
Abstract
Objective:
Exergames are playing an important role in person-centered therapy, health care services, and in the rehabilitation field. This study aimed to compare the effects of cooperative, competitive, and solitary exergames on cognition and anxiety levels in children with developmental disabilities (DD).
Materials and Methods:
This study was a randomized controlled trial pretest–posttest including 36 children with DD who were allocated to the cooperative exergame group (CGG), competitive exergame group (CmGG), and solitary exergame group (SGG). The exergame program was performed two times a week for 8 weeks and the outcome measurements were conducted before and after the program. A paired sample t-test and one-way analysis of variance (ANOVA) were used to analyze the changes within and between the groups.
Results:
The result indicated a significant improvement in memory, attention, and visual perception in all groups; the CGG and CmGG showed a high increase in attention compared with the SGG. However, only the CGG presented a significant improvement in the language subscale. In terms of anxiety, only the CGG presented substantial improvements in all anxiety subscales. The CmGG showed improvement in social phobia and the SGG in physical injury fears, social phobia, and general anxiety fears.
Conclusion:
The findings suggest that cooperative and competitive exergames may be used to effectively improve cognitive functions; cooperative exergames can be applied as the most effective method to reduce anxiety compared with the other game types for children with DD.
Introduction
Developmental disabilities (DD) are a category of health conditions that start from a very early stage of the developmental period and usually last all over the lifetime. 1 Some of the common types of DD include attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), cerebral palsy, obsessive-compulsive disorder (OCD), intellectual disorders, and learning disorders. 2 Many individuals with DD experience a cognitive impairment, which is one of the hallmarks of deficits. 3 It affects many domains such as attention, memory, reasoning, planning, and problem-solving abilities.2,3 In addition, children with DD generally have a high level of anxiety which is among the major problems of children themselves and their families. It is associated with panic and confusion, feelings of stress, activation of the autonomic nervous system, and possibly detrimental effects on skills and performance. 4
According to a recently published nationwide population-based study, the prevalence of children with DD has considerably increased from 0.6% in 2003 to 2.5% in 2017 among the Korean population. 5 The increased number of children with DD indirectly affects children themselves, their families, and their communities. Therefore, a particular interest in research for childhood intervention is consistently required.
Although some normal developing children may respond positively to face-to-face interventions, most children with DD have difficulties expressing themselves verbally and may need a different approach. Knowing that games have essential value for children regarding healthy development, they may be used to create an adequate environment to develop cognitive skills, and decrease anxiety.6,7 However, different sorts of games may have varied impacts on children. Thus, it is important to determine the effective game types that will be adequate to improve cognition and anxiety levels in children with DD.
Recently, exergames (a combination of exercise and videogames) are playing a capital role in the health care and rehabilitation field. 8 Based on the interaction of the players and their opponents, we can divide exergames into three types namely cooperative, competitive, and solitary exergames. Cooperative exergames require players to participate in the game as a team, whereas competitive exergames are those in which players play against each other and where one player winning means another player loses. Solitary exergames are those played as a single player with players' objectives independent and indicating that winning or losing does not impact the result of others.
Two published reviews analyzed the use of exergames in children with ASD and both found promising effects on behavioral outcomes (restricted and repetitive behaviors), cognitive function (memory, attention, cognitive flexibility, and inhibition), and physical fitness (cardiorespiratory function, strength, endurance, and agility).9,10 Most studies included in those reviews used Xbox Kinect or Nintendo Wii with solitary exergames as they examined separately their effects on each participant. Another study that used solitary exergame on Xbox Kinect also found a significant improvement in executive function and motor abilities in children with ADHD. 11 Two studies have examined the effects of exergames on anxiety, one in healthy women, 12 another in women with systemic lupus erythematosus. 13 Both found a significant decrease in anxiety levels after performing exergames, although there is a lack of evidence on the impact that solitary exergames have on anxiety levels in children with DD.
