
Abstract
Background:
At present, there is no gender-affirming facial surgery that offers feminization of the lateral neck.
Objective:
To demonstrate reliable relationship between the great auricular nerve point (GAP) and spinal accessory nerve along the sternocleidomastoid muscle (SCM) in human anatomical specimens and demonstrate feasibility of muscle transection in one transgender female patient.
Methods:
A total of 14 human anatomical specimen dissections were performed to determine if a transection of the SCM perpendicular to the GAP could be performed without potential compromise of the spinal accessory nerve. The surgical course of a patient who underwent transection is discussed.
Results:
Mean distance from the GAP to the accessory nerve at the posterior border of the sternocleidomastoid was 1.01 ± 0.54 cm, consistent with results from prior studies. In both the human anatomical specimens and the patient, sternocleidomastoid muscles were divided without injury to accessory nerve. The patient’s neck girth was reduced by an average of 7 cm at 2 years post-operatively.
Conclusion:
Transection with distal denervation of the SCM by identifying the relationship between the GAP and accessory nerve is a feasible method of feminizing the lateral neck to improve cosmetic satisfaction while minimizing the risks of cervical neurovascular injury.
Key Points
Introduction
Facial feminization surgery (FFS) refers to a set of procedures that modify characteristically male features to provide a more feminine facial appearance. 1 Using craniofacial and aesthetic surgical approaches, surgeons mitigate gender dysphoria by bridging the gap between accepted gender norms of facial morphometrics and a patient’s inward identification and unique interpretation of their gender.2–5 A wealth of research underscores the positive effects of gender affirmation surgery on mental health-related quality of life, self-perception of beauty, and patient satisfaction scores.3,5
FFS procedures are often grouped into stages. A first-stage FFS might involve modifications to craniomaxillofacial structures, such as hairline advancement, feminizing frontal cranioplasty, chondrolaryngoplasty, or reduction mandibuloplasty. 6 A second-stage FFS might involve soft-tissue procedures such as cheek fat grafting, blepharoplasty, face/neck lifting, and lip augmentation. A patient may opt to pursue all, just a few, or extensions of these procedures depending on the degree and location of dysphoria they experience related to their facial physiognomy.
While many procedures modify features of the face, there are fewer options to feminize the neck. Soft tissue procedures for neck modification such as rhytidectomy are routinely performed but are rarely covered by insurance. 7 Non-surgical procedures, such as platysma neurotoxin injections, only address the rejuvenation of the neck and inadequately address the underlying muscle bulk that contributes to the appearance of masculinity. 8 Neck characteristics most significantly associated with perception of female gender include reduced neck girth, skin smoothness, and reduced thyroid protrusion. 9 On average, males have 7% greater muscle volume compared to females and differences in percentage of muscle mass are shared between cervical muscles such as the longus capitis muscle, obliquus capitis inferior muscle, and sternocleidomastoid muscle (SCM).10,11 Given this sex-specific variability of neck volume and patient requests for neck feminization, we sought to develop a safe, minimally invasive, aesthetically appealing approach to achieve a reduction in neck girth while preserving critical muscle function and preventing iatrogenic nerve injury. In this study, the objective was to measure the distance and demonstrate reliability of the anatomical relationship between the great auricular nerve point (GAP) and spinal accessory nerve along the SCM. This will serve to assure that among patients seeking SCM thinning for cervical feminization that muscle contouring is feasible while protecting against cervical neurovascular injury.
Methods
Institutional review board approval from the University of California, San Francisco was obtained prior to investigation.
The necks of seven freshly frozen human anatomical specimen heads were dissected bilaterally on surgical tables in a training facility at our institution to demonstrate proof-of-concept and safety of the proposed technique. Subjects with congenital neck deformities or a history of neck dissection or surgery were excluded. All subjects were measured using a ruler, with the neck in a straight position with the head perpendicular to the neck. Measures of central tendency and variability were used for statistical analysis.
