
Abstract
One of the most troublesome overuse injuries is stress fractures, for which female gender is a major risk factor. In 2015, the Israeli government opened identical combat duties for both genders. The purpose of this study is to provide a detailed report regarding the prevalence and characteristics of stress fractures in females that will serve as an evidence-based platform for future policy planning and implementation regarding female integration in combat units. This is a report of a cross-sectional study of 2223 female soldiers recruited to combat units between 2010 and 2013. Data were collected from the Israeli Defense Force's (IDF's) computerized medical consultation records package. Descriptive and analytic statistics were performed to obtain and analyze results. The overall stress fractures rate was 11.6% (258 soldiers). The most frequent site for stress fracture was the distal tibia (215 cases, 83%). The average lost training days due to a stress fracture were 26.6 days. The risk for developing a stress fracture was 2.15 (215%) times higher in the noninfantry group than in the infantry group, (p = 0.0232, 95% confidence interval 1.346, 4.536). The rate of stress fractures and the consequent lost training days in the IDF are high and necessitate the planning and implementation of a comprehensive intervention policy to reduce overuse injuries and stress fracture rates among female warriors.
Introduction
Israel is one of only three countries over the world (Israel, North Korea and Norway) in which compulsory military service for females is mandated. Before 2015, only a few selected combat duties were open for women; most women performed noncombat duties in rear units. All combat duties are now open for both genders. Female gender is considered to be a major risk factor for injuries, and there are substantial physiological differences between males and females that may have deleterious effect on a unit's readiness and performance.1–6 Thus, the full integration of women into combat units may have far-reaching consequences on female soldiers' health, on the resources of military medical services, and on unit's readiness and performance, all of which were described in the experience of the British army. 7
After full integration of females into the British army, British military commanders mandated identical training programs for males and females. The immediate result of this measure was a dramatic increase of injury rates and lost training days among females.7–9
One of the most troublesome overuse injury is stress fractures, which are characterized by significant loss of training days and pose a diagnostic challenge for the combat unit's physicians.2,10 The rates of these fractures also serve as a sensitive indicator for overall overuse injury rates in these units.
The most common site for the occurrence of stress fracture is the distal tibia followed by metatarsal bones, the shaft of the femur, the neck of the femur, and the pelvis.2,11–14 Stress fractures of the femoral neck should draw special attention and treatment since these fractures may be complicated by avascular necrosis of the femoral head, leading to severe disability and the need for hip arthroplasty at a relatively young age.15,16
Purpose
The purpose of this study is to provide a detailed report of the prevalence and characteristics of stress fractures in Israeli female warriors. This report will serve as an evidence-based platform for future policy planning and implementation regarding female integration into combat units.
Materials and Methods
Study design and IRB approval
A cross-sectional study was approved by the Israeli Defense Force's (IDF's) Internal Review Board (IRB), approval number: 1273–2013.
Population
A total of 2223 female soldiers were recruited to combat units during a 4-year period between 2010 and 2013.
The female recruits were divided into two combat training tracks: a noninfantry combat training track that lasted 8–10 weeks and an infantry track requiring greater physical effort and fitness demands; this training program lasted 16–20 weeks.
Inclusion criteria
All females successfully recruited to combat duties during the period of 2010–2013.
Exclusion criteria
(1) Female recruits who did not complete basic combat training due to reasons unrelated to stress fractures.
(2) Female recruits who suffered a stress fracture <2 weeks after beginning of training: the assumption in such case is that the fracture occurred before recruitment and was not related to or caused by training.
Data collection
Data were collected from the IDF's computerized medical consultation records package (CPR®) and introduced into a dedicated SAS® database for further analysis. ICD-10 codes and medical records text including the words “stress fracture” were used to identify cases. The following variables were collected: subject age, weight, height, and body mass index (BMI). The type of training (infantry, noninfantry), type and result of imaging studies, fracture site, method of diagnosis (clinical/documented by imaging studies), and number of lost training days were also tabulated.
Data analysis
SPSS® version 21 was used for statistical analysis.
Descriptive statistics were performed using means and standard deviations to express results. For the statistical significance of the comparison of two dichotomous variables, chi square test was used. For the statistical significance of the comparison of interval variables divided into two categories, Student's t-test was used.
For three groups or more, analysis of variance (ANOVA) was used with multidirectional comparison performed by Tukey's post hoc method.
Although this is primarily a descriptive study, some associations between exposure and outcome variables were examined using logistic regression models after adjusting for potential confounders or effect modifiers.
Results
In this study, 2223 female soldiers were included. A total of 1384 (62%) were trained in the noninfantry combat training track and 839 (38%) were trained in the infantry combat training track. In the noninfantry group, mean weight, height, and BMI were 59.66 ± 10.7 kg, 162.81 + 5.97 cm, and 22.5 ± 3.54 kg/m2, respectively. The mean weight, height, and BMI in the infantry group were 60.67 ± 9.7 kg, 162.82 ± 5.95 cm, and 22.88 ± 3.39 kg/m2, respectively. The differences of weight and BMI between groups were statistically significant (p = 0.0202, p = 0.0118, respectively). The height difference between the groups was not statistically significant (p = 0.9679). For detailed anthropometric data by training track, see Table 1.
