
Abstract
Background:
A variety of surgical techniques have been described to address nasal obstruction related to internal nasal valve insufficiency. The internal nasal valve is defined as the angle between the caudal border of the upper lateral cartilage the septum, and the head of the inferior turbinate. Correction of nasal valve obstruction generally involves addressing these anatomical boundaries with grafts, sutures, excision, radiofrequency ablation, or implants. 1 Determining the most appropriate surgical approach requires assessment of individual nasal anatomy as well as consideration of overall surgical goals. Here we demonstrate the use of the Lopez-Infante flap to directly address the caudal upper lateral cartilage. This technique is attributed to Dr. Fausto Lopez-Infante of Mexico City and is not widely described in existing literature. 2
Objective:
To demonstrate the Lopez-Infante flap for management of internal nasal valve collapse.
Methods:
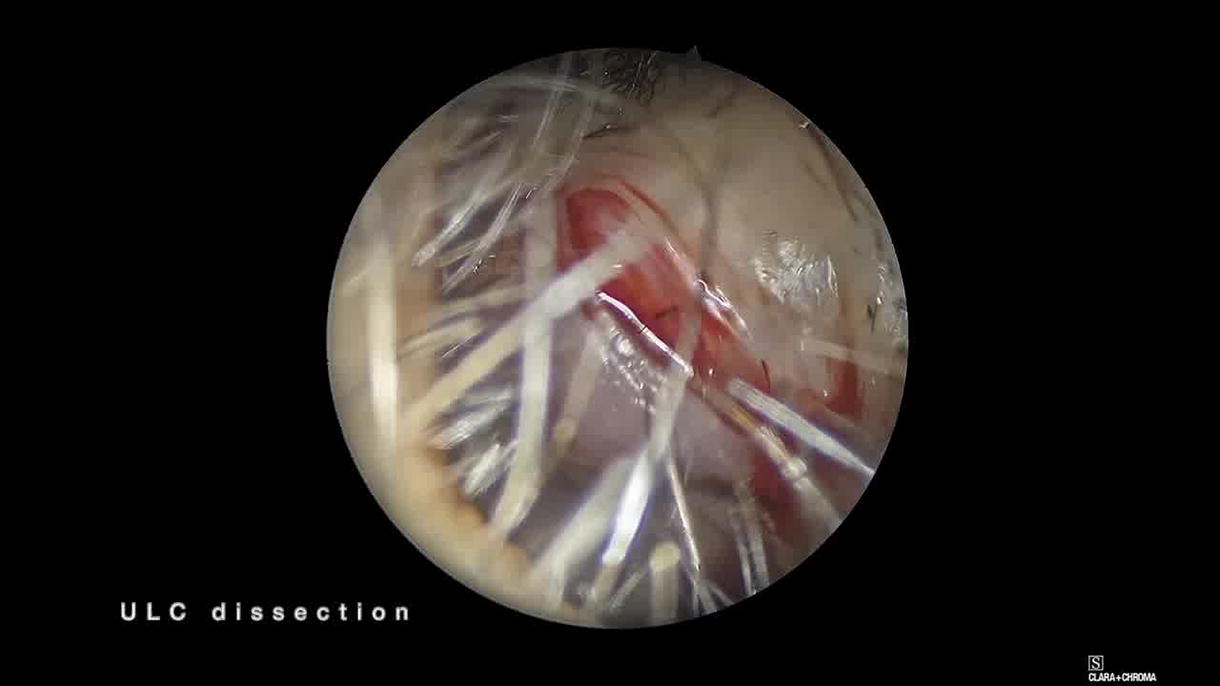
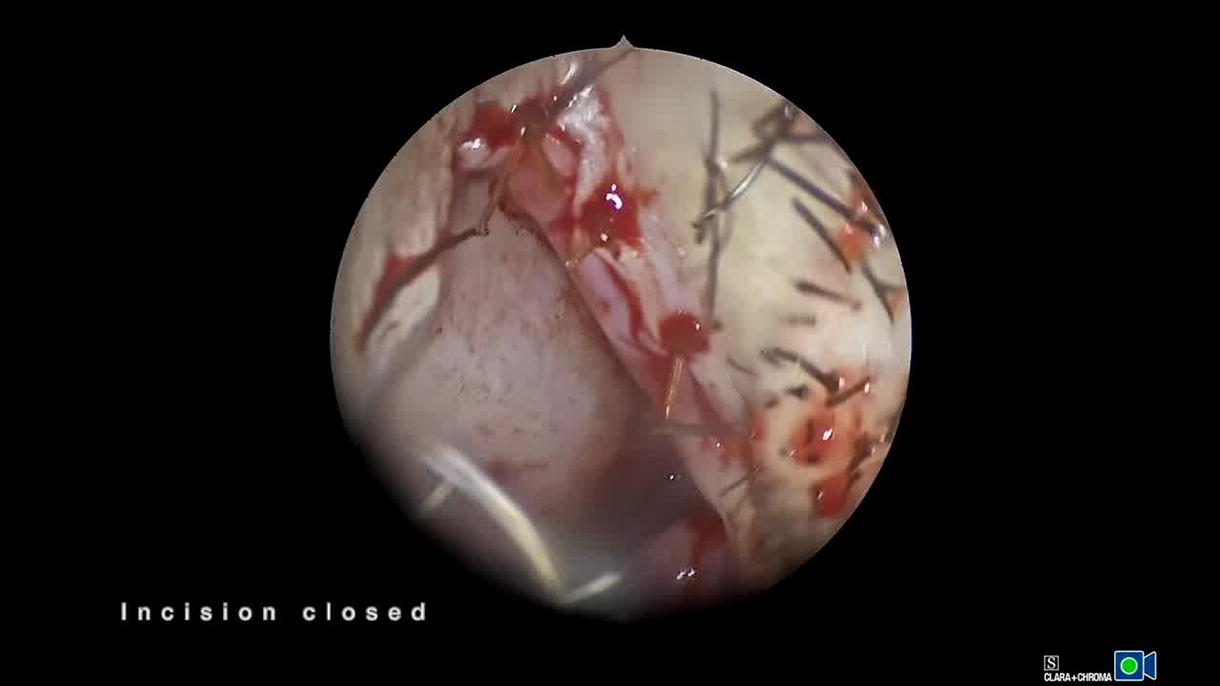
The video shows a patient undergoing Lopez-Infante flap. After injection of local anesthetic with epinephrine off the field, an intercartilaginous incision is made. The caudal edge of the upper lateral cartilage is dissected from surrounding mucosa using a combination of sharp and blunt dissection. Once the cartilage is adequately exposed, a 2–3 mm strip is excised from the caudal border. Mucosa from the cephalic edge of the incision is reflected caudally. The excess mucosa is trimmed and the incision is closed with absorbable suture.
Results:
The Lopez-Infante flap results in a wider internal nasal valve by eliminating redundant caudal upper lateral cartilage and mucosa. This technique is best suited for elongated upper lateral cartilage that is impinging on the internal valve at rest. Postoperative scar formation in this area further enforces the valve. This technique can be performed awake in the office or under general anesthesia as part of a functional nasal surgery. There is a risk of nasal tip rotation as well as alar malposition and retraction with over resection of the upper lateral cartilage. For this reason, this technique may be best suited for an under rotated tip and should be performed prior to additional planned tip work. A similar patient underwent Lopez-Infante flap in combination with septoplasty and inferior turbinate reduction. Preoperative SCHNOS score was 22. Six month postoperative SCHNOS was 1. There was no alar retraction or tip rotation noted at follow-up.
Conclusion:
The Lopez-Infante flap is a useful tool to address nasal valve insufficiency. This video demonstrates the technique, which can be performed awake in office or as a component of functional septorhinoplasty under general anesthesia. The result is widening of the internal nasal valve angle and larger valve area.
Funding Statement:
No funding was received.
Contribution:
Morgan Lee MD: Article preparation, video editing. Sunthosh Sivam MD: Supervision, conceptualization, article review and editing.
Ethics Approval:
No identifiable patient information is included in this submission.
Disclosure Statement:
The authors have no relevant disclosures or conflicts of interest to report. No competing financial interests exist.
Runtime of video: 1 min.
Get full access to this article
View all access options for this article.