
Abstract

Introduction
Facial suspension threads (FSTs) are a novel approach in reconstructive surgery for addressing ectropion by repositioning the eyelid. This study investigates the efficacy of FSTs as a novel intervention to improve eyelid positioning and coverage in patients with ectropion secondary to facial palsy.1–4
Material and Methods
Study design
This retrospective case series encompassed patients diagnosed with ectropion due to facial palsy who underwent FST implantation. Inclusion criteria dictated the presence of ectropion due to facial paralysis, whereas exclusion criteria eliminated healthy individuals and those necessitating adjunctive surgical procedures. All participants provided informed consent prior to the intervention, conforming to local ethical standards, as a centralized Institutional Review Board is not operational in Georgia. The FST utilized in this study comprises nonabsorbable polypropylene, specifically designed to deliver sustained support for the eyelid. Outcomes were quantitatively assessed using the degree of ectropion and lower eyelid retraction (DELER) and the Periorbital Aesthetic Improvement Scale (PAIS) by three independent raters, both pre- and postoperatively. 5 DELER was assessed on a 5-point Likert scale: 0 = no retraction, 1 = mild (<1 mm scleral show), 2 = moderate (>2 mm scleral show), 3 = severe (>3 mm scleral show, >1 mm tarsal detachment), 4 = very severe (>5 mm scleral show, >3 mm tarsal detachment). PAIS was rated by an expert on a 5-point Likert scale: 1 = “Much worse,” 2 = “Worse,” 3 = “No change,” 4 = “Improved,” and 5 = “Much improved.”
