
Abstract
Objective:
The goal of this research was to investigate the feasibility, safety, and short-term clinical outcome of pure extraperitoneal sacrocolpopexy with transvaginal natural orifice transluminal endoscopic surgery (V-NOTES) for treating central pelvic defects.
Material and Methods:
A total of 9 patients with central pelvic prolapse underwent extraperitoneal sacrocolpopexy with V-NOTES, at the Chengdu Women's and Children's Central Hospital, Chengdu, Sichuan, China, between December 2020 and June 2022. The patients' demographic characteristics, perioperative parameters, and clinical outcomes were analyzed retrospectively. Each patient had the following major surgical procedures: (1) Establishing a platform for an extraperitoneal approach with V-NOTES; (2) separating the extraperitoneal path to the sacral promontory region; (3) suturing the long arm of the mesh to the anterior longitudinal ligament S1; and (4) suturing and fixating the short arm of the mesh at the top of the vagina.
Results:
The median patient age was 55, the median operative time was 145 minutes, and the median intraoperative blood loss was 150 mL. The operations were successful for all 9 cases, with a median preoperative Pelvic Organ Prolapse–Quantification score of C: +4, and a 3-months postoperative score of C: −6. There were no recurrences during a follow-up of 3–11 months, and no complications occurred, such as mesh erosion, exposure, and infection.
Conclusion:
As a new surgical approach, extraperitoneal sacrocolpopexy with V-NOTES is safe and feasible. (J GYNECOL SURG 39:108)
Introduction
Pelvic organ prolapse (POP) is a common disease among middle-age and older women, while sacrocolpopexy is still considered as the gold standard procedure for apical prolapse. Surgical approaches include abdominal sacrocolpopexy (ASC), laparoscopic sacrocolpopexy (LSC), robot-assisted laparoscopic sacrocolpopexy, and transvaginal natural orifice transluminal endoscopic surgery (V−NOTES) sacrocolpopexy. 1 No matter which surgical approach is adopted—whether or not it is robot-assisted, 2 —during the procedure, mesh access from the vaginal cuff level to the first sacral vertebra (S-1) anterior longitudinal ligament is created by opening the peritoneum under the pneumoperitoneum in the abdominal cavity and separating the surrounding tissues. 3 For the extraperitoneal approach, it is not necessary to enter the abdominal cavity, and, thus, interference of obesity may be avoided, the surgical field may be exposed fully, and relevant complications may be reduced. A new pure extraperitoneal approach for sacrocolpopexy with V-NOTES was tried, and this approach was safe and feasible for treating central pelvic prolapse.
Materials and Methods
Patients
A total of 9 patients with central pelvic prolapse underwent extraperitoneal sacrocolpopexy with V-NOTES at the Chengdu Women's and Children's Central Hospital, in Chengdu, Sichuan, China, between December 2020 and June 2022. Before the study, all of these patients signed informed consent forms.
Surgical procedure
Each patient was given cephalosporin antibiotics to prevent infection 30 minutes prior to surgery. Under general anesthesia, the patient was placed in a lithotomy position and indwelling urethral catheter was placed in her bladder. The posterior fornix of the patient's vagina was incised transversely without opening the peritoneum. Then blunt dissection was performed to create a separation in the right pararectal space. A 24-Fr double-lumen balloon urinary catheter was place in that space after the blunt separation, 60 mL of water was injected into the balloon, and an extraperitoneal space was established initially by dilating the balloon. A laparoscopic instrument for V-NOTES was then placed in the extraperitoneal space (Fig. 1). The extraperitoneal space was separated under the pneumoperitoneum to the sacral promontory. (Fig. 2). After mesh access was established, the long arm of a Y-shaped tension-free mesh was sutured on the anterior longitudinal ligament of S-1 (Fig. 3).
