
Abstract
Abstract
Introduction
Inadequate accessibility and visibility caused by insufficient space for thick clamps and suture ligation posed difficulties during attempted vaginal hysterectomy in patients with previous cesarean sections. Use of bipolar forceps for hemostasis and right-angle forceps to delineate anatomy, as well as use of fiberoptic cables, as done in the Purohit technique for vaginal hysterectomy, 6 may improve visibility, accessibility, and ease of vaginal hysterectomy in such cases. Many more vaginal hysterectomies associated with cesarean section may be attempted easily.
Conventional careful dissection of the bladder from the uterus in patients with dense uterovesical adhesions caused prior cesarean sections has still been responsible for causing a fear of unintentional bladder injuries during vaginal hysterectomies1,5,7 and in the vaginal phase of laparoscopic-assisted vaginal hysterectomies. 8 Unintentional bladder injury increases morbidity. 9
Instead of making a direct attempt to perform careful dissection in the uterovesical space, the current authors formulated an indirect posterioanterior approach during vaginal hysterectomy; this approach (the Purohit technique) is described later in this article. The objective of this approach was to mobilize all of the dense uterovesical adhesions intact, from their higher level down to the level where direct tactile palpation by the surgeon was possible. The next step was to thin out the thick uterovesical adhesions, layer by layer, under direct vision, to differentiate and dissect the bladder away from the uterus. The overall purpose of this refinement was also to facilitate the approach and minimize chances of unintentional bladder injuries during vaginal hysterectomies in patients who have had prior cesarean sections and who had dense uterovesical adhesions.
Materials and Methods
An observational study was conducted in a private general hospital between February 2010 and June 2012.
Inclusion criteria and consent
