
Abstract
Abstract
Objective:
Laparoscopic surgery has been developed worldwide due to its minimal invasion as well as noninferiority, compared with laparotomy. However, whether or not laparoscopic systematic para-aortic lymphadenectomy for endometrial cancer is feasible and has advantages of various clinical factors, such as a short hospital stay, less blood loss, and faster recovery, compared with open surgery has not yet been clarified. The aim of this study was to compare a laparoscopic procedure with laparotomy for para-aortic lymphadenectomy for patients with endometrial cancer.
Study Design:
This was a retrospective multicenter study of laparoscopic systematic para-aortic lymphadenectomy for endometrial cancer in five institutions.
Materials and Methods:
The current authors conducted a retrospective multicenter study of laparoscopic systematic para-aortic lymphadenectomy for endometrial cancer. The study involved patients from five institutions in Japan between January 2008 and March 2016. Clinical data were compared with those of a laparotomic procedure performed around the same period.
Results:
A total of 54 patients in the laparoscopic group and 99 patients in the laparotomic group were analyzed. In the laparoscopic group, 21 patients had stage IA disease, 19 had stage IB disease, 5 had stage II disease, and 9 had stage III disease. In the laparotomic group, 35 patients had stage IA disease, 19 had stage IB disease, 9 had stage II disease, and 36 had stage III disease. There were no significant differences in characteristics between the groups, including age, body mass index, and histologic type. The mean operative time in the laparoscopic group was 483 ± 102 minutes, while that in the laparotomic group was 481 ± 106 minutes (p = 0.9). The laparoscopic group had less intraoperative blood loss (143 ± 253 versus 988 ± 694 mL; p < 0.01) and shorter hospital stays (8.4 ± 5.7 versus 16.1 ± 8.0 days; p < 0.01). The rates of intraoperative complications were not significantly different between the groups. No cases of ileus occurred in the laparoscopic group. Procedures for 2 of the 54 patients in the laparoscopic group were converted to laparotomy. The number of dissected pelvic lymph nodes (31.8 ± 10.1 versus 39.9 ± 15.9, p < 0.01) and para-aortic lymph nodes (26.2 ± 10.9 versus 31.1 ± 13.2; p = 0.02) were lower in the laparoscopic group than in the laparotomic group. The postoperative minimum level of hemoglobin was higher in the laparoscopic group than in the laparotomic group (10.4 ± 1.1 g/dL versus 9.9 ± 1.4 g/dL; p = 0.02). In contrast, the postoperative maximum level of C-reactive protein was lower in the laparoscopic group than in the laparotomic group (6.3 ± 3.8 mg/dL versus 10.2 ± 4.9 mg/dL; p < 0.01). The recurrence rate was not significantly different between the groups in the above time period (7.4% versus 14.3%; p = 0.2).
Conclusions:
Laparoscopic systematic para-aortic lymphadenectomy is feasible and can be substituted for laparotomic procedures for patients with early stage endometrial cancer.
Introduction
P
According to the National Comprehensive Cancer Network, para-aortic nodal evaluation from the inframesenteric and infrarenal regions may also be utilized for staging of selected high-risk tumors—such as deeply invasive lesions; those with high-grade histology; and tumors with serous carcinoma, clear cell carcinoma, or carcinosarcoma features—in patients undergoing primary surgical management of endometrioid uterine cancer. 12 However, para-aortic lymphadenectomy is conventionally performed via laparotomy with a large skin incision, and the incidence of postoperative ileus is 12.9%–50% among patients receiving para-aortic lymphadenectomy.13,14
The first laparoscopic para-aortic lymphadenectomy was performed in 1992. 15 The main advantages of this minimally invasive approach over conventional laparotomy included a short hospital stay, less blood loss, faster recovery, less pain, less scarring, and a faster return of bowel function with equivalent assessment of lymph-node status. 16 However, whether or not the laparoscopic systematic para-aortic lymphadenectomy for endometrial cancer is feasible and has advantages of various clinical factors—such as a short hospital stay, less blood loss, and faster recovery—compared with open surgery has not yet been clarified.
The current authors conducted a retrospective multicenter study of laparoscopic systematic para-aortic lymphadenectomy for endometrial cancer in five institutions. Clinical data were compared with those of laparotomic procedures performed in the same five institutions.
Materials and Methods
Participants
This was a multi-institutional cohort study of women with endometrial cancer who underwent systematic para-aortic lymphadenectomy via laparoscopy or laparotomy. A retrospective study was performed. The study involved patients from five institutions in Japan between January 2008 and March 2016: Tokyo Medical Center (Meguro-ku, Tokyo, Japan); Osaka Medical College (Takatsuki-city, Osaka, Japan); Tenriyorozu Hospital (Tenri-city, Nara, Japan); Osaka University (Suita-city, Osaka, Japan); and Kyoto University (Kyoto-city, Kyoto, Japan). The collected data, including information concerning the surgical procedures, intra- and postoperative details, as well as follow-up evaluations, were analyzed retrospectively.
