
Abstract
Introduction:
Cleft palate is a common congenital condition, affecting approximately 1 in 1700 births globally. 1 Despite advancements in surgical techniques, postpalatoplasty complications like velopharyngeal insufficiency (VPI) often persist. 2 VPI occurs owing to inadequate function of the velum and the lateral or posterior pharyngeal walls, and it manifests as hypernasality, nasal emission, and facial grimacing, affecting speech and quality of life. 3 The posterior pharyngeal flap (PPF), dating back to 1865, remains a cornerstone treatment for VPI, particularly when nasopharyngoscopy reveals dynamic lateral wall movement. 4 Despite multiple iterations of this technique, the Hogan modification has been the most widely accepted approach. 5,6 This video abstract presents the Hogan modification of the PPF, a widely adopted approach to treat VPI.
Materials and Methods:
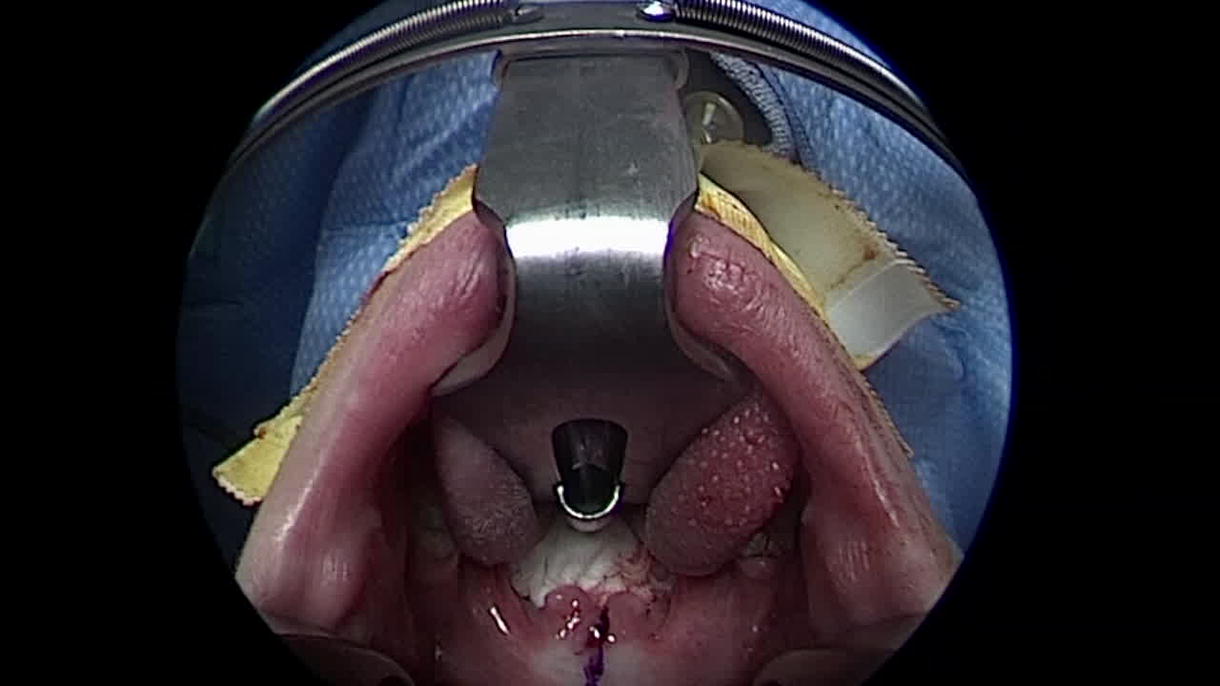
With informed consent, the Hogan-style PPF procedure was recorded on a 6-year-old male with VPI and bifid uvula. The surgery was recorded using an endoscopic camera, ensuring a comprehensive visual guide to the technique.
Results:
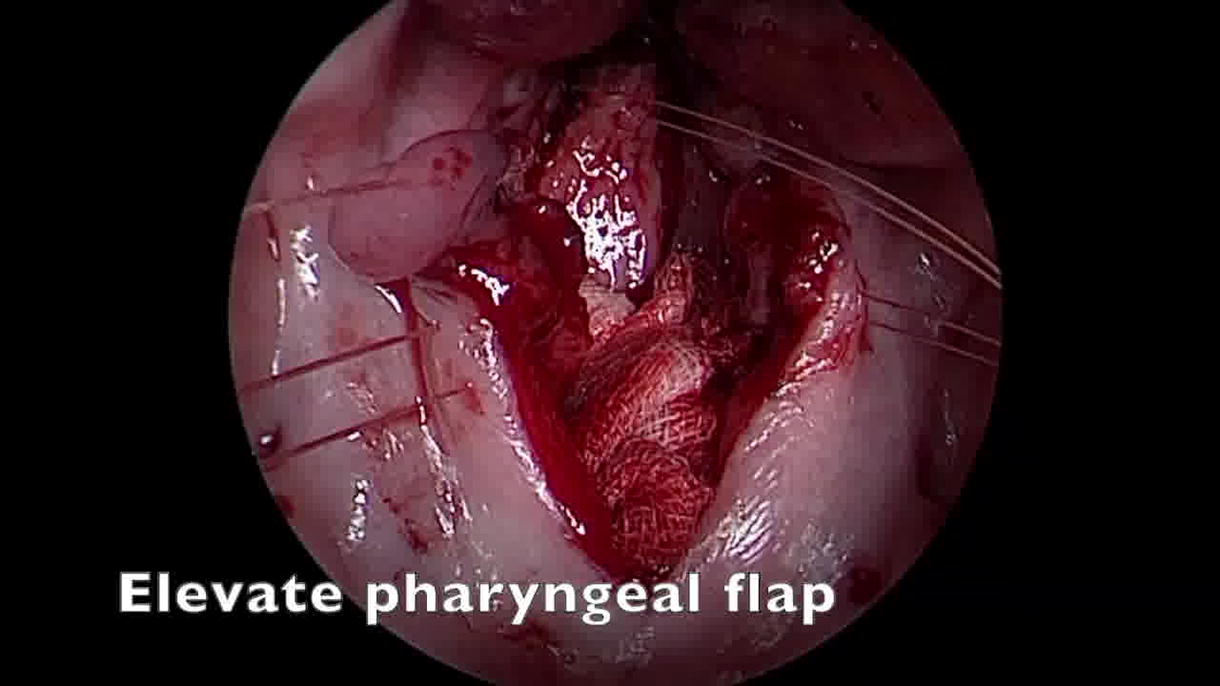
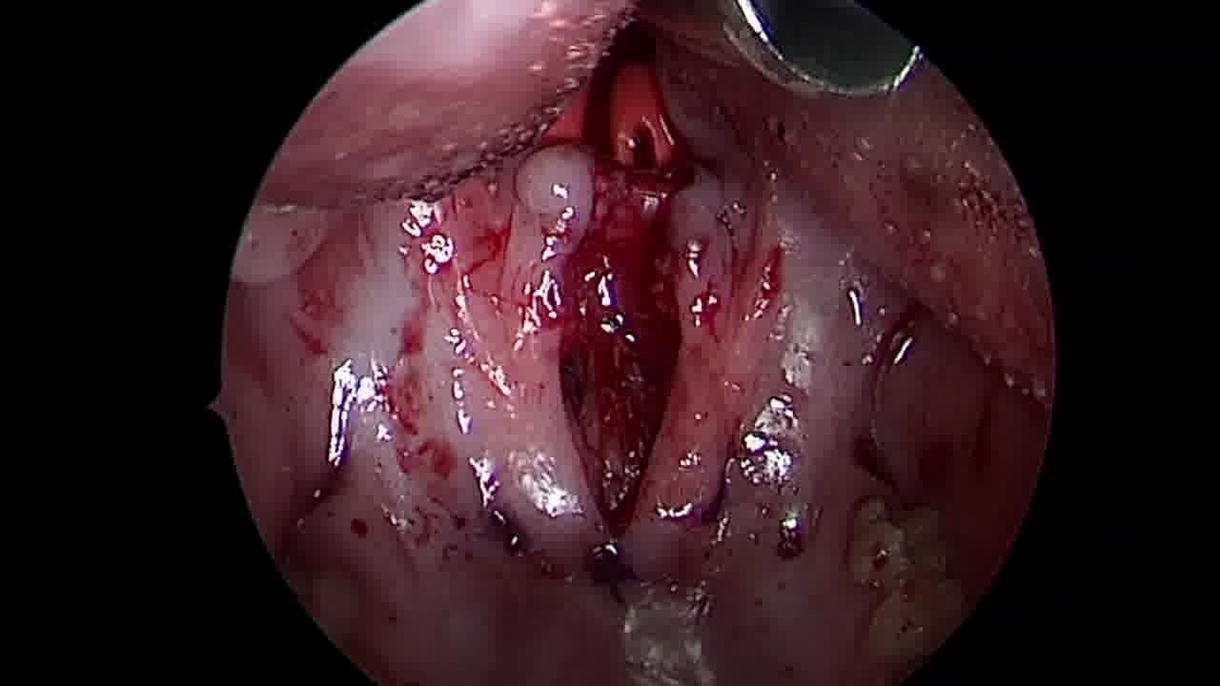
Beginning with the division of the velum, the procedure includes dissecting nasal lining flaps and retracting them laterally. This is followed by marking and elevating a 15–20 mm wide superiorly based PPF from the inferior pharyngeal wall up to the level of the first cervical vertebra (C1), situated above the palate. The flap donor site mucosa is closed primarily, and 14 French red rubber catheters are inserted to establish two velopharyngeal ports adjacent to the PPF. The PPF is then sutured to the nasal mucosa with mattress sutures, followed by suturing the lining flaps to the PPF’s posterior wall and edge, concluding with velum closure. Other flap inset alternatives include the fish mouth or mail slot approach.