Regarding the use of cooperative exergames, studies were found to have positive benefits on prosocial acts and physical contact in normal developing children.14,15 Moreover, a review conducted by Marker and Staiano 16 showed an increase in motivation, self-efficacy, and prosocial behaviors during cooperative exergames. Two studies that compared the effects of cooperative and competitive exergames reported that competitive exergames improve executive function more than cooperative exergames in adolescents with obesity 17 while only cooperative exergames significantly improved anxiety levels in healthy adult males. 18
Despite the positive results found in the previous studies, there were no descriptions of how much interactions with peers during the game may have impacted their anxiety levels considering that interplay with others can be challenging and highly demanding. Therefore, further research is needed to determine how competitive and cooperative exergames affect children with DD, particularly in terms of anxiety outcomes. There has not been any prior research that compared the impacts of various exergame genres on cognition and anxiety in children with DD. It would be of special interest to know which of the cooperative, competitive, and solitary exergames is more effective to improve cognition and reduce anxiety in those children.
The purpose of this study was to compare the effects of cooperative, competitive, and solitary exergames on cognition and anxiety levels in children with DD. We expect that the findings of this study will provide evidence of the effective exergame type that can be practically used for improving cognition and reducing anxiety in children with DD. Furthermore, this study may provide directions for further research to design customized exergames for children with DD.
Materials and Methods
Research design
This study was a randomized controlled trial pretest–posttest with three groups conducted in the Department of Physical Therapy at Sun Moon University, Korea. Participants were randomly assigned to one of the three groups, and the intervention lasted for 8 weeks. The outcome measurements were performed by a trained pediatric physiotherapist before and after the intervention.
Ethical considerations
The study procedure followed the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of Sun Moon University (SM-202104-042-2). Since the participants were children younger than 18 years of age, written informed consent was acquired from their parents or legal guardians. Before starting the experimental procedure, children and their parents received a full explanation of the purpose and procedure of the research and were given the possibility to ask any questions about the study.
Sample size calculation
The sample size was calculated using the computer software G-power version 3.1.9.7. (Heinrich Heine, University, Düsseldorf, Germany) with the following setting: analysis of variance (ANOVA): repeated measures, within–between interaction, effect size (f) of 0.4 (standardized effect size, Cohen's f large effect size), 19 alpha level set at 0.05, power (1−β) of 95%, with three groups and two measurements, and nonsphericity correction (Є) of 1. The sample size needed was 30 with 10 participants per group. However, two more participants for each group were recruited in case of dropout.
Participants
Participants were recruited from local social welfare centers for individuals with special needs. Children were referred to the study by their parents and social workers. A total of 36 children between the ages of 6 and 16 participated in this study. All the children were attending school (some in special education school) and their diagnosis was confirmed by their parents and the social workers.
The inclusion requirements included having a DD diagnosis or exhibiting some of its symptoms, as well as not having any issues with vision, hearing, or following simple directions. Exclusion criteria were children with severe genetic conditions (i.e., Down syndrome), those who were not able to or did not want to follow the instructor's directives, and unable to stand unassisted. Figure 1 provides the flow diagram of the study.