The inclusion criteria for laparoscopic para-aortic lymphadenectomy were as follows: (1) tissue-proven endometrioid carcinoma of grade 3, or more than half myometrial invasion noted on preoperative magnetic resonance imaging or from an intraoperative frozen section diagnosis; (2) no regional or distal lymph-node enlargement; and (3) a tumor clinically confined to the uterus (clinical stage I) based on a preoperative evaluation.
The laparoscopic group was compared with a historical cohort of patients with endometrial cancer who had undergone surgical staging through laparotomy during the same time period. All of the patients underwent hysterectomy, bilateral salpingo-oophorectomy, pelvic lymphadenectomy, para-aortic lymphadenectomy, and/or omentectomy by either laparoscopy or laparotomy. Extraperitoneal pelvic and para-aortic lymphadenectomy was performed in all patients. Briefly, systematic pelvic and para-aortic lymphadenectomy, which was not performed for sampling, consisted of complete skeletonization of all common, external, and internal iliac vessels, and harvesting of all fatty and lymphatic tissue above and below the obturator nerve. After the peritoneal incision, all lymphatic tissue was harvested from the lateral, anterior, and medial aspects of the vena cava and aorta to the level of the renal veins (Fig. 1).
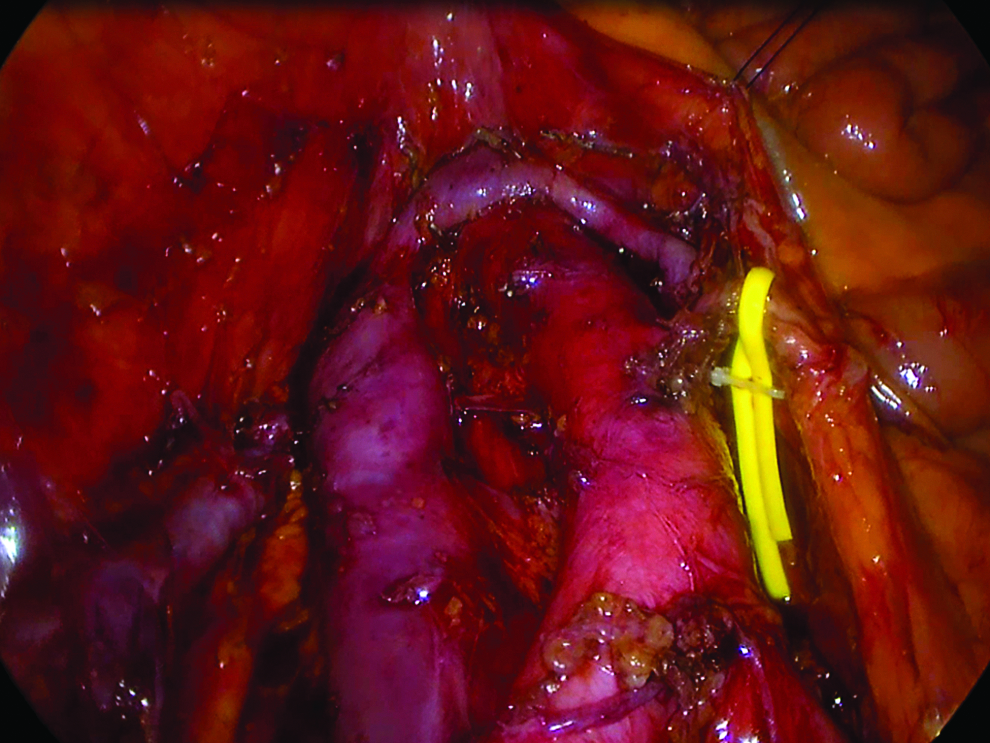
Operating field of laparoscopic systematic para-aortic lymphadenectomy for endometrial cancer. The left renal vein is the cranial border of dissection that was exposed. The vena cava and the anterior aspect of the aorta were cleared. The superficial intercavoaortic nodes were also removed.
Statistical analysis
All of the statistical analyses were performed using the JMP software package (version 11.1.1; SAS, Cary, NC). Continuous variables were expressed as the mean ± standard deviation (SD). The Mann-Whitney–U test was used to compare continuous variables, and Fisher's exact test was used to compare frequencies. p-Values of <0.05 were considered to indicate statistical significance.