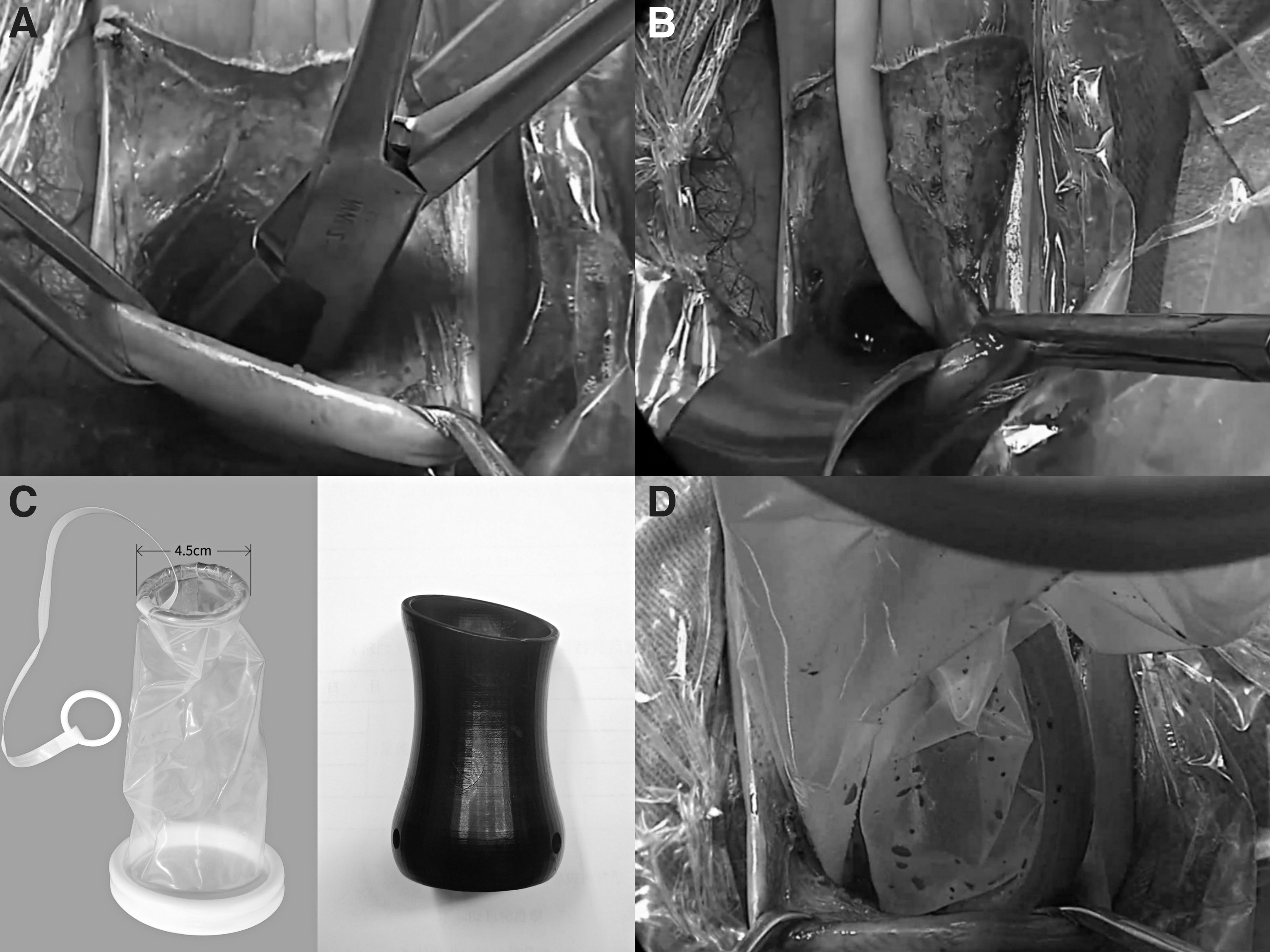
Establishing a platform for an extraperitoneal approach.