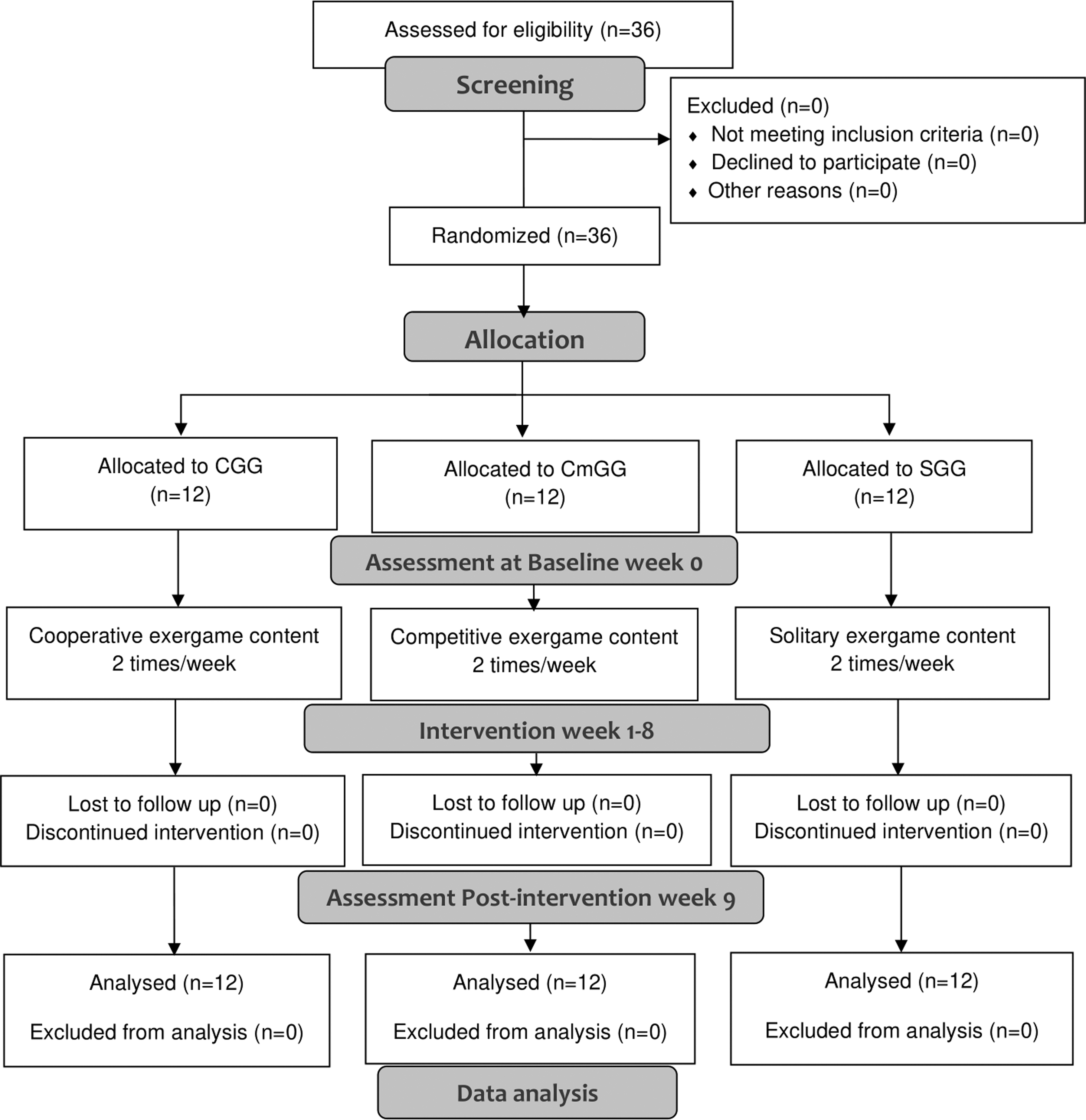
Study flow diagram.
Randomization and blinding
Participants were randomly allocated to one of the three groups: the cooperative exergame group (CGG), the competitive exergame group (CmGG), and the solitary exergame group (SGG). The allocation was conducted by an independent investigator who generated 36 cards with three different colors. The cards were placed into sealed envelopes and participants were asked to pick one card among the 36. They were assigned in a 1:1 ratio to the group according to their card. Participants were blinded to the type of exergames that were played in separate group sessions. Moreover, the outcome examiner was not aware of the group allocation of the participants.
Outcome measurements
Cognition
The computerized cognitive testing program (CoSAS-S; NetBlue Ltd, Daegu, Korea) was used to measure various cognitive functions. The CoSAS-S is a tablet-based cognitive measurement widely used in Korean clinics. It measures six specific domains related to orientation, memory, attention, visual perception, language, and high-level cognition. It includes 29 items and has been reported to have excellent interrater reliability with an intraclass correlation coefficient between two raters of 0.93 (P < 0.001; 95% confidence interval = 0.82–0.97). 20 The score ranges from 0 to 100 with a higher score indicating a higher cognitive function level. A detailed explanation of the measurement procedure has been published elsewhere. 21
Anxiety
The Spence Children's Anxiety Scale—Parent (SCAS-Parent) was used to measure children's anxiety levels. The SCAS-Parent is a well-established psychological questionnaire and a widely used assessment completed by parents of children and provides an overall measurement of child anxiety. Previous studies have proved good test–retest reliability and internal consistency of its psychometric properties22,23 and a fair good agreement (0.41–0.66) between the parent report and the child self-report version.24,25 It consists of 38 items and assesses six domains of anxiety that constitute six subscales, namely separation anxiety disorder, social anxiety, generalized anxiety disorder, OCD, physical injury fear, and agoraphobia. Parents were asked to rate the frequency of the anxious symptoms their children exhibit on a four-point scale with 0 = never, 1 = sometimes, 2 = often, and 3 = always. The sum of the score was used and the higher score indicated an elevated level of perceived anxiety.