Results
Table 1 shows the characteristics of 153 patients with endometrial cancer who underwent systematic para-aortic lymphadenectomy. Fifty-four patients underwent systematic para-aortic lymphadenectomy with laparoscopy and 99 with laparotomy. In the laparoscopic group, 21 patients had stage IA disease, 19 had stage IB disease, 5 had stage II disease, and 9 had stage III disease. In the laparotomic group, 35 patients had stage IA disease, 19 had stage IB disease, 9 had stage II disease, and 36 had stage III disease. While 74.1% of patients in the laparoscopic group had stage I disease, 54.5% had stage I disease in the laparotomic group; this indicated that the patients in the laparotomic group had more advanced disease than those in the laparoscopic group.
Histologically, in the laparoscopic group, 21 patients had G1 endometrioid carcinoma, 10 had G2 endometrioid carcinoma, 17 had G3 endometrioid carcinoma, 2 had carcinosarcoma, 3 had serous carcinoma, and 1 had another histologic carcinoma. In the laparotomic group, 38 patients had G1 endometrioid carcinoma, 24 had G2 endometrioid carcinoma, 18 had G3 endometrioid carcinoma, 4 had carcinosarcoma, 2 had clear cell carcinoma, 9 had serous carcinoma, and 4 had other histological carcinoma. The rate of type 1 carcinoma did not differ significantly between the groups (57.4% versus 62.6%).
In the laparoscopic group, hysterectomy was performed in 22 patients as total laparoscopic hysterectomy, in 20 patients as extended hysterectomy, and in 12 patients as modified radical hysterectomy. In the laparotomic group, hysterectomy was performed in 65 patients as total abdominal hysterectomy, in 23 patients as modified radical hysterectomy, and in 11 patients as radical hysterectomy. Omentectomy was performed in 8 patients (14.8%) in the laparoscopic group and in 39 patients (39.4%) in the laparotomic group.
Table 2 shows the results of the study. The mean (± SD) age of the patients (57.9 ± 11.0 versus 58.0 ± 10.3; p = 0.9) and body mass index (22.8 ± 11.0 versus 22.4 ± 4.3 kg/m2; p = 0.6) were not significantly different between the groups, nor was the mean operation time (483 ± 102 versus 481 ± 106 minutes; p = 0.9). The laparoscopic group had less intraoperative blood loss than the laparotomic group (143 ± 253 versus 988 ± 694 mL; p < 0.01). Naturally, the rate of blood transfusion was lower in laparoscopic group than in the laparotomic group (3.7% versus 10.0%; p = 0.1). The number of resected pelvic lymph nodes was less in the laparoscopic group than in the laparotomic group (31.8 ± 10.1 versus 39.9 ± 15.9; p < 0.01). The number of resected para-aortic lymph nodes was also less in the laparoscopic group than in the laparotomic group (26.2 ± 10.9 versus 31.1 ± 13.2; p = 0.02). The postoperative minimum level of hemoglobin was higher in the laparoscopic group than in the laparotomic group (10.4 ± 1.1g/dL versus 9.9 ± 1.4 g/dL; p = 0.02). In contrast, the postoperative maximum level of C-reactive protein was lower in the laparoscopic group than in the laparotomic group (6.3 ± 3.8 mg/dL versus 10.2 ± 4.9 mg/dL; p < 0.01).
Based on an analysis of variance (mean ± SD).
Median (+ interquartile ranges).
BMI, body mass index; SD, standard deviation; EBL, estimated blood loss; Hb, hemoglobin; CRP, C-reactive protein.
The rate of intraoperative complications was not significantly different between the groups (5.6% versus 8.1%; p = 0.7). Two vessel injuries and 1 compartment syndrome occurred in the laparoscopic group, and 6 vessel injuries, 1 ureter injury, and 1 obturator nerve injury occurred in the laparotomic group. The 2 patients with vessel injuries in the laparoscopic group were converted to laparotomy for hemostasis; the conversion rate of laparoscopic para-aortic lymphadenectomy was 3.7%.
Postoperatively, there were 1 urinary-tract infection, 1 case of pelvic cellulitis, 3 cases of venous thrombosis, and 3 cases of pulmonary embolus in the laparotomic group. No complications described above occurred in the laparoscopic group. Bowel obstruction and urinary fistula did not occur in either group. While no cases of ileus occurred in the laparoscopic group, 10 occurred in the laparotomic group. There were 2 wound infections in the laparoscopic group and 3 in the laparotomic group. There were 2 cases of lymphocyst in the laparoscopic group and 1 in the laparotomic group. The rate of chyle or lymphhorrhea was higher in the laparoscopic group than in the laparotomic group (18.5% versus 7.1%; p = 0.02). These symptoms resolved spontaneously in a few days with observation and basic support. The rate of lymphedema was lower in the laparoscopic group than in the laparotomic group (3.7% versus 13.1%; p = 0.07). The laparoscopic group tended to have shorter hospital stays than the laparotomic group (8.4 ± 5.7 days versus 16.1 ± 8.0 days; p < 0.01). The medium (quantile) duration of follow-up was 364 (110–681) days in the laparoscopic group and 693 (267–1222) days in the laparotomic group. The recurrence rate was not significantly different between the groups in the above time period (7.4% versus 14.3%; p = 0.2).