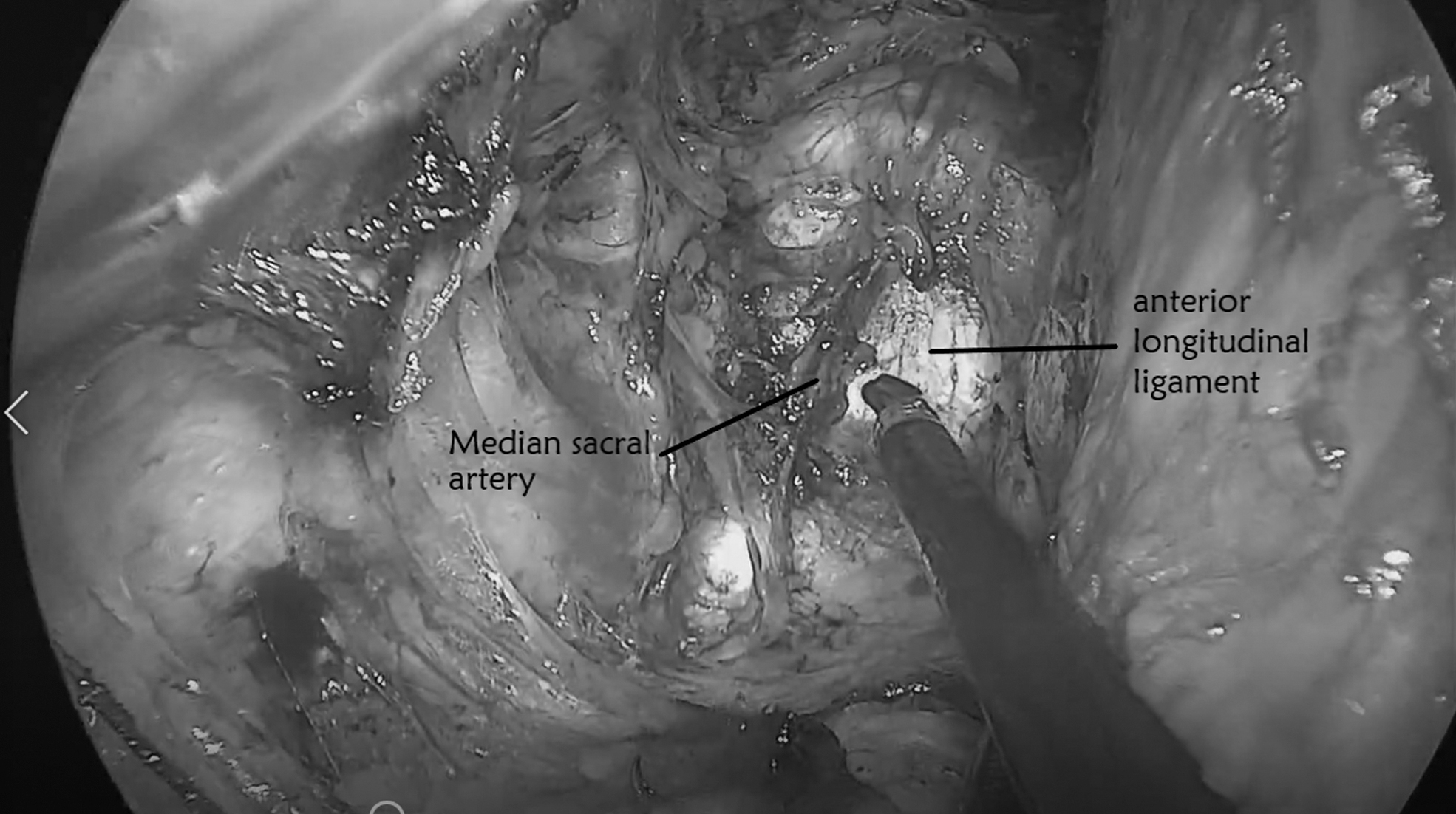
The sacral promontory region in the extraperitoneal space.
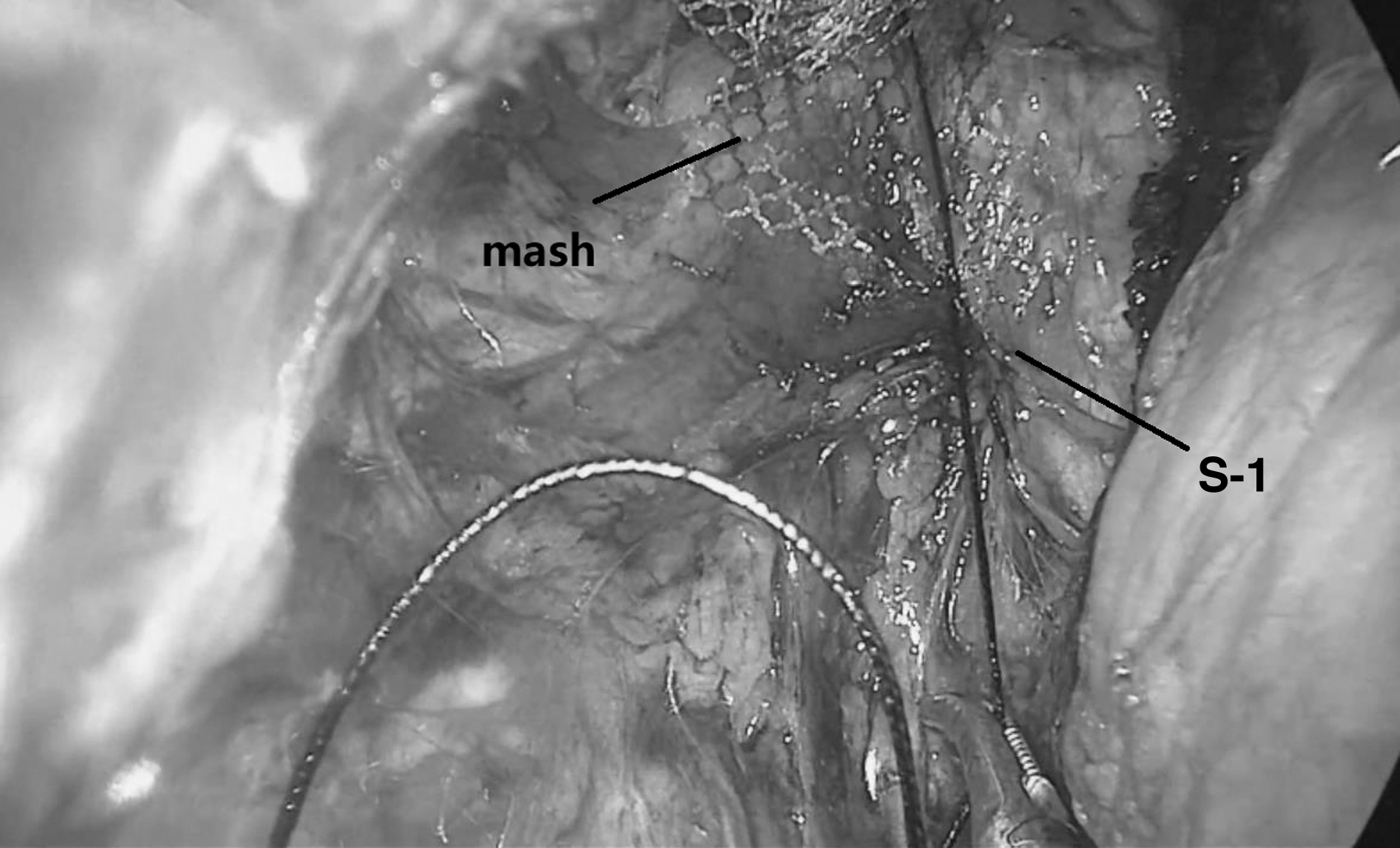
Suturing the long arm of the Y-shaped mesh in the extraperitoneal space.
A routine hysterectomy and bilateral salpingectomy were performed. The vaginal–vesical space and rectovaginal spaces were separated, to expose enough of the prolapsed areas among the anterior and posterior vaginal walls. The mesh was removed. The length of the prolapse of the anterior and posterior walls of the vagina were measured and the mesh was cut to fit these areas. The distal end of the mesh was first sutured to the distal end of the prolapsed vagina and then sutured to the proximal end of the prolapsed vagina, in turn, to ensure that this mesh had sufficient width and length. The junction of this mesh was located at the peak of the vagina (Fig. 4), and the entire mesh was located extraperitoneally. Gauze was inserted into the vagina, to prevent sticking between the vaginal wall and the mesh. Vaginal surgery and endoscopic procedures are shown in Figures 1, 2, 3, and 4 and in Supplementary Video 1 (Supplementary Data are available online at: www.liebertonline.com/GYN). The gauze in the vagina was removed 48 hours post surgery. Forty-eight hours of preventive antibiotics were given post surgery.