Conclusions:
This video abstract highlights the importance of precise surgical technique to maximize patient outcomes and minimize complications. Surgeons must approach this procedure with caution, especially in patients with obstructive sleep apnea (OSA) and those with 22q11.2 deletion syndrome owing to the risk of medialized carotids. 7 In patients with adenoid hypertrophy, tonsillectomy is recommended before PPF surgery. 8 Postoperatively, early snoring is expected, and a nasopharyngeal airway may be left in place. Most patients experience improvement in nasal resonance and speech, although a secondary speech surgery is necessary for about 9% and 4% may develop OSA. 9 Notably, the division of PPFs owing to OSA has not been demonstrated to have a detrimental effect on speech. 10 In conclusion, PPF is an effective secondary procedure for enhancing speech in patients with VPI. Surgeons must be adept at addressing the nuances and potential complications associated with changing nasal airflow.
Christopher M. Runyan, MD, PhD is a consultant for KLS Martin.
Runtime of video: 4 mins 6 secs
Source of Study:
The source of this study was a 6-year-old male with VPI and bifid uvula who underwent the Hogan-style posterior pharyngeal flap procedure. There were no conflicts of interest resulting from the source of this study.
Institutional Board Approval:
The participant in this study provided written informed consent to accessing their intraoperative video, imaging, or other identifying characteristics in this review. This review was also approved by the Institutional Review Board at Atrium Health Wake Forest Baptist (IRB00052044).
Get full access to this article
View all access options for this article.