Anthropometric Data by Training Track
BMI, body mass index.
Out of 2223 female soldiers, 258 (11.6%) were diagnosed with a stress fracture. Two hundred fifteen fractures (83%) were clinically diagnosed. Sixty-four bone scans were performed, of these, 43 (67%) demonstrated stress fractures and confirmed the clinical suspicion of a stress fracture, 6 (10%) were negative for stress fractures, and for 15 (23%) of the results of bone scanning were missing.
The most frequent stress fracture site was the distal tibia (215 cases, 83%). For detailed distribution of stress fractures by site of fracture, see Figure 1.
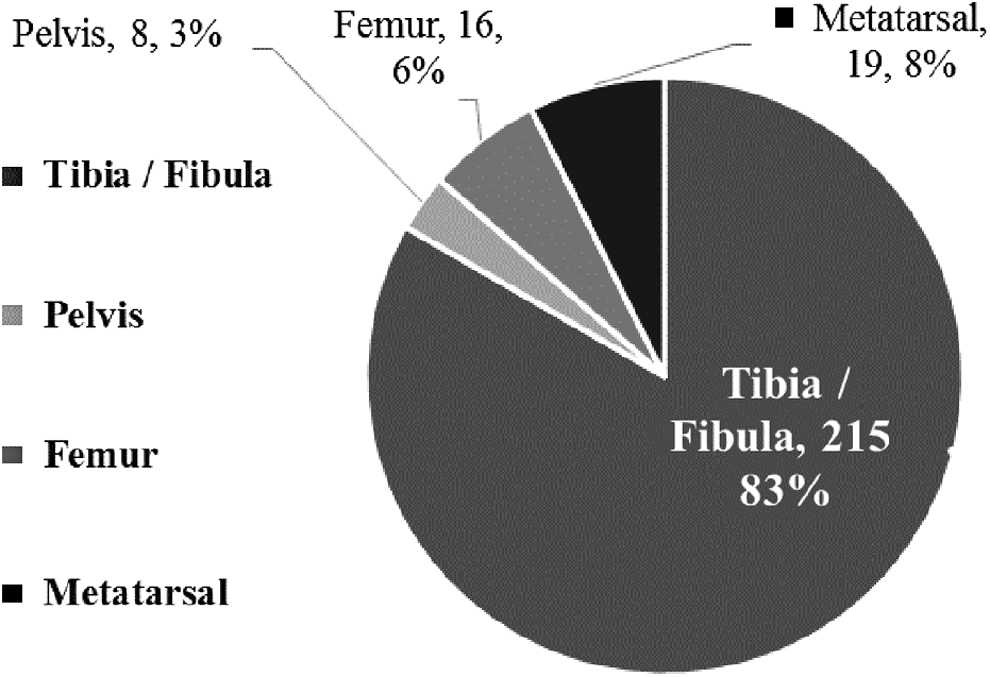
Stress fractures distribution by site of injury.
The average lost training days due to a stress fracture were 26.6 days. The averages lost training days for metatarsal, distal tibia, femur, and pelvis stress fractures were 16, 29, 40, and 42 days, respectively. Five percent of soldiers diagnosed with a stress fracture lost <11 training days, 62% lost 11–30 training days, 33.5% lost >30 training days, and 13.5% lost >50 training days. For detailed distribution of soldiers diagnosed with stress fractures by amount of lost training days, see Figure 2.