All candidates for hysterectomy for benign indications who had had previous cesarean sections were examined for clinical and sonographic signs10–12 of fixed adhesions of uterine corpi to anterior abdominal-wall incisions made for the prior cesarean sections. Candidates who had such adhesions10–12 were excluded from undergoing vaginal hysterectomy. There were no other exclusion criteria for the other candidates.
Written informed consent was obtained from each patient. An institutional ethics committee reviewed and approved the study. Selected candidates were allowed to undergo vaginal hysterectomies.
Outcomes sought
The primary outcomes of interest were the success of vaginal hysterectomies and the number of unintended cystostomies resulting from separation of the bladders from the uteri.
Secondary outcomes were the need for conversion to laparotomy and other intraoperative and postoperative complications.
Procedures
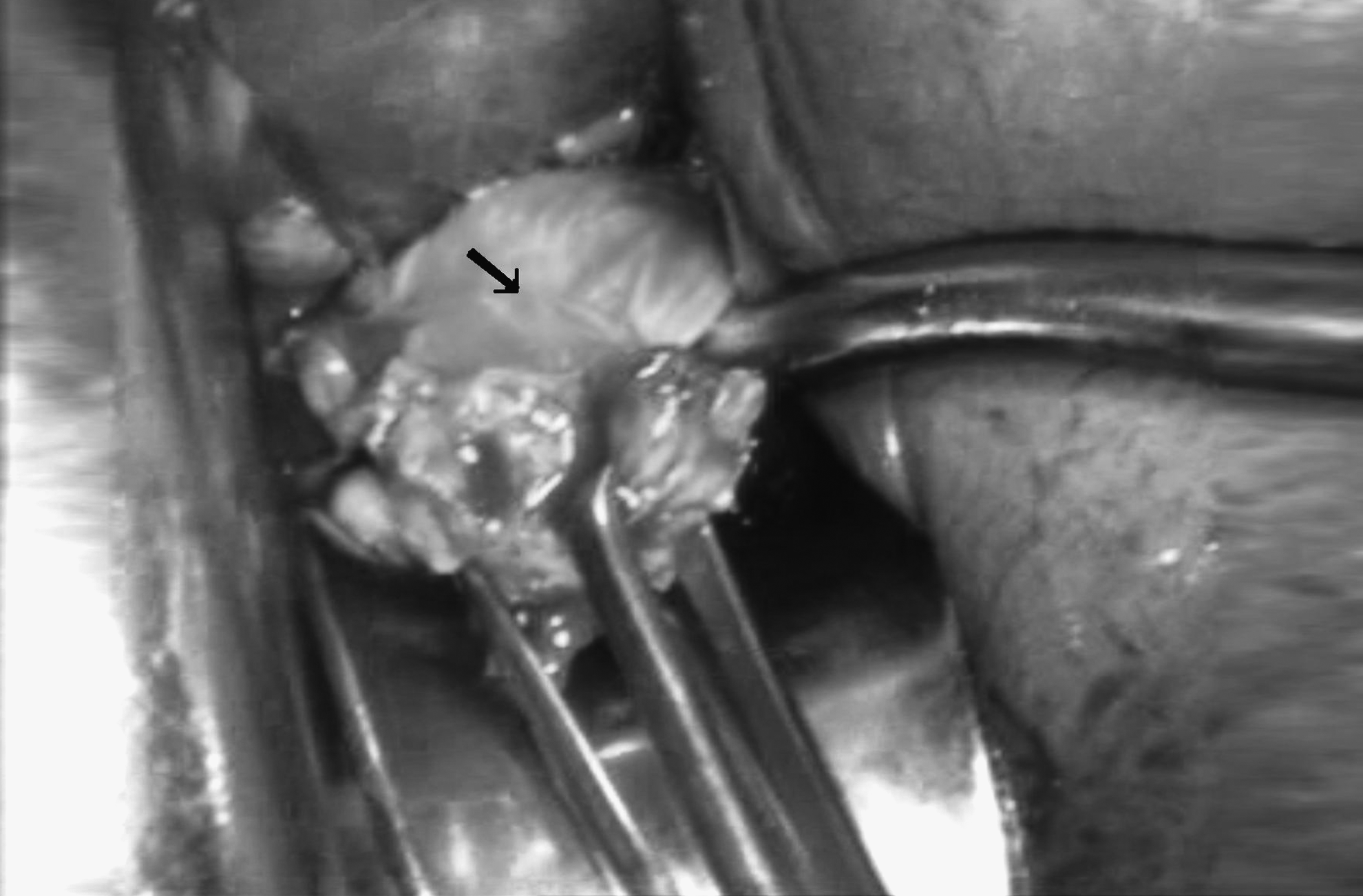
Each patient was positioned for dorsal lithotomy, flexing the thigh toward the abdomen. Vaginal hysterectomy was started, using the Purohit technique.6,13 Figure 1 shows the vaginal walls separated from the cervix by applying a monopolar current (40 Watts). The lower part of the cardinal ligament of ∼1 cm on the right side of the cervix was separated from the cervix, after bipolar coagulation (applying a 50-Watt current) to create a split. Through the split, the tip of a closed-right angle forceps was inserted anteromedially between the anterior wall of the cervix and the vaginal wall (lateral application of the right-angle forceps). Prongs of the right-angle forceps were opened to stretch and spread the supravaginal septum (Fig. 1). The septum was coagulated close to the cervix and divided by scissors allow entry into the vesicocervical space.

The supravaginal septum (arrow) is stretched between the prongs of a right-angle forceps. Bipolar coagulation forceps are close to the cervix.
Separation of the remaining portion of vesicocervical–cardinal ligament from the cervix extraperitoneally was performed after bipolar coagulation exposed the bulge of the uterine artery. The uterine artery was coagulated by a bipolar current and divided extraperitoneally between the prongs of the right-angle forceps.6,13 The above procedures were repeated on the opposite side to secure the uterine artery and to enhance uterine descent.
