
Abstract
Introduction:
Sterno-omohyoid free flap has been described as an option for dual-vector, dual-innervation facial reanimation by Vincent et al. 1 Sterno-omohyoid flap can more closely resemble the mimetic muscles of the face because of its small size and fast-twitch muscle fibers when compared to the gracilis. The sternohyoid and omohyoid are separate muscles, allowing for dual-vector reanimation. Innervation by the ansa cervicalis arcade allows a long nerve graft with two end-to-end neural anastomoses.
Materials and Methods:
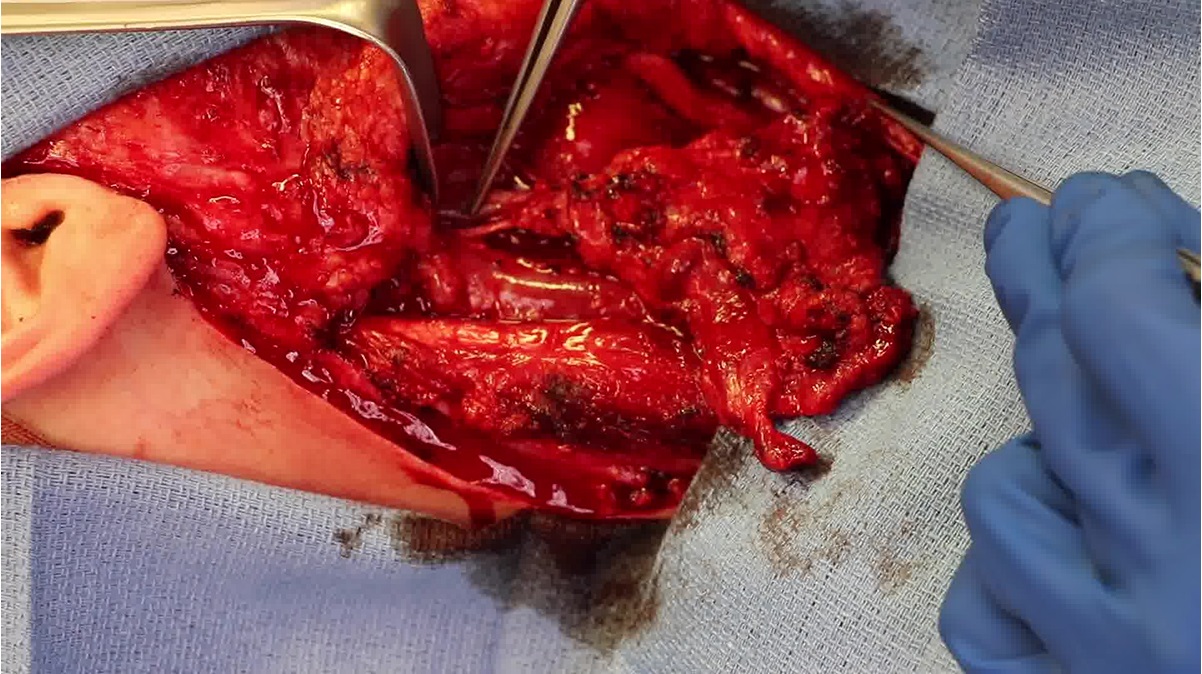
What follows is a case report of an adult undergoing sterno-omohyoid free flap used in dual-vector, dual-innervation with cross facial nerve graft (CFNG) and masseteric nerve for smile reanimation. The patient is a 36-year-old with long-standing facial paralysis from traumatic brain injury. The patient had previously undergone a temporalis tendon transfer and VII–XII nerve transfer over 10 years ago achieving some tone but an unsatisfactory smile. The patient underwent a CFNG 9 months before the sterno-omohyoid free flap. During harvest, the arterial pedicle was the superior thyroid artery and two venous outflow tracts were identified: venae comitans and middle thyroid vein. The flap's weight was 20 g; the sternohyoid flap measured 9.5 cm in length when on tension in the neck and 6 cm after harvest and the omohyoid flap measured 9 cm at harvest and 7 cm after harvest. Intraoperative electric stimulation of ansa hypoglossi generated more robust contraction of the omohyoid and sternohyoid than ansa cervicalis. The ansa hypoglossi was therefore connected to the masseteric nerve and ansa cervicalis to the CFNG. The omohyoid functioned as the medial vector to the upper lip and sternohyoid as the lateral vector to the modiolus. The superior thyroid artery was connected to the superficial temporal artery, venae comitans to superficial temporal vein, and middle thyroid vein to facial vein for additional venous outflow.
Results:
The patient recovered well postoperatively. Facial movement was assessed, and video recorded at the 4-month postoperative visit. As shown, he has good movement of the lips with smile including good lateral excursion at the modiolus, upper lip elevation, and nasolabial fold creation.
Discussion:
Advantages of the sterno-omohyoid free flap include providing two vectors for smile reanimation and improved dental show with minimal bulk. Dissection within the muscle, as done in the gracilis free muscle transfer, is not necessary when using the sterno-omohyoid flap. However, the perforator vessels to the strap muscles are small, and consistent reliability of the blood supply is a potential concern for this free flap. Finally, creating additional vectors (beyond two) with the free strap muscles is more difficult than when using the gracilis free muscle flap.
Conclusions:
Sterno-omohyoid free flap is a viable alternative to the gracilis free flap for dual-vector, dual-innervation facial reanimation. This video provides a helpful visual aid for those adopting this free flap in their practice, with movement results at 4 months postoperatively.
The authors involved in this video have no relevant financial disclosures related to the material herein.
The source of work or study, and if there are any conflicts of interest or obligations resulting from it.
Ethics Approval and Patient Consent Statements: The patient whose recording and information appears in this video has signed both an authorization to use and disclose protected health information and a media release consent form.
Runtime of video: 5 mins 25 secs

Get full access to this article
View all access options for this article.