Exergame programs
All participants participated in the 8-week training program with two sessions of 30 minutes per week. The exergame programs were performed using a commercially available exergame system, the UINHEALTH (UINCARE Corp., Korea), which uses a Microsoft Kinect v2 sensor to identify and track the user's body to display their image or avatar into the monitor, removing the need for a controller. Participants assigned to the CGG group and the CmGG group played the exergames in pairs that were chosen at random, and the exergames' difficulty was gradually raised following their performances. Each participant was rated separately according to their performance and the pairs matching was adjusted in case one of the partners had a lower performance with a difference >25% with the other partner in the previous session as it was conducted in a previous study. 21
Those in the CGG group were not aware of their individual score but only the group score to avoid competition between pairs. Participants allocated in the Solitary exergame group (SGG) performed the exergames alone with the level of difficulty gradually increasing after each session.
In this study, two exergames were used in each group allocation and were performed during all sessions. The CGG group played a farm protection game with two players acting as colleagues and a table tennis game with two rackets, one for each player (Fig. 2A, B), with players playing together. For the CmGG group, a basketball ball shooting and balloons boxing game with balloons of various colors (Fig. 2C, D) were used while participants compete against each other, and their score was recorded separately. The participants in the SGG group performed a car race with obstacles to avoid and a soccer striker game (Fig. 2E, F) while they played alone, and their scores reflected their performances. The UINHEALTH provided visual and audible feedback while the exergames were being played, with the words “Perfect,” “Great,” “Good,” and “Missed” shown on the screen.
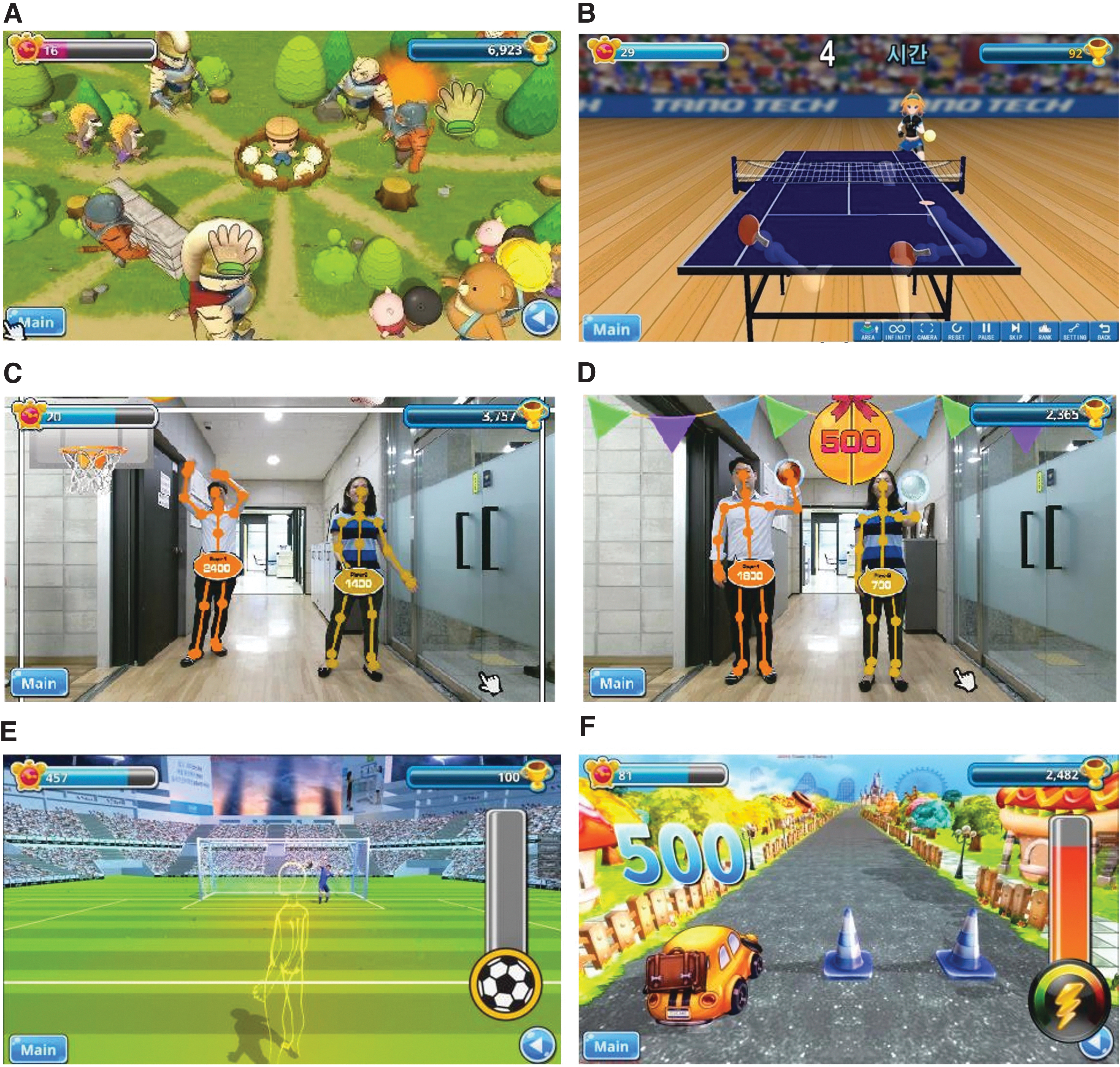