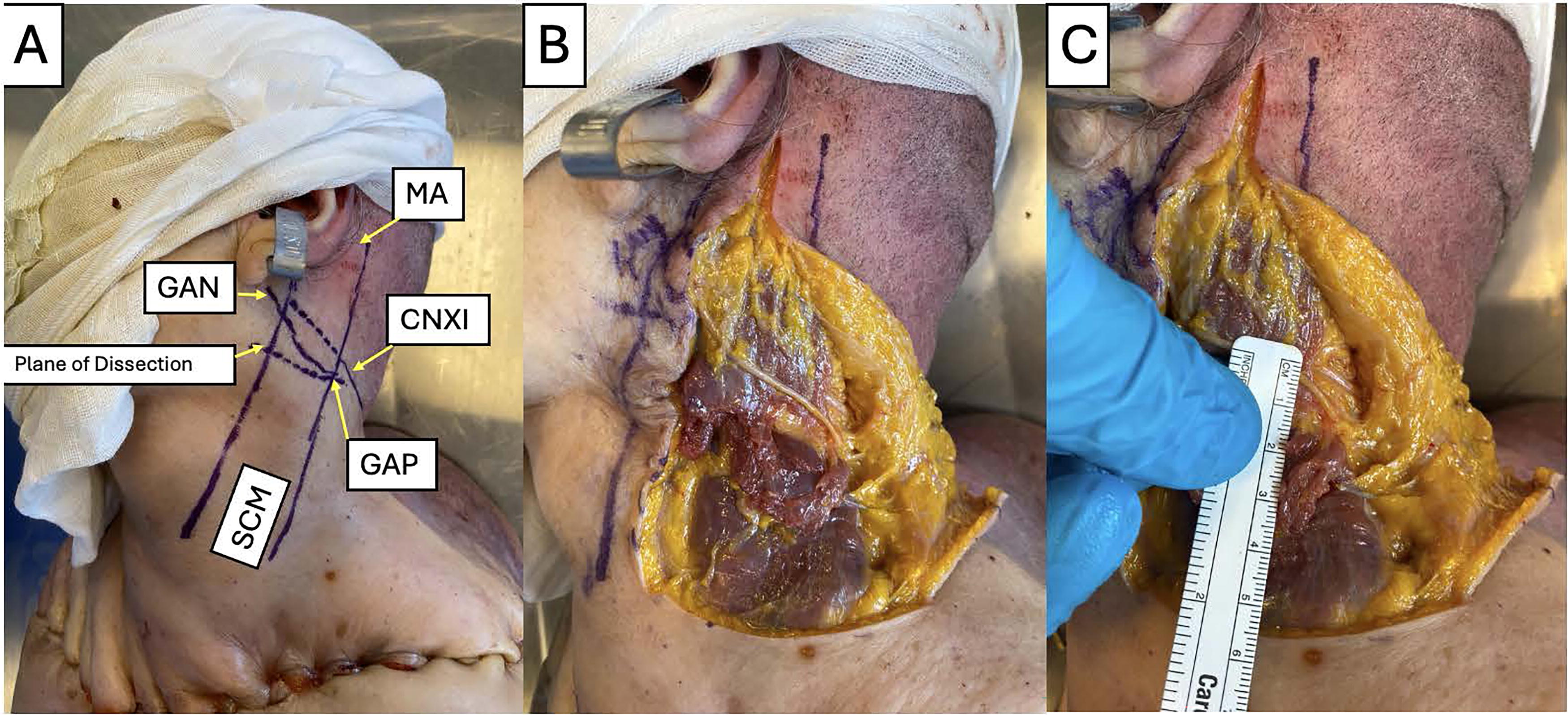
First, a midline neck incision was made and subplatysmal flaps were elevated to identify the great auricular nerve (GAN). Then, the GAP was identified at the emergence of the GAN over the posterior border of the SCM. The SCM muscle was then completely transected at a plane from the GAP to the anterior border of the SCM perpendicular to the direction of the muscle fibers (Fig. 1). The distance from the GAP to accessory nerve (CNXI)—where the CNXI crossed the posterior border of the SCM into level 5—was measured (Fig. 2). Distance from the mastoid apex (MA) to CNXI was also measured. Any injury to CNXI was recorded.
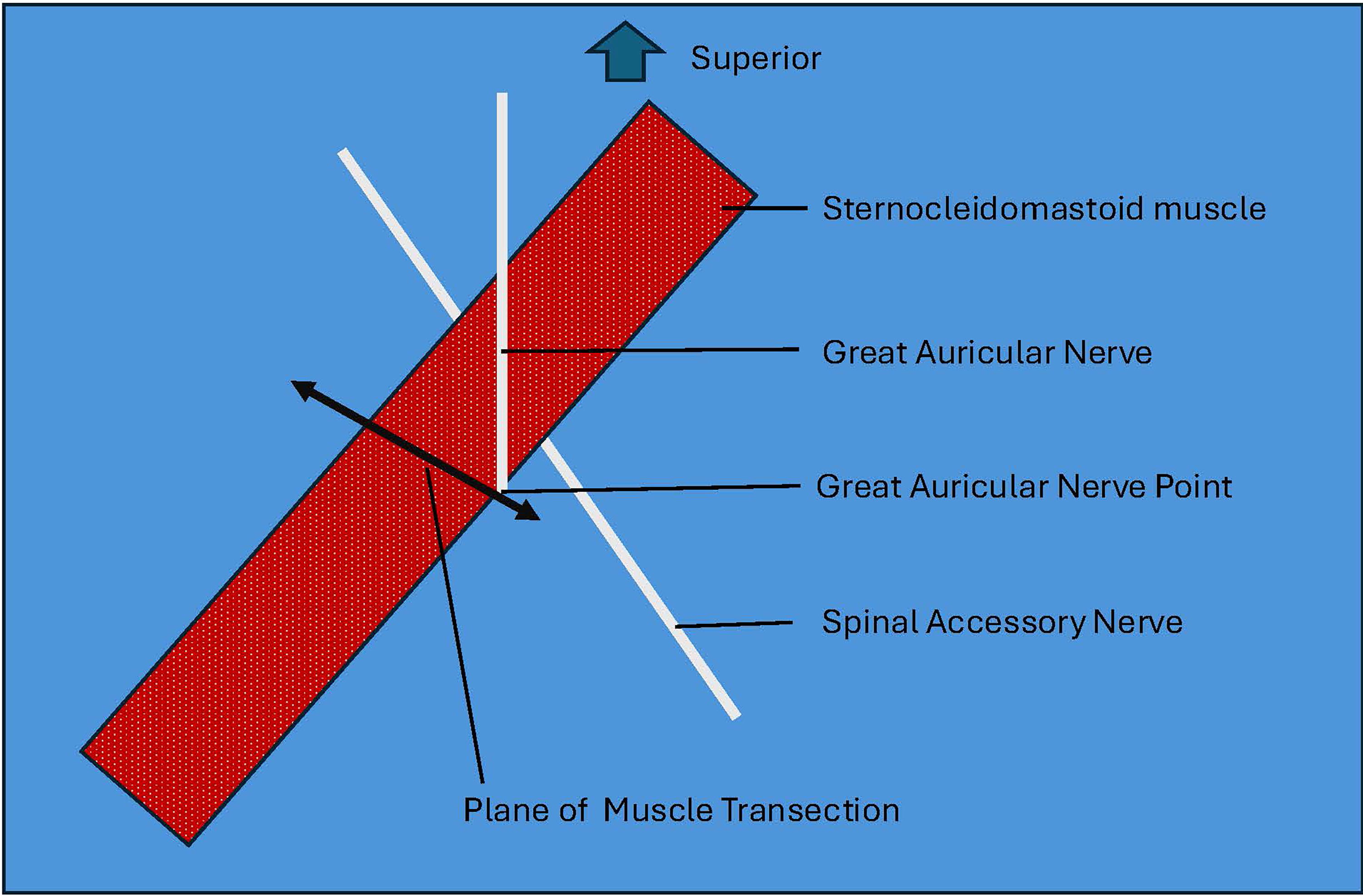
Diagram illustrating anatomical landmarks of the neck showing the sternocleidomastoid muscle, great auricular nerve, great auricular nerve point, spinal accessory nerve, and the plane of muscle transection.
Results
Table 1 provides the CNXI measurements. Mean GAP-CNXI distance was 1.01 ± 0.54 cm (range: 0.2–1.6) with a variance of 0.27 and mean CNXI-MA distance was 6.36 ± 0.79 cm (range: 5.1–7.8) with a variance of 0.58. In all 14 necks, the GAP was inferior to the level of CNXI. No CNXI injury was observed.
Distances from GAP to CNXI and distances from CNXI at the posterior border of the sternocleidomastoid muscle to MA measured in seven cadavers dissected bilaterally
CNXI, accessory nerve; GAN, the great auricular nerve; GAP, great auricular point; MA, mastoid apex; PBSCM, the posterior border of the sternocleidomastoid muscle.
Case Study
Surgical protocol
A 51-year-old transgender woman with a medical history of gender dysphoria on estradiol, finasteride, and spironolactone, presented with a desire for further workup of her brows, cheeks, and neck to look more “feminine.” Neck girth was measured pre-operatively in the superior and inferior neck. Written consent was obtained after an extensive discussion of potential risks, benefits, and alternatives. A bilateral upper lid blepharoplasty, bilateral face/neck lift with platysmaplasty, cheek fat graft augmentation, and a bilateral SCM division was performed by the authors J.A.W and P.D.K.