Then the posterior cul-de-sac was opened. The uterosacral ligament and the posterior leaf of the broad ligament, up to the level of the stump of the uterine artery on either side of the uterus, were gradually stretched between the prongs of the right-angle forceps, coagulated, and separated by scissors to enhance the descent of the uterovesical space toward the surgeon. Adhesions in the uterovesical space were dissected—layer by layer, using the tip of the right-angle forceps—from their lateral aspects to enable visualization of the uterovesical fold of the peritoneum. Then the anterior cul-de-sac peritoneum was entered and the vaginal hysterectomy was continued, again, using the Purohit technique.6,13
When dense vesicouterine adhesions obstructed the accessibility of the anterior cul-de-sac, blurred the anatomical planes, and raised concerns about the potential for bladder injury during careful dissection with scissors, 7 the attempt to access the anterior cul-de-sac using anterior vesicouterine dissection was stopped. Then, a posterioanterior approach was started, to bring the whole uterovesical adhesion down to the level where direct tactile palpation of its contents by the surgeon was possible for differentiating the anatomy.
The cervix was split at the midline. Bisection incision was stopped just below the level of the thick vesicouterine adhesions. The incision of the posterior uterine wall was progressed cranially. Wedge morcellation beneath the serosa was performed to reduce the width of the posterior wall of the uterus. Long single-tooth tenaculums (26 cm) were useful for moving upward on the incised margin. Decompression of the posterior uterine wall and fundus mobilized the broad ligament and ovarian ligaments medially. The residual portion of the posterior leaf of the broad ligament on either side was separated from the uterus to enhance descent of the uterus.
Forward and outward traction of the upper incised margin of the posterior uterine wall at this stage exposed the deeply placed white ovarian ligament. The ovarian ligament was hooked by the bend of the right-angle forceps from its posterior aspect, spread between its prongs, coagulated close to the uterus (Fig. 2), and divided by a pair of scissors. The above procedure was repeated on the opposite side to detach both ovarian ligaments from the uterus. Deaver's retractors (2.5 cm in width) and a pelvic illuminator (Kalelker Surgicals, Mumbai, India) with a fiberoptic light source were used occasionally to improve visibility 6 at this step of the procedure.

Right ovarian ligament (arrow) stretched between the prongs of a right-angle forceps. Bipolar coagulation forceps (22-cm long with a tip width of 2 mm) are close to the uterus. Allis forceps are shown, at the lowest part of this photograph, retracting the upper incised margin of the posterior uterine wall to expose the ovarian ligament.
Wedge morcellation beneath the serosa was repeated to reduce the bulk of the corpus above the level of the ovarian ligaments. Forward and outward traction of the upper incision margin of the remaining portion of the posterior wall, using Allis forceps, exposed the uterine end of the pink tube and round ligament. The tube and round ligament were hooked by the bend of the right-angle forceps from their posterior aspects and were separated from the uterus, using the same technique mentioned above for the ovarian ligament. The opposite-side tube and round ligament were similarly separated from the uterus.
Separation of upper pedicles bilaterally dropped the anterior uterine wall with uterovesical adhesions, bladder pillars, and the anterior leaf of the broad ligament further down toward the surgeon. Omental adhesions, if any present at this stage, were separated from the fundus of the uterus. Then the surgically freed fundus was excised to reduce the length of the anterior uterine wall.
At this stage, the vesicouterine fold of the peritoneum was visible through the posterior peritoneal opening. The anterior cul-de-sac was palpable, by sweeping an anteriorly bent index finger that was inserted through the posterior peritoneal opening.
Forward and outward traction of the incised cranial margin of the anterior wall by the surgeon at this stage, made it possible to see the thick bands of scarring of the broad ligament above the level of the lower-segment cesarean section scar. Until this stage, these bands of scar tissue had contracted and pulled the uterovesical space up.
These tough anterolateral adhesions were approached, layer by layer, by the tips of the right-angle forceps that were inserted from the adhesions' lateral aspect. They were separated bilaterally from the uterus by the same technique mentioned above for the broad ligament to enhance descent of the remaining central portion of the vesicouterine adhesions.
The vesicouterine adhesions were palpated directly between anteroposteriorly placed index fingers of both hands. The thick fibrous vesicouterine fold of the peritoneum was differentiated from the firm uterine wall and the fleshy bladder wall. The vesicouterine peritoneum was incised.