Screen images of the exergames.
All the exergames were chosen because they involve both motor and cognitive tasks and were easily monitorable. In addition to the mentioned criteria, the cooperative exergames were selected as they require solidarity between players to achieve the games and because they were found favorable for use in a previous study that assessed the feasibility of multiplayer games for children with ASD. 21
Data analysis
The SPSS statistics software version 29.0 for Windows (Armonk, NY: IBM Corporation) was used for statistical analysis. Descriptive statistics included the mean and standard deviation of all outcome measures. The normal distribution of data was confirmed using the Shapiro–Wilk test and parametric tests were used for data analyses. Paired sample t-test (two-tailed) was used to analyze the changes between the pretest and the posttest within groups and Cohen's d for t-test was calculated to determine the effect size, which is interpreted as small (d ≥ 0.2), medium (d ≥ 0.5), and large (d ≥ 0.8). 19 One-way ANOVA was performed to compare the difference between the three groups using the posttest minus pretest value. The Bonferroni was used for the post hoc test and eta square (η2) as the between-group effect size. The level of significance was set at P < 0.05.
Results
Demographic information
The demographic information of the participants is presented in Table 1. A total of 36 participants with 21 boys and 15 girls completed the exergame program without a dropout or loss of follow-up. Participants were predominantly in primary school while only two attended special education in the CGG and one in each CmGG and SGG. Most of the participants were familiar with videogames, 60% in the CGG and SGG, and 70% in the CmGG.
Participants General Information
Mean ± SD.
ADHD, Attention-deficit hyperactivity disorder; ASD, autism spectrum disorder; CGG, cooperative exergame group; CmGG, competitive exergame group; ID, Intellectual Disorder; OCD, Obsessive-Compulsive Disorder; SD, standard deviation; SGG, solitary exergame group.
