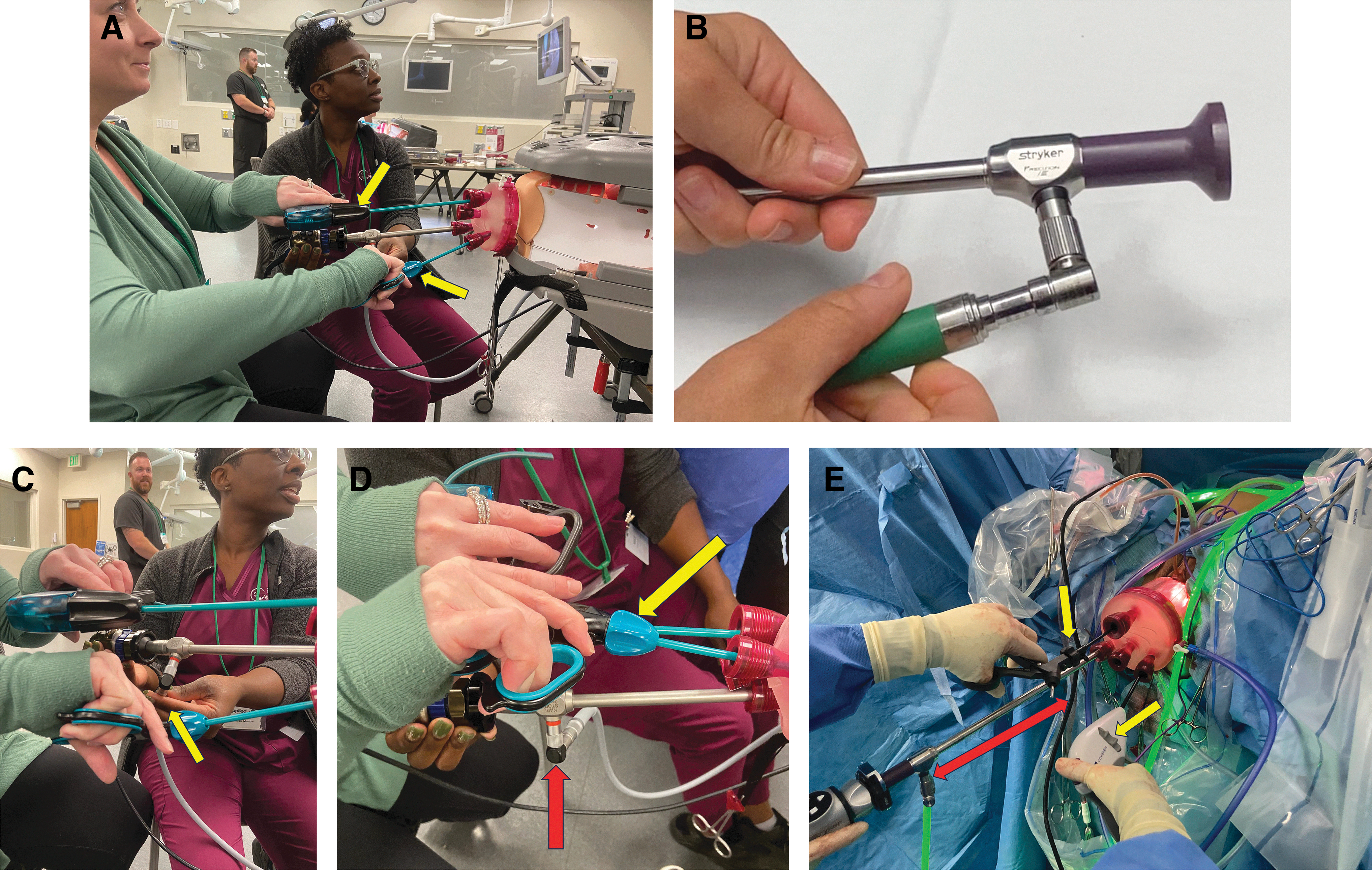
Another challenge in LESS surgery in general (including vNOTES) is internal and external instrument collisions and crowding. In vNOTES, to minimize external collisions, one option is to orient the surgeon's hands horizontally rather than vertically which, in turn, requires using articulating instruments (Fig. 3 A, C–E). In addition, using a right-angle light adapter moves the light cord out of the way (Fig. 3B). Yet another is to option is to stagger instruments by using a bariatric length scope and a bariatric length bipolar device (Fig. 3E).