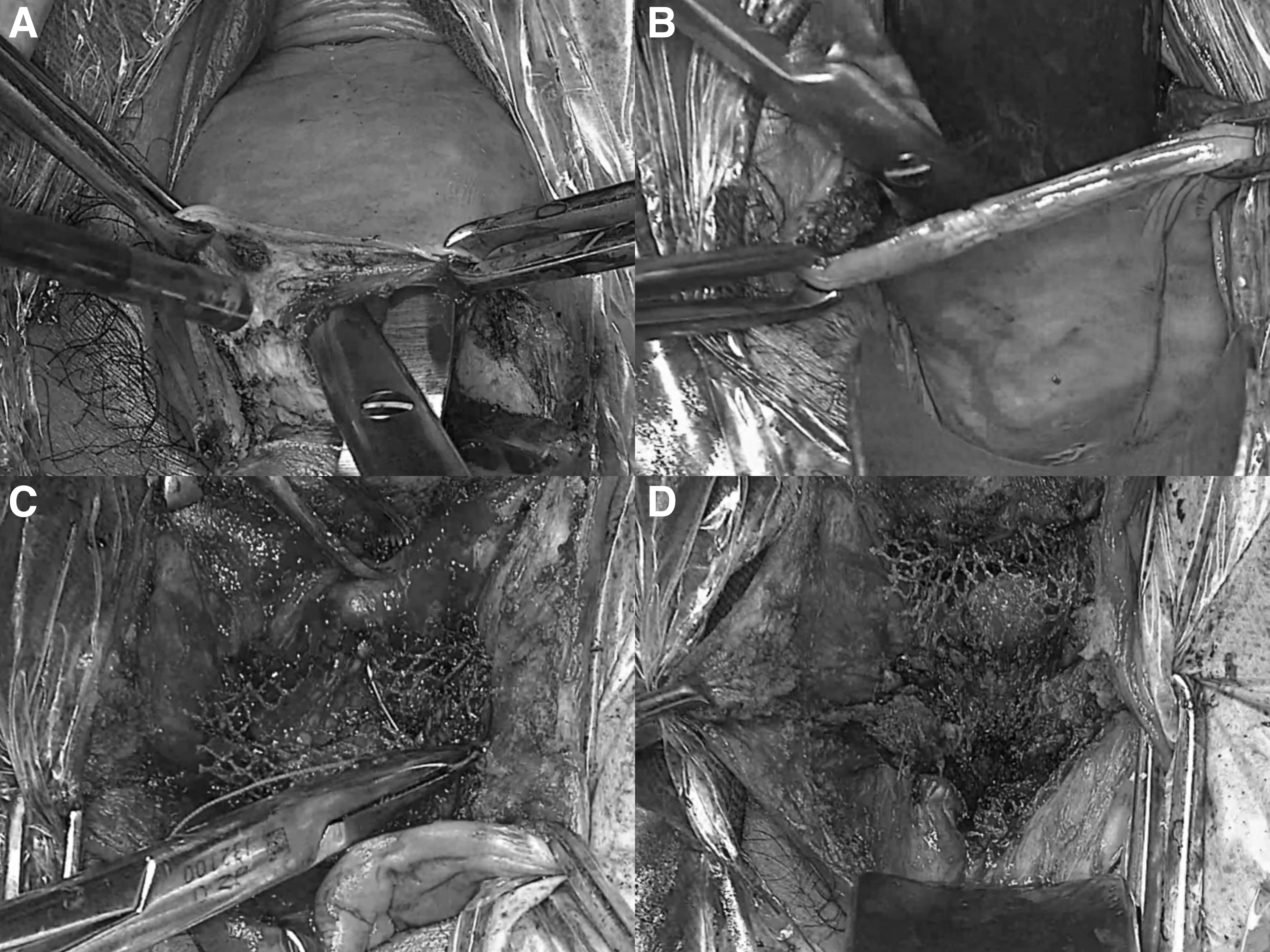
Mesh fixation at vaginal cuff.
Results
Nine patients were studied, and the extraperitoneal approach was successful in all cases. The median patient age was 55; body mass index (BMI), 23.5 kg/m2; operative time, 145 minutes, and intraoperative blood loss, 150 mL. Two patients had bleeding from the anterior sacral-branch vein; this bleeding was stopped by electrocoagulation. No massive bleeding occurred during or after surgery. The median postoperative hospitalization lasted 4 days (Table 1).
Clinical Characteristics and Perioperative Parameters of the Study Patients
yrs, years; BMI, body mass index; min, minutes; d, days.
No complications occurred during or after the procedures, and associated symptoms disappeared or were reduced significantly after surgery. The median preoperative Pelvic Organ Prolapse–Quantification (POP-Q) score was C: +4, and at 3 months postoperatively, it was C: −6. There were no recurrences during the follow-up of 3–11 months.
Within 3–11 months of postoperative follow-up, relevant symptoms were resolved, there were no discomfort in the each patient's sexual life with no pain during intercourse, and there were no complications such as mesh erosion, exposure, and infection (Table 2).
Clinical outcomes in This Study
POP-Q, Pelvic Organ Prolapse–Quantification (score); mos, month(s).