Cognition
The result of the cognitive function within and between groups is given in Table 2. The within-group analysis showed a statistically significant difference in memory, attention, visual perception, and language subscales in the CGG (P < 0.05). However, no statistically significant changes were observed in orientation and high-level cognition between pretest and posttest scores (P = 0.089 and P = 0.069, respectively). The results of CmGG and SGG were similar with statistically significant differences in memory, attention, and visual perception (P < 0.05). However, both groups did not show significant improvements in orientation, language, and high-level cognition subscales (P > 0.05).
Comparison of Cognition Pre-Post Intervention Within and Between Groups
Data are expressed as mean ± SD.
P < 0.05, **P < 0.001.
Results from paired sample t-test, η2 between-group effect size.
Significant difference between CGG and SGG.
Significant difference between CmGG and SGG.
Significant difference between CGG and CmGG.
ANOVA, analysis of variance.
Regarding the between-group comparison, statistically significant differences were observed in different subscales during one-way ANOVA. First, significant differences were observed in attention between the groups (F(2,33) = 6.333, P = 0.005, η2 = 0.227), whereas the Bonferroni post hoc test revealed a difference between the CGG and SGG, and between the CmGG and SGG (P < 0.05) but without a difference between the CGG and CmGG (P > 0.05). Moreover, significant differences were observed in the language subscale (F(2,33) = 4.719, P = 0.016, η2 = 0.222) with the post hoc test showing a difference between the CGG and CmGG and between CGG and SGG (P < 0.05). No significant differences were observed between the groups in the other subscales of cognition (P > 0.05).
Anxiety
The result of the anxiety score is given in Table 3. First, in the within-group analysis, we observed a statistically significant reduction in all six anxiety subscales in the CGG (P < 0.05). In the CmGG, a significant change was only observed in the “social phobia” subscale (P = 0.034, d = 0.698), whereas the other five subscales did not present any significant changes (P > 0.05). Regarding the SGG, “physical injury fears,” “social phobia,” and “general anxiety disorder” subscales showed significant changes between the pre-and postintervention ([P = 0.046, d = 0.648]; [P = 0.044, d = 0.658]; and [P = 0.039, d = 0.677], respectively). The other subscales did not show significant differences (P > 0.05).
Comparison of Anxiety Levels Pre-Post Intervention Within and Between Groups
Data are expressed as mean ± SD.
P < 0.05.
Results from paired sample t-test, η2 between-group effect size.
Second, the between-group comparison did not show statistically significant differences in all anxiety subscales between the three groups (P > 0.05).
Discussions
This study aimed to compare the effects of cooperative, competitive, and solitary exergames on cognition and anxiety levels in children with DD. The findings highlight that memory, attention, and visual perception were significantly improved in all groups regardless of the type of the exergame, whereas language was only improved in the CGG. The findings revealed that playing cooperative and competitive exergames had more positive benefits on attention than playing solitary exergames and the only approach that had an impact on language was the cooperative exergame. In terms of anxiety, the cooperative exergames had positive effects on all anxiety subscales. Only social phobia improved in competitive exergames, whereas physical injury, social phobia, and general anxiety fear improved in solitary exergames.
In this study, all types of exergames positively impacted memory, attention, and visual perception. This can be explained by the fact that exergames combine physical and mental tasks that may stimulate various parts of the brain with a larger demand for neuronal activity and may result in high levels of neural plasticity (structural and functional adaptations of the brain). In addition, participating in exergames requires mental processes such as imagination, thinking, and emotion that may increase synaptogenesis resulting in an improvement of various aspects of cognition. Similar results were found in previous studies that used exergames and confirmed improvements in memory, attention,11,26 and visuospatial processing. 27
Of interest, in this study, cooperative and competitive exergames had higher effects on attention compared with solitary exergames. The nature and the content of the exergames may be the principal reason. Children in the cooperative exergames needed to pay attention to their performance in addition to their partners to successfully complete the exergames. On the contrary, those who played the Competitive exergame required a high among of attention to compete and try to win the game over their opponents. However, those with solitary exergames may have less attention demand that may be limited to the performance of the ongoing exergame.