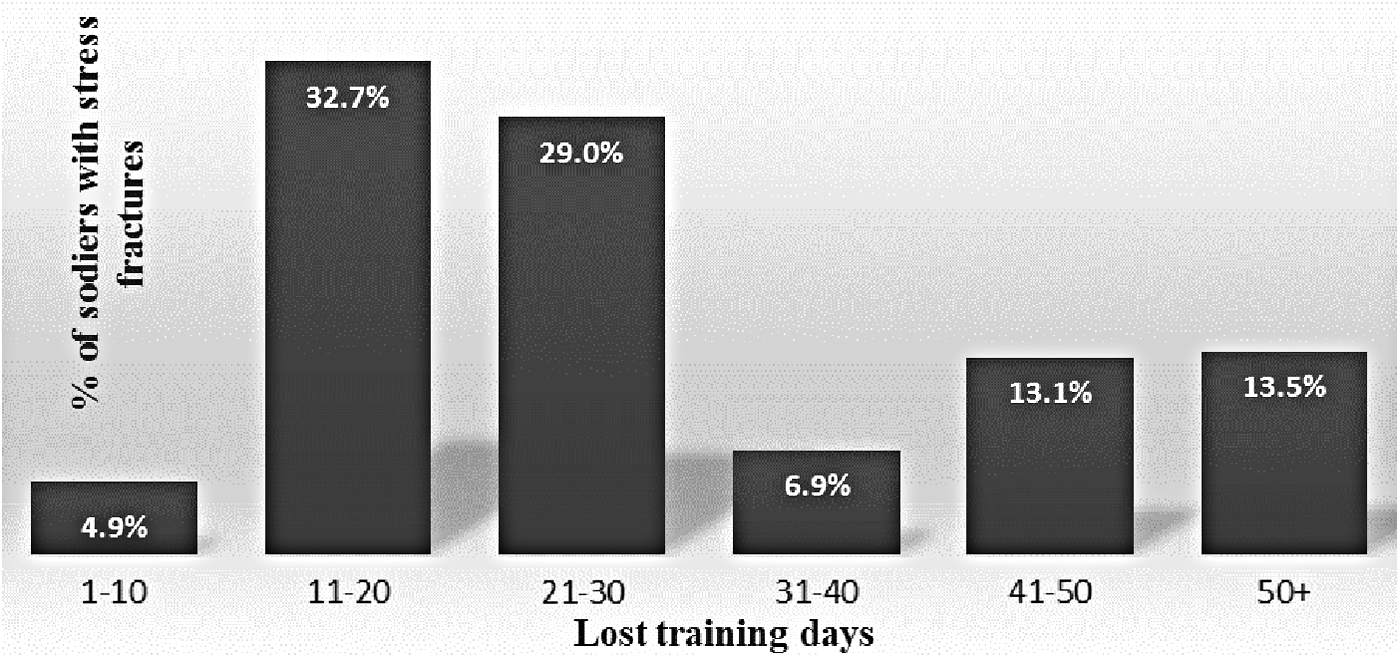
Detailed distribution of soldiers diagnosed with stress fractures by amount of lost training days.
After adjusting for age and BMI, the risk for developing a stress fracture was 2.15 (215%) times higher in the noninfantry group than in the infantry group. This result was statistically significant (p = 0.0232, 95% confidence interval 1.346, 4.536). For detailed logistic regression results for the adjusted association between training type and stress fracture development, see Table 2.
Logistic Regression Results for the Adjusted Association Between Training Type and Stress Fracture Development
Discussion
The purpose of this study was to characterize and evaluate the frequency of stress fractures among females in the IDF.
The mean BMI was 22.6 kg/m2 with a standard deviation of ±3.5 kg/m2, which demonstrates that most female soldiers were in the normal category of weight (category II, normal weight 18–25 kg/m2) or slightly overweight (category III, overweight 25–30 kg/m2). Although statistically significant differences in weight and BMI were found, we consider these small differences clinically insignificant.
The rate of stress fractures observed in this study was 11.6% and is similar to rates in other armies around the world. 17 Most stress fractures (83%) occurred in the calf and ankle region, most of these (90%) in the distal tibia. These numbers are similar to the numbers reported in other studies performed on military14,17 and nonmilitary2,11–13 populations. The quoted studies on military populations included male and female recruits during combat training who were trained following the same training program.
In the Australian army, an intervention plan for reduction of stress fractures was conducted and resulted in a vast reduction in pelvic stress fracture rates from 11.2% to 0.6%. 17 In light of the fact that bone scan data results were missing in 23% of women, we propose a comprehensive study to define the precise sensitivity and specificity of clinical and imaging diagnosis to establish an IDF diagnosis protocol. Such a protocol should include guidelines for the use of clinical diagnosis, diagnosis by imaging, or both modalities.
The rate of femoral stress fractures was 6%. Unlike stress fractures of the distal tibia, femoral stress fractures have the potential for severe complications with the result of permanent disabilities. We urge a dedicated effort to ascertain the risk factors for these fractures and the implementation of plans for intervention to reduce the high rate of these fractures.
The risk of developing a stress fracture among female soldiers who performed noninfantry combat basic training was 2.15 times higher than that of female soldiers who performed infantry basic combat training (odds ratio = 2.15, p = 0.0232). This result is surprising and counter intuitive, since the infantry combat training is twice as long and requires higher physical effort and fitness demands. The main reasons for this surprising finding in our opinion may be the higher professional level of the training team and the basic physical fitness of the soldiers in the infantry combat training units as compared with the noninfantry units.
Another reason that may explain this finding may be related to nutrition issues such as low vitamin D levels and lack of adequate sleep duration in the noninfantry units. Again, these data suggest the need for a study to delineate the reasons for this unexpected finding.
Sixty-two percent of those who suffered a stress fracture lost >21 days of training and 21% lost >40 days of training. These numbers are very high and emphasize the need to consider stress fractures prevention among female soldiers as a high priority military public health issue.
Conclusions and Recommendations
(1) The rate of stress fractures among female soldiers during basic combat training is high and the lost training days due to these fractures are very high. Therefore, an aggressive intervention is recommended to significantly reduce the rates of these fractures. The necessary financial and personnel resources to reduce these fractures should be allocated so that a plan for intervention can be formulated.
(2) The surprising finding of a higher risk of developing a stress fracture among female soldiers in noninfantry basic combat training as compared with infantry basic combat training should be comprehensively investigated.
Footnotes
Authors Disclosure Statement
No competing financial interests exist.