Discussion
In the current study, laparoscopic surgery with para-aortic lymph node dissection for patients at intermediate/high risk of recurrence, such as those with deeply invasive lesions, high-grade histology, and tumors of serous carcinoma, clear cell carcinoma, or carcinosarcoma features of endometrial cancer had roughly the same operation time, less intraoperative blood loss, and a shorter hospital stay than laparotomic surgery. The rate of intraoperative complication was not significantly different between the groups.
There have been several studies demonstrating the feasibility of laparoscopic surgery for patients with endometrial cancer. In these studies, laparoscopic surgery involved less intraoperative blood loss and shorter hospital stays than laparotomic surgery.16–21 The Gynecologic Oncology Group's LAP 2 study, which was a multicenter randomized trial comparing treatment of endometrial cancer performed by laparoscopy versus laparotomy, demonstrated not only the short-term feasibility of laparoscopy but also its noninferiority with regard to long-term prognosis, compared with laparotomy. In this study, both pelvic lymphadenectomy and para-aortic lymphadenectomy were performed in 91.5% of laparoscopy patients and in 95.8% of laparotomy patients. The median operation time was 204 minutes for laparoscopy and 130 minutes for laparotomy. 16 However, there was substantial variation between the procedures in operative time, which is based on the extent of the procedure, how radical it is, the number of yielded nodes, and the experience and learning curve of the surgical team. In the current study, similar feasibility was found for laparoscopy, including relatively little blood loss, a similar operative time, and shorter hospital stays than for laparotomy.
The number of dissected lymph nodes was fewer in the laparoscopic group than in the laparotomic group. The appropriate number of lymph nodes to be removed remains controversial. What is adequate lymph-node dissection? How many lymph nodes should be removed? While these questions remain unanswered, several studies have clarified the median number of removed lymph nodes. In Kilgore et al.'s study, the median number of removed lymph nodes for a biopsy was 11, 1 while Chuang et al. removed a median of 9 lymph nodes. 22 In Chan et al.'s retrospective review of the SEER [Surveillance, Epidemiology, and End Results] database, extensive lymph node dissection improved the 5-year disease-specific survival in patients with >20 lymph nodes removed. 23 Lutman et al. reported that ≥12 removed lymph nodes was a major influential factor affecting the outcome of patients with high-risk endometrial cancer. 24 In the SEPAL [survival effect of para-aortic lymphadenectomy] study, Todo showed that para-aortic lymphadenectomy improved the prognosis of patients with intermediate- to high-risk endometrial cancer. The median number of para-aortic lymph nodes removed in that study was 23. 11
In the current study, 26.2 lymph nodes was the median number of para-aortic lymph nodes resected by laparoscopy, which the current authors believe was a permissible number, although a longer follow-up will be needed before long-term survival can be evaluated accurately.
There have been several studies on complications associated with laparoscopic para-aortic lymphadenectomy. In the LAP 2 study described above, the rate of intraoperative complications was not significantly different between the laparoscopy and laparotomy groups (10% versus 8%). However, the percentage of patients with arterial bleeding was significantly higher in the laparoscopy group than in the laparotomy group (1.8% versus 0.7%). Of the 30 laparoscopy patients who had arterial bleeding, 11 cases were controlled without conversion to laparotomy. The rate of postoperative complications was lower in the laparoscopy patients than in the laparotomy patients. Ileus and cardiac arrhythmia were more common in the laparotomy group. 16 In the current study, 2 patients in the laparoscopic group had intraoperative vessel injury, which resulted in conversion to laparotomy. Postoperatively, the rate of complications was lower in the laparoscopic group than in the laparotomic group.
Several limitations associated with the present study warrant mention. First, a multivariate analysis could not be performed due to the small sample size. Second, long-term prognosis could not be determined within the short follow-up period. However, the current authors believe that laparoscopic para-aortic lymphadenectomy is feasible and can be substituted for laparotomic procedures for patients with early stage endometrial cancer.
Conclusions
This laparoscopic procedure had a similar mean operation time, lower rate of intraoperative hemorrhaging, and shorter hospital stay than the laparotomic procedure. The rate of intra- and postoperative complications was not significantly different between the groups. While fewer lymph nodes were dissected in the laparoscopic group than in the laparotomic group, the numbers were still in the permissible range. Taken together, these findings suggest that laparoscopic systematic para-aortic lymphadenectomy was safe and feasible, compared with laparotomic systematic para-aortic lymphadenectomy.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest in association with this study.