Cooperative exergames were the unique exergame type that positively impacted the language subscale. According to these results, children who played cooperative exergames were more socially engaged and required more verbal communication to win the game than those who played competitive or solitary exergames. This explanation is supported by a previous study that affirmed active participation in exergames with players discussing, which may help to promote language skills. 28
Regarding anxiety, promising improvements were observed during cooperative exergames. It is important to mention that cooperative exergames selected for this study included tasks that required reciprocal communication and teamwork that might reduce the feeling of fear, worry, panic, and nervousness among the children. Wang et al. 29 reported that active participation in socially engaged activities motivates reciprocal support that enhances psychological safety and reduces the symptoms of anxiety.
On the contrary, the competitive exergames did not show positive effects on anxiety subscales expecting for the social phobia subscale. Engaging in competitive activity may be challenging and stimulating that may increase mental pressure, lack of self-esteem and self-confidence among children with DD and may lead to a negative impact on mental health and anxiety.
In this study, solitary exergames showed improvements in physical injury fears, social phobia, and general anxiety disorder. Playing exergames alone required less social interaction, less fear of failure, and less stress. This situation may be explained by the fact that children are more capable of controlling their environment and their performance independently of another individual. In addition, they felt less psychological pressure as they played the game without concern for other players, at their own pace, and just paying attention to their own aims without worrying about being criticized or falling short of others.
Study strengths and implications
This study presents some strengths and implications. First, a randomized controlled trial was used with three groups to evaluate how various game kinds may affect children with DD in terms of cognition and anxiety levels while minimizing the possibility of selection bias. Second, all the sessions were performed separately with participants blinded to types of exergames played by the other groups to reduce performance bias. Moreover, it is important to mention that there was no loss to follow-up among the participants and they attended all sessions. Finally, the program lasted 8 weeks with 16 sessions that may be considered sufficient to compare the effects of the different types of exergames. 30
For health practitioners, our study shows the effects of different types of exergames in children with DD and offers a guide to choose the appropriate type of exergame to use in their practice with found results. For the research community, our results are important because they contribute to the knowledge of using exergames in children with DD by providing evidence that all types of exergames may effectively increase some domains of cognitive function (memory, attention, and visual perception). Furthermore, it also showed that cooperative exergames may have more impact on anxiety levels in children with DD compared with the other types of exergames. This may generate new interest in exergames that may lead to further research on the topic.
Study limitations and future research suggestions
Despite all the above strengths, this study also has some limitations. First, even knowing that all participants attended school and their educational levels were indicated, we could not properly measure their intellectual levels, which may limit the generalization of our findings. Second, although the sample size was calculated to have an effect size (f) of 0.4 with power (1 − β) of 95%, a large number of participants would have been better to lower the standard of deviations. Many participants could not be included in this study owing to the COVID-19 pandemic. Moreover, a long-term follow-up should be studied to evaluate the continuity of the program.
Conclusion
This study aimed to compare the effects of cooperative, competitive, and solitary exergames on cognition and anxiety levels in children with DD. The results suggest that all types of exergames may be used to improve cognitive function especially memory, attention, and visual perception, whereas only cooperative exergames may improve verbal communication. Moreover, cooperative and competitive exergames may be used to effectively improve attention compared with solitary exergames. Regarding anxiety, cooperative exergames are more effective followed by solitary exergames, whereas competitive exergames may have a limited impact on children with DD. Therefore, the type of exergames should be chosen carefully according to the child's needs and conditions.
Footnotes
Acknowledgment
The authors thank all participants who participated in the experiments and made possible the completion of this study.
Authors' Contributions
D.M.N.: conceptualization (lead), methodology (lead), writing—original draft (lead), review and editing (lead). H.-Y.K.: investigation (lead), formal analysis (supporting), writing—original draft (supporting). J.-W.L.: investigation (supporting), formal analysis (supporting), writing—original draft (supporting). S.-Y.O.: investigation (supporting), formal analysis (lead). J.-H.Y.: conceptualization (supporting), methodology (supporting), writing—review and editing (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Culture, Sports and Tourism R&D Program through the Korea Creative Content Agency grant funded by the Ministry of Culture, Sports and Tourism in 2022 (Project No.: SR202106002).