The residual portion of these vesicouterine adhesions was palpated and thinned out, layer by layer, by the tip of the right angle forceps to isolate (if any were present) fixed cohesive uterovesical adhesions (Fig. 3). No attempt was made to dissect the fixed cohesive uterovesical adhesions. At this point, the cervix was excised just below the fixed uterovesical adhesions, and a slice of the superficial layer of the uterus was spared with with the posterior wall of the bladder to avoid an unintended cystostomy. In the absence of such inseparable cohesive uterovesical adhesions, layer-by-layer dissection separated the bladder easily from the uterus to complete the hysterectomy. No sponges or holders or finger dissections were used at any stage for mobilization of adhesions.
Fixed cohesive uterovesical adhesions (arrow). Allis forceps are shown retracting the residual portion of the uterine wall.
Bladder integrity was confirmed by filling the bladder with 200 mL of saline stained with methylene blue, and the presence of any leaking was checked. Salpingo-oophorectomy was done in indicated cases. Finally, the vault was closed.
Results
During the study period, 78 women with previous cesarean section requested hysterectomies for benign indications. The mean age of these women was 40.78±4.59 years. In 14 (17.94%) women, fixed adhesions of uterine corpi to anterior abdominal-wall scars10–12 was diagnosed preoperatively; thus, these candidates were excluded from undergoing vaginal hysterectomy. The rest, 64 women (82.05%) of the total 78 women with previous cesarean section(s), underwent vaginal hysterectomies.
Clinical characteristics of patients (Table 1)
In 51.56% of the cases, there were histories of 2 cesarean sections, 40.62% of the cases had a history of 1 cesarean section, and only 7.81% of the cases had histories of 3 cesarean sections. No patient had a history of 4 cesarean sections. Only 4 cases had histories of previous pelvic operations. In 63 (98.43%) of 64 cases, the cervix was felt without difficulty11,12 during bimanual vaginal examination at the office and operation theater. In 1 case, the cervix was high up because of the presence of long-band omental adhesions between the anterior abdominal wall and a uterus of 16 weeks' gestation size.
The uterus was smaller than 12 weeks' size of gestation in 62 (96.87 %) of 64 cases. Of 2 (3.12%) cases with a large uterus >12 weeks' of gestation, 1 patient had a uterus of 16 weeks' gestation size, and the other patient had a uterus of 18 weeks' gestation size. Thus, vaginal hysterectomy was initiated in every case. The maximum weight of any patient was 108 kg.
Parauterine adhesions (Table 2)
In 26 (40.62%) of 64 patients, there was no obstruction to accessing anterior cul-de-sac, and vaginal hysterectomy was accomplished by using the Purohit technique.6,13 In 38 (59.37%) of 64 patients, there was obstruction to accessing the anterior cul-de-sac because of the presence of dense uterovesical adhesions, and a posteroanterior route of approach was used to accomplish vaginal hysterectomy. Dense uterovesical adhesions were found in 10/26 (38.46%) patients after 1 cesarean section, in 23/33 (69.69%) patients after 2 cesarean sections, and in all 5/5 (100%) patients after 3 cesarean sections.
CS, cesearean section(s).
The posterior cul-de-sac was not obliterated in 62 (96.87 %) cases associated with previous cesarean section(s). In 2 (3.12%) patients, the posterior cul-de-sac was obliterated secondary to severe endometriosis in 1 patient and secondary to chronic pelvic inflammation in the other patient. None of the patients had incidental intraoperative detection of ventrofixation of the uterine corpus to the previous anterior abdominal-wall scar. Vaginal hysterectomy was accomplished in all 64 cases. There were no failures and there were no conversions to address uncontrolled bleeding during these vaginal hysterectomies.
Perioperative outcomes (Table 3)
None of patients were excluded after the start of the procedure. Fixed cohesive uterovesical adhesions were isolated during uterovesical dissection in only 4 (6.25%) cases. In each of these patients, a slice of serosa of the uterus was spared with the posterior wall of the bladder to avoid an unintended cystostomy.
