
Abstract
Introduction:
Nasal septal perforation, marked by symptoms such as whistling breathing, crusting, and nasal obstruction, significantly impacts patients' quality of life. A range of repair techniques exist, including septal buttons, advancement flaps, and open approaches with grafts, 1 –5 reflecting success rates between 30% and 90%. 6 –8 Given this diversity, personalized selection based on patient history and surgeon preference is essential.
Materials and Methods:
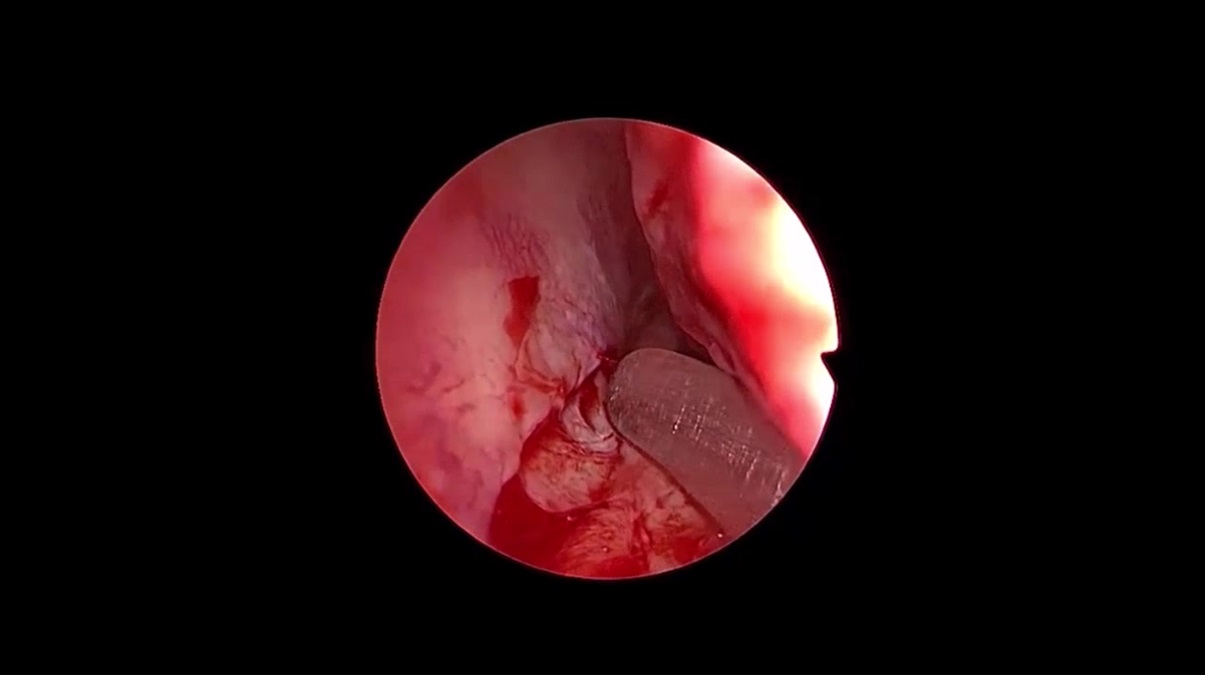
In this case study, we detail a patient with postoperative septal perforation who underwent bilateral upper blepharoplasty. The patient was mildly affected by the septal perforation and the primary complaint was occasional whistling. There was no notable crusting and the patient requested for a blepharoplasty. Otherwise unplanned and unrequested nasal septal perforation seemed eligible because of the subsequent blepharoplasty and resultant skin graft. We concurrently addressed the perforation using a unique strategy involving a unilateral rotational mucosal flap and contralateral skin graft. The patient was informed and provided consent for both the procedure and subsequent publication, with anonymity preserved. After upper blepharoplasty, wet-gauze-covered skin grafts were applied. Endoscopic measurements confirmed a 6 × 3 mm perforation without cartilaginous involvement. We chose the right side for a mucosal advancement flap and the left side for skin grafting due to ergonomic considerations for right-handed surgeons. For the advancement flap, an incision beneath the inferior turbinate was made, extending anteriorly a few millimeters from the perforation. Elevating a mucoperiosteal and mucoperichondrial flap, we incised the perforation margin circumferentially before suturing the nasal floor advancement flap on the right. On the left, perichondrium covered the perforation, offering vascularity to nourish the skin graft. A 10 × 5 mm skin graft was endoscopically sutured to the left side using 6/0 absorbable sutures. A comprehensive surgical demonstration is available in the accompanying video.