Discussion
The surgical approach with V-NOTES has been widely used in tubal surgery, ovarian cystectomy, hysterectomy, etc. This approach has also been reported frequently used to address pelvic-floor dysfunction conditions. In the transvaginal path for sacrocolpopexy, the pelvic side wall needs to be opened to separate the peritoneum before a mesh pathway is established; then the peritoneum can be sutured and closed, and the mesh placed outside the peritoneum.4,5 There are few cases of totally extraperitoneal approach surgery with V-NOTES without opening the peritoneum.
In 2012, Noblett et al. studied the feasibility of extraperitoneal sacrocolpopexy with V-NOTES, using cadavers. 6 However, the sacrum and its surrounding important structures could not be found, and fixation of mesh to perivaginal structures could not be completed; thus, the extraperitoneal approach was given up. In 2018, Wang and Liang reported a study concerning a series of patients with central pelvic prolapse who underwent extraperitoneal sacrocolpopexy with V-NOTES for the first time, 7 and established extraperitoneal access to the sacral promontory successfully. However, the study failed to detail the procedure for fixing the mesh at the top of the vagina, which is a difficult point for extraperitoneal sacrocolpopexy with V-NOTES.
The current surgical method is a true whole-process extraperitoneal procedure with V-NOTES surgery, with 4 difficult points as follows:
Establishing a platform for extraperitoneal approach with V-NOTES—For the extraperitoneal approach, it is easy to pull the conventional port out of the vaginal orifice repeatedly, thus affecting the operation. A small inner ring for the port was chosen to adapt to the narrow space outside the peritoneum. A patent vaginal-support device was used to strengthen the support and expansion for the vagina, so that the inner ring would not be pulled out repeatedly. Thus, the surgical approach was established successfully. Separating the extraperitoneal path to the sacral promontory region—During extraperitoneal separation, there are few anatomical landmarks for reaching the sacral promontory region, where it is easy for the surgeon to get lost. After repeated attempts, the coccygeus muscle was taken as the first anatomical landmark for the separation along the pelvic side wall toward the cephalic side, with the sacral promontory located at the medial cephalic side. After the sacral promontory was identified, it was found that the direction for bony anatomy changed from ventralward to cephalad. The surgical target area was under the sacral promontory. Suturing the long arm of the mesh to anterior longitudinal ligament S-1—The extraperitoneal space was narrow; thus the suturing was difficult. Various methods were tried, including robot-assisted suturing, and, at last, a common suture technique was found to solve the problem. In the future, rivets need to be used to fix the mesh in the anterior longitudinal ligament to make the operation relatively easy. Suturing and fixating the short arm of the mesh at the top of vagina—Few researchers have described this transvaginal approach in detail. In 2018, Chen described this as follows
8
: First, the mesh was cut and fixed to the posterior vaginal wall; after a routine uterine resection, the long arm of the mesh was sutured and fixed to the sacral promontory; and, finally, a “window” in the lower anterior vaginal wall was created and the anterior mesh was sutured to the descending ramus of the pubis.
In the current series, the distal end of the mesh was sutured to the distal end of the vagina, so it was sutured while it was rolled outwardly. As shown from the schematic diagram in Figure 5, the mesh was sutured to the proximal end of the vagina, in turn, to ensure that the mesh had sufficient width and length. The junction of the mesh was located at the peak of the vagina.