Vaginal oophorectomy was done as indicated 3 (4.68%) cases. The mean operative time was 78.59±33.15 (35–190) minutes. The mean weight of specimen uteri was 161.01±108.87 (50–550) g. Blood transfusion was not needed in any case. Temporary unilateral leg paraesthesia was noted in 1 case, and this condition was relieved spontaneously after 3 postoperative days. No patients had bladder, ureteric or thermal injuries to the pelvic organs. No vesicovaginal fistulas were seen. No other major postoperative complications were seen.
Discussion
Gynecologic surgeons are using the safe vaginal route of hysterectomy increasingly,14,15 and this route may be preferred. 16 Previous cesarean section has still been a significant risk factor for unintended intraoperative cystostomy by all routes including vaginal hysterectomy.1,4,5
The purpose of the present study was to demonstrate a safe approach to ease vaginal hysterectomy in cases of patients with previous cesarean sections in the absence of fixed adhesions of the uterine corpi to previous anterior abdominal scarring and to avoid unintended bladder injuries during vaginal hysterectomy in cases with dense uterovesical adhesions caused by previous cesarean sections.
It was difficult to reach the cervix vaginally in cases associated with fundal adhesion of the uterus to the anterior abdominal wall,10–12 thus patients with this problem excluded from undergoing vaginal hysterectomy. Fixed uterus adhesion to the anterior abdominal wall for prior cesarean section was determined by the clinical and sonographic signs described by Sheth et al.11,12 and El-Shawarby et al. 10 Failed completion of vaginal hysterectomy may occur owing to the presence of thick adhesions between the uterine fundus and the anterior abdominal wall. 17
In the absence of fundal adhesions of the uterus to anterior abdominal wall, hysterectomy was initiated and accomplished vaginally in all cases including 5 cases with 3 previous cesarean sections (Table 2). Other adhesions (Table 2) to the uterus caused by prior cesarean sections did not obstruct the completion of vaginal hysterectomy in this case series. None of these patients were excluded after the start of procedure because of incidental detection of ventrofixation of the uterine corpus to a previous anterior abdominal-wall scar.
The difficulty caused by inadequate lateral space during vaginal hysterectomy by a conventional method in cases with previous cesarean section(s) had been alleviated by the described procedure, using bipolar forceps 6 for hemostasis of pedicles instead of sutures. Similar to the current authors' findings, electrosurgery has been reported to be safe in vaginal hysterectomy by many studies,6,13,18–21 when this technique is applied carefully. Accessibility to pedicles was increased by using a right-angle forceps 6 in this procedure. Visibility had been improved occasionally using a pelvic illuminator with a fiberoptic light source 6 during the procedure. Extraperitoneal 6 ligation of uterine arteries—instead of conventional intraperitoneal ligation—during vaginal hysterectomy decreased need of blood transfusion. Similar to observations by other studies,11,22 the majority of the current series of patients requesting hysterectomy associated with previous cesarean sections had a uterus size of <12 weeks' gestation or 300 g (Table 3). Thus, large volume was not an obstacle to the progress of vaginal hysterectomy in the majority of these cases. Conventional attempts5,7 of vesicouterine dissection in the presence of dense uterovesical adhesions caused by previous cesarean sections, had still carried a risk of bladder injuries in vaginal hysterectomies. Bringing dense uterovesical adhesions down by the described posterioanterior approach so that these adhesions could be palpated in a direct tactile fashion facilitated differentiation of the bladder from the uterus and made uterovesical dissection easier. Isolation of cohesive uterovesical adhesions in this approach prevented unintended bladder injuries in the present case series.
Conclusions
Vaginal hysterectomy for benign indications associated with previous cesarean sections may be accomplished safely in the absence of fixed adhesions of the uterine corpi to previous anterior abdominal scarring. The posterioanterior approach during vaginal hysterectomy may avoid unintended bladder injury in the presence of dense uterovesical adhesions caused by previous cesarean sections.
Footnotes
Disclosure Statement
All authors have no commercial associations that might give rise to a conflict of interest in connection with the publication of this article.