As with transabdominal LESS, the surgeon has 2 options in vNOTES instrument maneuvering: (1) a parallel technique or (2) a cross technique (Fig. 2D–F).21,22 When working in parallel, 2 instruments move conventionally as they would in multiport transabdominal laparoscopy; however, when working space is limited, this technique may result also in instrument crowding, and internal and external collisions. Working space in LESS is thought of as an ellipse and its shape is determined by the camera degree, the distance between instruments and the camera, and the length of the instruments. For example, in LESS, if all instruments point to the same target, and do not cross each other with the use of a 0° laparoscope, all instruments are parallel to each other, and the range of movement is limited (Fig. 2B). However, using a 30° lens leads to a laparoscope crossing with the instruments. Furthermore, keeping 1 instrument static for tissue traction provides more space for movement of the second instrument; static and dynamic instruments are alternated as needed (Fig. 2C).
As in LESS, in vNOTES, using a 30° lens expands the view; while few surgeons prefer to use a 0° laparoscope, as it requires less skill to operate, most prefer the advantages of a 30° scope (Fig. 2B, 2D–F). Of note, using a flexible scope has been tried in vNOTES and has not been found useful for addressing this limitation. 5
Despite the surgical techniques described above, movement restriction remains a challenge for higher-complexity vNOTES cases. For example, procedures that require extensive sidewall dissection (endometriosis, lymph nodes) or suturing (myomectomy) are performed by few surgeons.7,23–33 Movement restriction results in a decreased ability to triangulate, which requires surgeons to cross instruments and manage image reversal. Several robotic platforms are being explored to address this limitation.7,23–29
Finally, smoke evacuation can affect visualization. In conventional, transabdominal, multiport laparoscopic and robotic surgery, tubing that insufflates the abdomen is typically attached to one of the lateral ports, and tubing that is used for smoke evacuation is attached to another port (usually as far away from the insufflation port as possible and away from the camera port). In any LESS surgery, insufflation and smoke evaluation ports are located in close vicinity (in the gel cap). Those challenges tend to be less problematic in vNOTES in comparison to transabdominal LESS surgery, as smoke tends to partially float cephalad out of the pelvis, away from the surgical field. 5
In cases when the uterus cannot be removed intact, conventional volume-reduction techniques (coring and wedging) and ExCITE (extracorporeal C-incision tissue extraction) techniques can be utilized or contained in-bag tissue extraction is performed if indicated or desired.34–40 In vNOTES, unlike in conventional vaginal hysterectomy, all blood supply is secured as the uterus can be rotated easily in the pelvis in cases of patients with enlarged uteri before specimen removal (Video 1).
In addition to conserving costly human resources, retraction provided by the vNOTES port has the potential to reduce ergonomic strain on both the primary surgeon and the 2 assistants.41–44 Studies need to compare surgeon ergonomics between the different routes.
Postoperative Care
vNOTES hysterectomies are ideal candidates for SDS (same day surgery) in ambulatory surgical centers with aggressive use of enhanced-recovery pathways. 45 In comparison to the transabdominal laparoscopic approach, avoiding abdominal ports helps decrease postoperative pain. In comparison to the vaginal route, patients are exposed to pneumoperitoneum; however, it is easier to evacuate the gas at the end of the procedure due to the larger aperture of the vNOTES port. Furthermore, avoidance of metal vaginal retractors, and difference in handling of the pedicles (clamping, cutting, and tying versus using advanced bipolar devices) could potentially explain why patients who undergo vNOTES might experience less pain, compared to patients who undergo conventional vaginal hysterectomy. Unfortunately, studies on this topic do not address questions about postoperative pain adequately, as that metric is not the primary endpoint of most studies. As a result, some vNOTES studies show lower pain scores, 46 while others do not 47 ; a systematic review and meta-analysis comparing vNOTES to laparoscopic hysterectomy published in 2020 showed no difference in pain scores after vNOTES hysterectomy. 48
Finally, this topic is difficult to study as ERAS (enhanced recovery after surgery) protocols involve many components and vary widely from institution to institution. Based on clinical experience alone, many vNOTES surgeons note a decrease in pain scores after vNOTES hysterectomy in comparison to other routes and adjust their ERAS protocols and preoperative counseling accordingly.