Results:
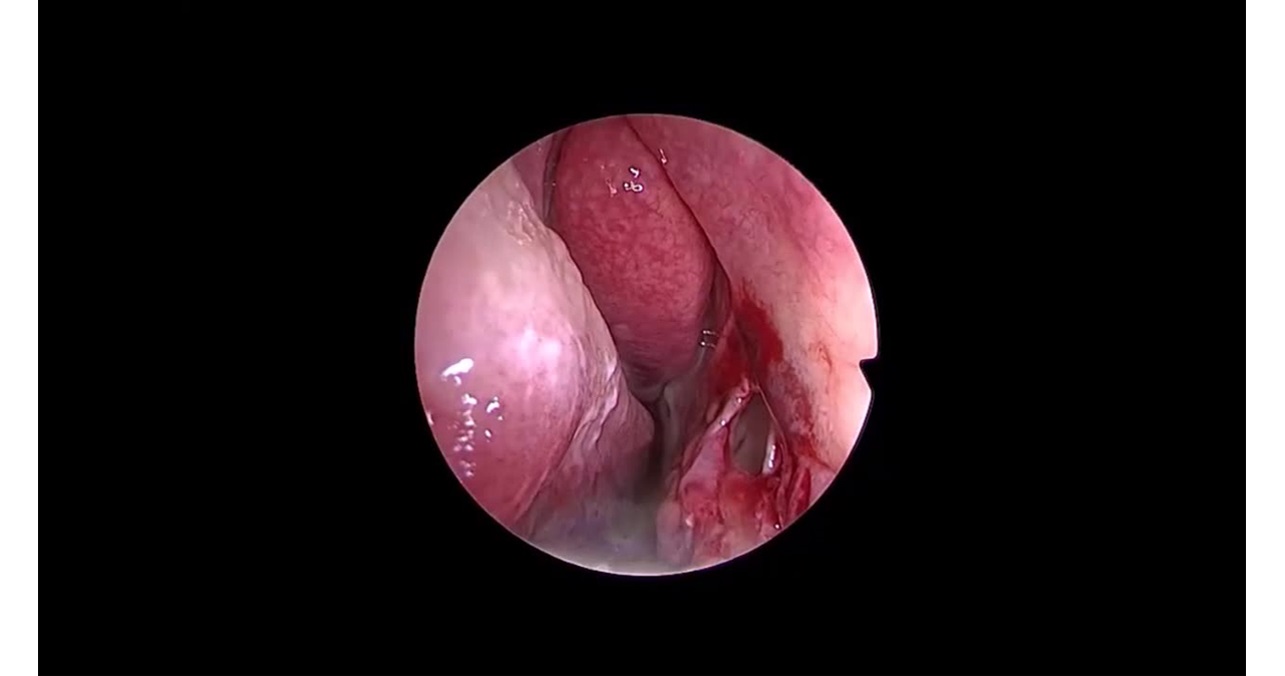
Doyle splints were placed bilaterally in the nostrils for 2 weeks, removed at the end of the second postoperative week. The mucosal flap harvest site exhibited near-complete mucosalization, remaining viable. The skin graft displayed vitality and vascularization. During recovery, the patient adhered to topical ointments and nasal irrigation, avoiding smoking. The closure was confirmed as successful on the first postoperative month examination. Six-month postoperative examination revealed complete mucosalization in the right nasal cavity including the nasal floor. Minimal crusting was observed at the donor site. On the left side, the patient exhibited a vascular and moist epithelial lining with minimal crusting, which could be easily debrided. The patient-reported improvements in nasal breathing and whistling had ceased.
Conclusions:
Our unique approach of combining contralateral skin grafting with a unilateral rotational mucosal flap for nasal septal perforation repair presents a novel contribution not found in the existing English literature. This distinct case enriches surgical decision making for septal perforation repair, yet comprehensive evaluation necessitates extended follow-ups and a broader patient cohort.
Acknowledgments:
I would cordially thank our residents and hospital staff for their collaboration in patient care.
No competing financial interests exist
.
No funding was received for this article.

Get full access to this article
View all access options for this article.