Surgical technique
A subtarsal incision was executed across the lower eyelid, followed by blunt dissection in the sub-orbicularis oculi plane until the arcus marginalis was reached. The spacer was then introduced into the preseptal space and affixed with 6.0 Proline sutures to both the middle lamella of the tarsus and the periosteum of the inferior orbital rim, ensuring dual anchorage for optimal eyelid elevation and support. 5 Intentional overcorrection was performed to achieve a lower eyelid margin that covered the inferior limbus by a minimum of 2 mm (Figs. 1 and 2).
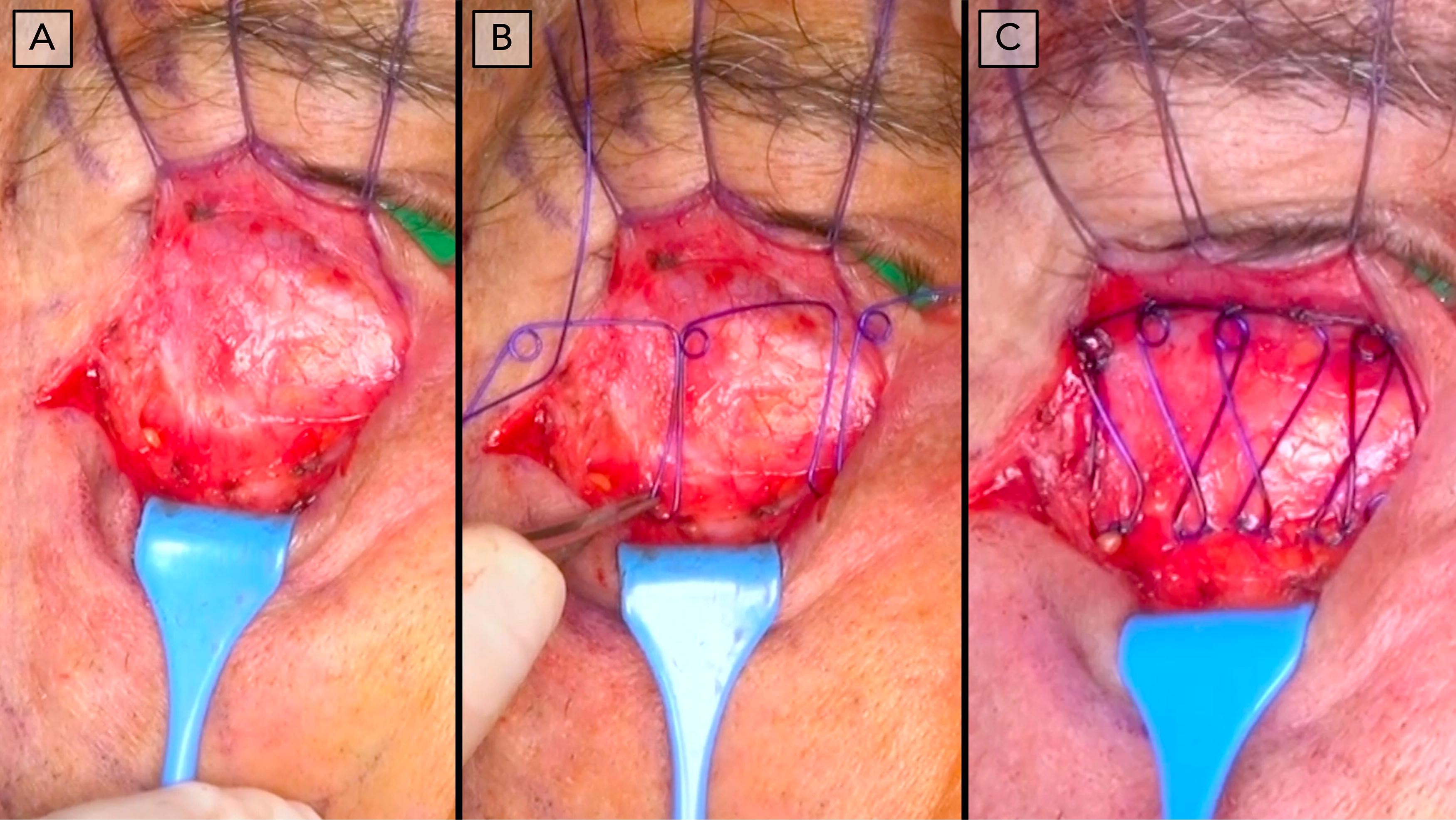
Intraoperative image series showing the placement and fixation of the FST in the right lower eyelid in a 72-year-old male patient. The FST is positioned within the preseptal space and is fixated to the inferior tarsal plane and to the arcus marginalis with sutures. FST, facial suspension thread.
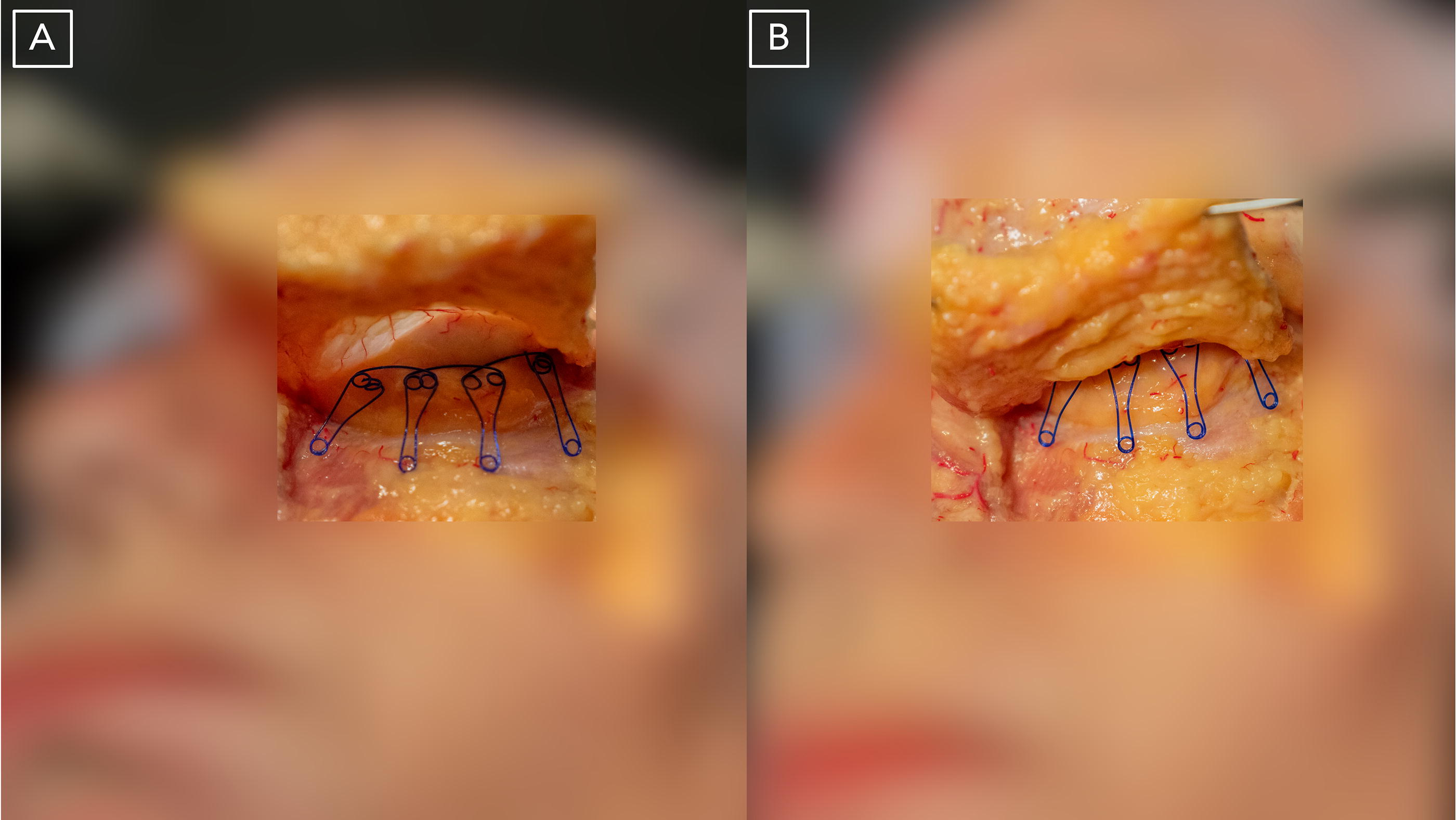
Photographs of a cadaveric specimen showing the anatomical relationship of FST placement as performed in this study: The FST is placed within the preseptal space below the orbicularis oculi muscle
Results
The cohort comprised 14 patients, with a mean follow-up duration of 8.5 months. Significant improvements in median scores were observed, indicating favorable aesthetic outcomes (Fig. 3; Table 1).
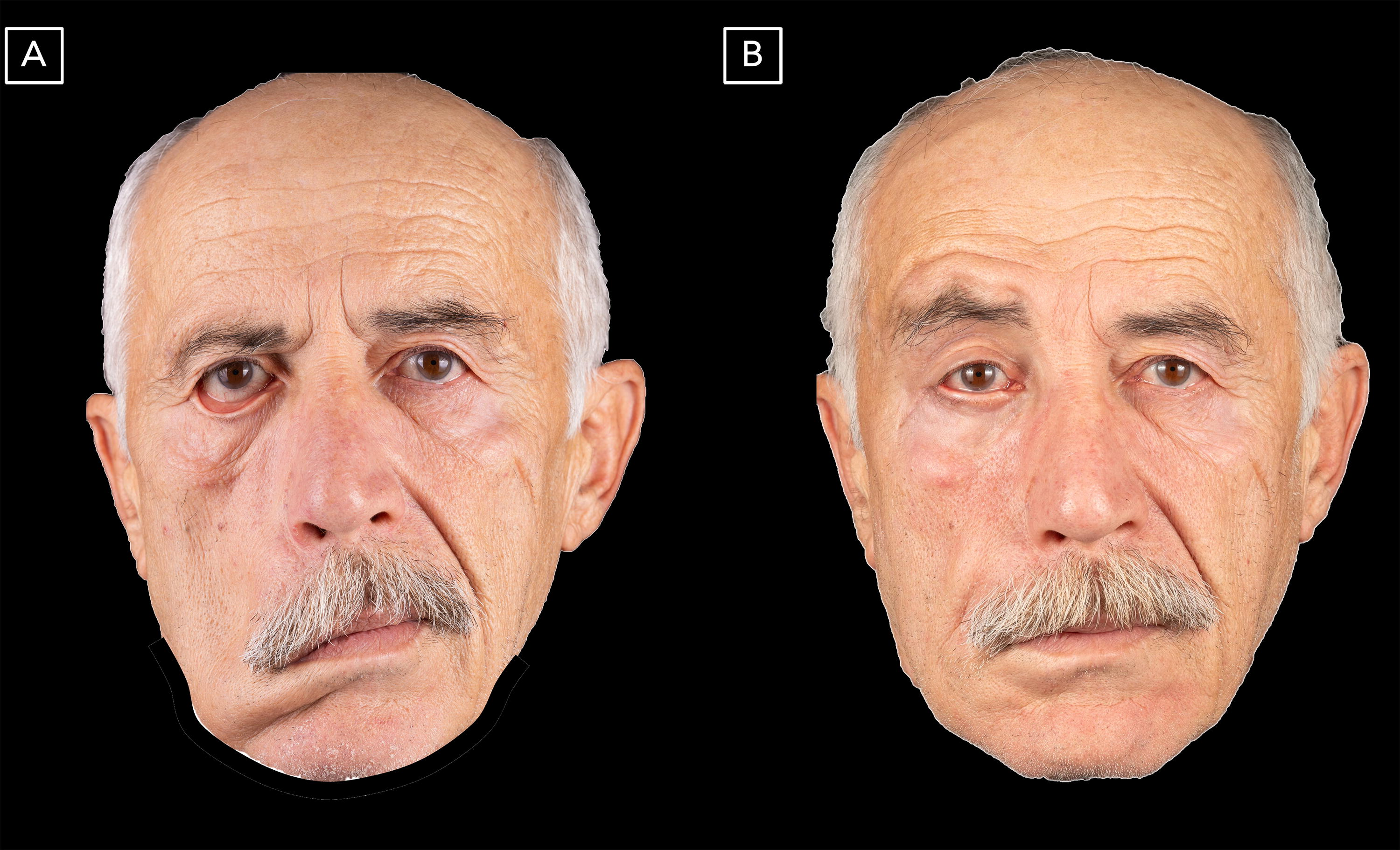
Photographs of a 65-year-old male patient with facial palsy before