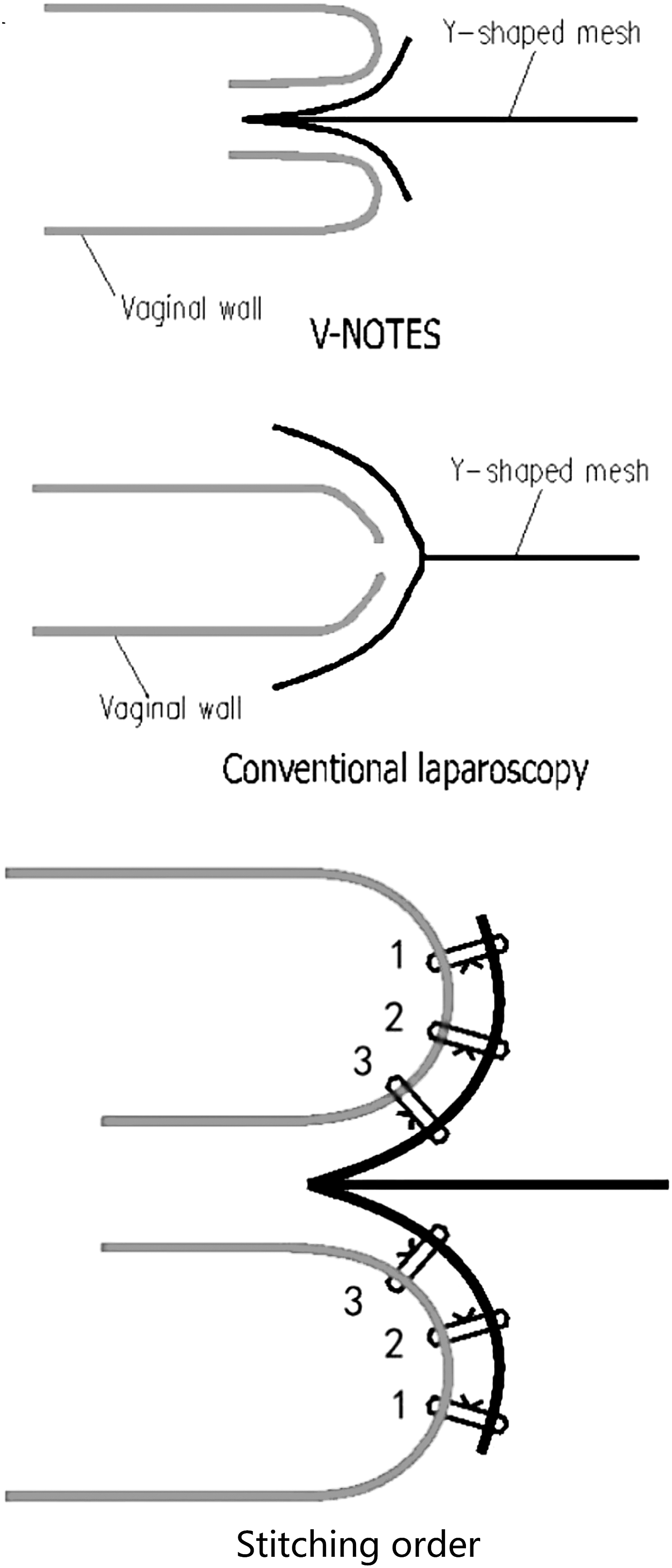
Schematic diagram of sutures. V-NOTES, transvaginal natural orifice transluminal endoscopic surgery.
In this series, there were no surgical failures. There was no intraperitoneal surgery for peritoneal damage, and the median POP-Q score of the C point in the follow-up 3 months after surgery was −6.
In this study, most of the patients had middle pelvic defects. The prolapsed condition of these patients' anterior and posterior vaginal walls were not serious, and prolapse of the upper vaginal segment was caused by cervical prolapse. Pelvic defects were corrected immediately after sacrocolpopexy, and no anterior or posterior vaginal-wall repair was performed. Repair of middle pelvic defects plays an important role in the treatment of pelvic-floor dysfunctional conditions. After corrections of middle pelvic defects, 50% of cases had bulging of the paries anterior vaginase and 30% of cases had bulging of the paries posterior vaginase corrected.9–11
Although the experience of sacrocolpopexy with V-NOTES was limited in this study, this group of physicians was able to complete general gynecologic surgery—and even tumor surgery—skillfully with abundant experience in conventional laparoscopic single-incision surgery and V-NOTES. The surgeons were familiar with pelvic-floor anatomy and skillful in the laparoscopic single-port suture technique, which also contributed to the successful operations. In the future, rivets can be used to fix the long arm of the mesh so that this operation may become relatively easy.
With the extraperitoneal approach, the whole-process procedure outside the peritoneum, was not restricted by obesity, abdominal adhesion, occlusion of bowel position, and other surgical obstacles. This is beneficial for postoperative pain relief and is also based on the principle of ERAS [enhanced recovery after surgery].
Conclusions
A true whole-process extraperitoneal procedure for V-NOTES surgery, as a new approach for sacrocolpopexy, is safe and feasible. However, its clinical efficacy is still to be verified by a randomized controlled study with a larger sample size.
Footnotes
Authors' Contributions
All of the authors were responsible for conception and design of the study, patient recruitment, surgery or imaging, data collection, and article preparation.
Drs. Gu, Huang and He contributed equally to this article.
Author Disclosure Statement
No financial conflicts of interest exist.
Funding Information
No funding was received for this research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.