
Abstract

Introduction:
Osteomas are benign bony lesions and the most common tumors of the facial skeleton and calvaria. 1 They can present with symptoms of facial pain, headaches, and facial deformity. 1 Definitive management is surgical excision. When located on the forehead, traditional approaches to consider include the coronal, midforehead, or pretrichial incisions. 2,3 Despite excellent access, these methods can be associated with scar widening, alopecia, hypesthesia posterior to the incision, and blood loss. 2,3 Minimally invasive approaches that use smaller incisions in locations easier to camouflage are the preferred approach for many aesthetic procedures of the forehead. 4 An incision made in the scalp can be utilized to access the lower forehead. Dissection and visualization are achieved using endoscopic forehead retractors and curved periosteal elevators that allow for the maintenance of an optical cavity. 2,5 The following case illustrates the steps used to excise an osteoma of the forehead, demonstrating how aesthetic techniques were applied.
Methods:
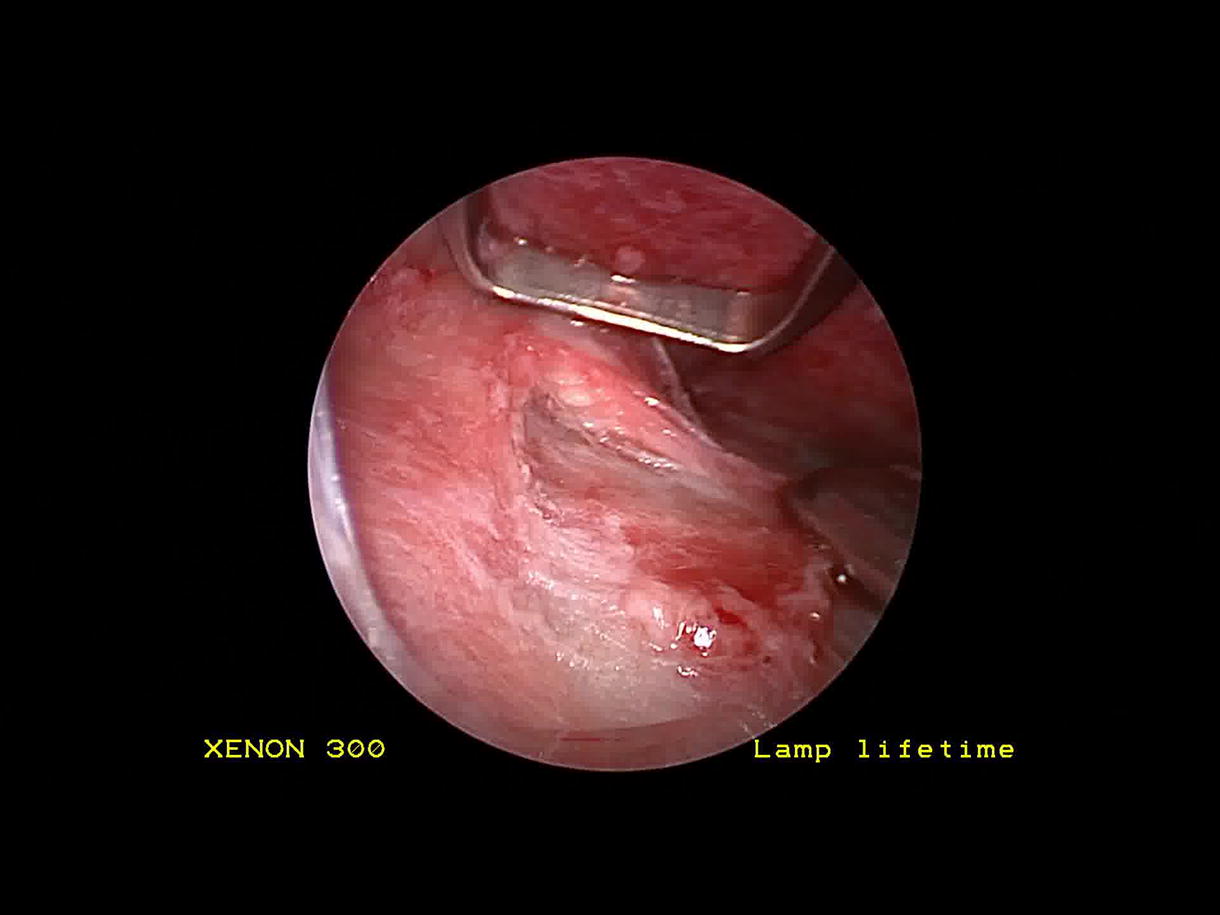
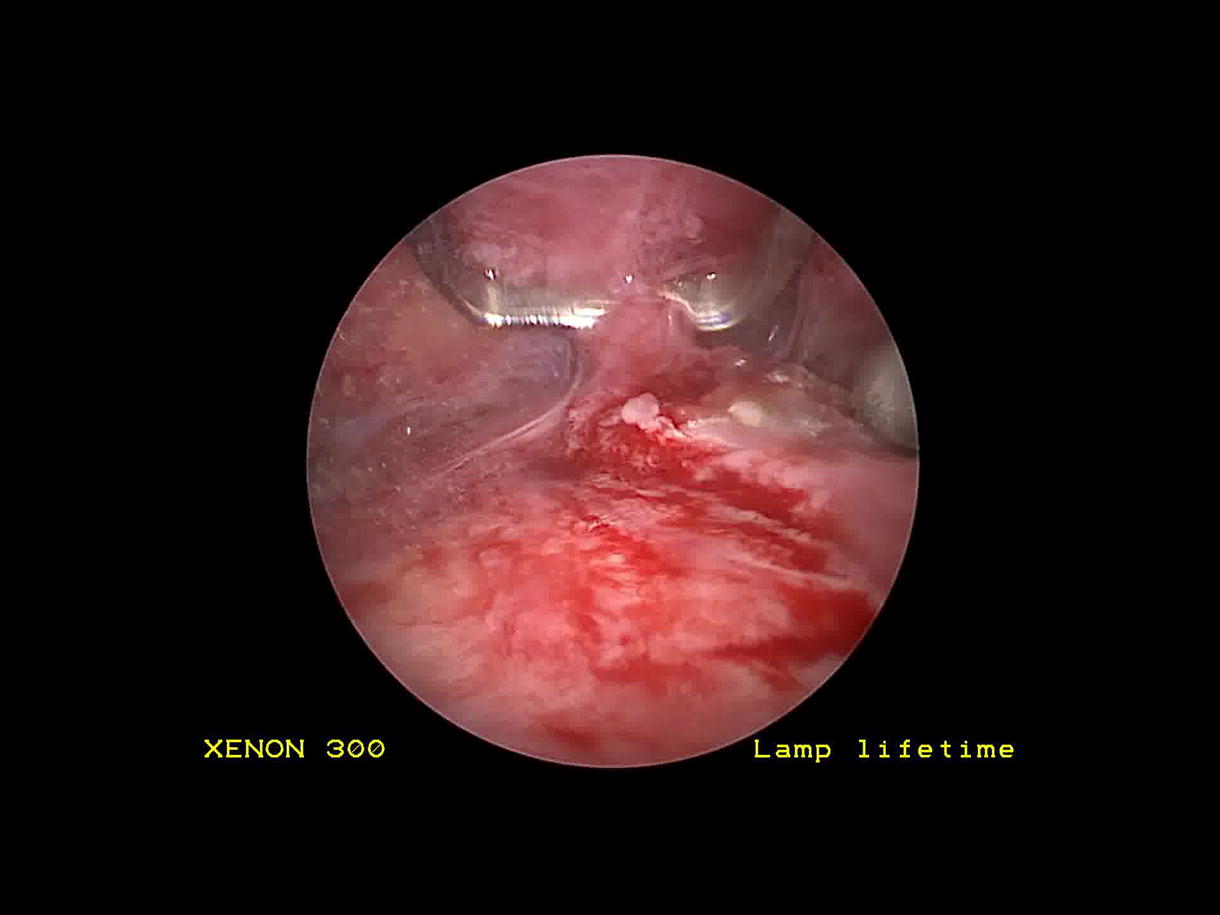
The video demonstrates a case of endoscopic excision of a forehead osteoma in a 26-year-old man. The patient presented with an eight month history of a forehead lesion, measuring 1.2 cm and positioned 1.5 cm above the left lateral eyebrow. The patient was interested in surgical removal with concern for cosmesis. In the operating room, a left paramedian incision was made 1 cm behind the hairline, and a second scalp incision was made at the lateral border of the frontalis muscle. The incisions were made down to and through the pericranium to allow for pericranial elevation. The endoscopic elevator was inserted through the paramedian incision, and the periosteal elevator was placed through the lateral incision to dissect the forehead in the subperiosteal plane. The osteoma was identified, and a 4 mm osteotome was used to remove the lesion followed by 4 mm cutting and diamond burs to smooth the edges of the residual bone. The scalp incisions were closed in layers and a pressure dressing was applied.