Summary of patient demographics as well as pre- and postoperative outcome parameters (DELER and PAIS)
*Indicates statistical significance.
DELER, degree of ectropion and lower eyelid retraction; IQR, interquartile range; PAIS, Periorbital Aesthetic Improvement Scale; SD, standard deviation.
Discussion
The application of FST in the management of facial palsy-related ectropion demonstrates promising efficacy as an innovative surgical intervention. The findings indicate satisfactory restoration of eyelid height, accompanied by minimal adverse events. Future investigations should prioritize the implementation of standardized assessment tools to rigorously evaluate clinical outcomes. Although the follow-up duration is adequate for preliminary assessments, extended longitudinal studies are essential to determine the durability of FST in maintaining eyelid support. The capacity to customize the fixation points of the spacer facilitates individualized treatment tailored to patient-specific anatomical variations. Notably, while there exists a learning curve associated with the procedure, it can be executed safely with appropriate surgical training. A key limitation of our study is the relatively short follow-up period and the absence of validated objective outcome assessment tools, which should be addressed in future research through the use of standardized assessment methods and extended follow-up durations to ensure more robust findings.
Conclusion
This study provides initial evidence that FST represents a viable surgical option in the management of ectropion secondary to facial palsy. While the preliminary findings are encouraging, further research is warranted to establish long-term efficacy and to refine the procedural techniques involved.
Footnotes
Authors’ Contributions
Conceptualization: M.S., G.S., K.S., and M.T. developed research goals and study concepts. Methodology: K.S., M.T., and S.C. led methodology design and model creation, with M.T. refining approaches. Formal analysis: S.C., M.T., and M.A. conducted statistical and computational analyses. Investigation: G.S., K.S., and M.S. performed experiments and data collection, with M.T. assisting. Resources: G.S., K.S., and M.S. provided essential study materials. Data curation: S.C., M.A., and M.T. managed data annotation, cleaning, and maintenance. Writing—original draft: M.A., S.C., and M.T. prepared the initial draft. Writing—review and editing: S.C., K.S., M.S., and G.S. reviewed and revised the article. Visualization: S.C., M.A., and M.T. created data visualizations supporting study findings.
Author Disclosure Statement
M.S., G.S., and K.S. are shareholders and employees of Aptos Medical, Tbilisi, Georgia. M.S. is a consultant of Aptos Medical, Tbilisi, Georgia. S.C. is the CEO of Cotofana Anatomy Corp, a company invested in anatomy education.
Funding Information
Data analysis and medical writing of the article received financial support from Aptos Medical, Tbilisi, Georgia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.