What We Know So Far—the Evidence-Based vNOTES Hysterectomy
The concept of transvaginal endoscopic surgery is not new—it was explored by Semm in the 1960s. Unfortunately, at that time, laparoscopic equipment such as cameras, instruments, and light sources were not adequate to develop the technique. Three decades later, transvaginal hydrolaparoscopy was developed as a diagnostic procedure and is considered a precursor for vNOTES. 49 In the 2000s, vaginal natural orifice surgery was first reported in general surgery for cholecystectomy and appendectomy.50,51 A decade later, surgeon–innovators published their work on vNOTES hysterectomy. MIGS surgeons in Taiwan, under the leadership of Chyi-Long Lee, shared their experience by publishing the first feasibility study describing NOTES hysterectomies, utilizing a self-made port made of a glove and a small wound retractor. 52
At the same time, Jan Baekelandt in Belgium utilized a similar technique and became not only a vNOTES pioneer in the Western world 53 but also a surgeon–scientist whose team researched and published extensively during that early innovation and later development phases following the principles of the IDEAL guidelines. 54 He and his team first documented complication rates in vNOTES hysterectomies in a large series 8 that spanned 5 years during this early adoption phase (2013–2018) involving 1000 vNOTES surgery patients, of which 73% were hysterectomies. The team noted a 5.2% complication rate (1.4% intraoperative and 3.8% postoperative). Most of the intraoperative complications involved cystotomies (9 cases; 1.2%). The mean specimen weight was 172 g (range: 20–3361 g), and the average operating time was 46 minutes (range: 20–250 minutes).
While descriptive studies are a great starting point for understanding innovation and setting the stage for future research, ultimately, randomized controlled trials (RCTs) are needed to understand how to utilize new approaches in a way that would benefit patients. There are multiple challenges to conducting high-quality research in MIGS, one of which is low complication rates.
Keeping that in mind, Baekeland and colleagues conducted a noninferiority RCT comparing vNOTES to the transabdominal laparoscopic approach for benign hysterectomy patients powered for conversions from vNOTES route, HALON (hysterectomy by transabdominal laparoscopy or natural orifice transluminal endoscopic surgery). The authors randomized 70 patients to vNOTES hysterectomy with sham skin incisions or laparoscopic hysterectomy (ClinicalTrials.gov NCT02631837). 47 The researchers concluded that vNOTES hysterectomy was noninferior to laparoscopic hysterectomy because neither group had any conversions; however, when looking at secondary outcomes, the vNOTES arm had a shorter length of stay and left the hospital earlier. Postoperative complication rates did not differ between the groups.
A systematic review and meta-analysis comparing vNOTES to laparoscopic hysterectomy published in 2020 included the RCT described above and 5 retrospective studies. 48 The researchers found that vNOTES had shorter operative times and lengths of stay, and lower estimated blood losses, with no differences in complications, readmissions, and pain scores. As utilization of vNOTES hysterectomy increased, surgical repertoires expanded to higher-complexity cases, a trend reflected in publications.
Several retrospective studies described the use of vNOTES hysterectomies in different settings, all with similar favorable safety profiles: a retrospective review of large uteri with a mean weight of 559 ± 425 g (range: 281–3361g) 55 ; uteri >1 kg 10 ; obesity56,57; virginal patients 9 ; and gender-affirming hysterectomy. 58 A vaginal NOTES hysterectomy has been described wherein the entire procedure was completed laparoscopically and could be explored further in cases when the vaginal portion is the most challenging. 53 A large international multicenter RCT is currently underway to compare vNOTES, conventional vaginal, and laparoscopic hysterectomies (the VANOLAH trial; ClinicalTrials.gov NCT05971875).
Tracking vNOTES cases in the United States is problematic because no Current Procedural Terminology code exists for vNOTES. Most surgeons use laparoscopically assisted vaginal hysterectomy codes for vNOTES hysterectomy when billing, which complicates tracking. The International NOTES Society has a voluntary case registry, but these data are not available for public use. 59
Future studies are needed to understand the cost of vNOTES hysterectomies, compared to other routes, patient preferences, surgeon factors, training, implementation, and adoption factors.
Conclusions
vNOTES is not a new surgical technique or tool, but rather a new surgical approach that combines and modifies several existing techniques. The current authors hope that it will allow us to expand the range of surgical repertoire in MIGS, which, in turn, will benefit patients.
Footnotes
Author's Contributions
Drs. Lerner and Baekalandt conceptualized this project, and Drs. Baekalandt and Stuart supervised it. All 3 authors visualized it, while Dr. Lerner was responsible for administration and worked with Dr. Baekalandt on the methodology. Dr. Lerner managed resources and software and curated the data. All 3 authors conducted the investigation and the formal analysis. Drs. Lerner and Baekalandt wrote the original draft of this article, and all 3 authors reviewed and edited it.
Author Disclosure Statement
Dr. Lerner is a paid consultant to Applied Medical (Rancho Santa Margarita, CA, USA) and Cooper Surgical (Trumbull, CT, USA). Dr. Stuart is a paid consultant to Applied Medical. Dr. Baekalandt is a paid consultant to Applied Medical and Momentis Surgical (Fort Lauderdale, Florida).
Funding Information
No funding was provided for this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.