Results:
At the 1-week postoperative visit, the patient’s left forehead was flat, smooth, and non-tender, which was stable at the 2-month follow-up. Scalp incisions showed no alopecia.
Conclusion:
In the era of minimally invasive approaches for surgery of the face, endoscopic-assisted techniques have an important role. The endoscopic technique avoids visible scaring, and compared with other forehead approaches, decreases the length of incisions, and the total amount of tissue dissection. These features of the procedure lead to high levels of patient satisfaction. There is also a safety benefit provided by the superior location of the incisions given the proximity of the lesion to the region of the brow where the temporal branch of the facial nerve enters the frontalis muscle. Discrete incisions, minimal blood loss, and rapid recovery times make the endoscopic approach to the forehead a worthy tool in the surgeon’s armamentarium. Proper preoperative workup will guide the selection of the right candidate for minimally invasive approaches, and if endoscopically assisted forehead approaches are not feasible, alternative incision types should be employed.
Source of work and study:
The video was obtained and edited at State University of New York Downstate Medical Center.
CRediT Author Statement:
T.S.: Data curation, investigation, Visualization, Writing—original draft, Writing—review and editing. R.T.: Data curation, Investigation, Software, and Visualization. H.J.: Investigation, Validation, Writing—review and editing. K.L.: Investigation, Resources, Visualization. S.C.B.: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing—review and editing.
No competing financial interests exist
.
No funding was received for this article
.
Runtime of video: 3 mins and 42 secs
IRB/Ethics Approval: The study was deemed exempt from formal review by the SUNY Downstate IRB. Informed consent was obtained from this patient for inclusion in education material such as this.
Get full access to this article
View all access options for this article.