A post-tragal preauricular incision was made extending behind the ear and into the hairline at the helical touch point. Then, a flap was raised in a sub-superficial musculoaponeurotic system plane in a standard deep plane facelift manner. The GAN and external jugular vein were identified. At the level of the GAP, a right-angle clamp was used to dissect through the sternocleidomastoid muscle, which was then transected sequentially with monopolar cautery. This division stopped once the internal jugular vein was encountered. Once transected, the inferior 2/3rds of the SCM retracted down into the sternoclavicular region. The deep plane face/neck lift was then performed in a standard fashion and neck drains were placed. The girth of the superior and inferior neck was measured pre-operatively and at 2 years post-operatively. No post-operative physical therapy or neck exercises were recommended or undertaken.
Surgical outcomes
The 51-year-old transgender female presented with dysphoria related to the girth of her neck, among other features. She consented to FFS with the novel SCM reduction procedure, which was fully explained to her on multiple occasions and well in advance of the surgical procedure. Preoperative neck girth was measured at 44 cm superiorly and 45 cm inferiorly. Her body mass index (BMI) on the day of surgery was 30 kg/m2. The procedure was uncomplicated, and the patient was discharged home on the second day following surgery. Her post-operative course was unremarkable, and she had full cervical neck flexion, extension, and rotation on physical exam. After a year, she continued to have full range of motion in her neck but noted mild bilateral neck fullness at the parotid tail region for which she was aesthetically unsatisfied. To address this concern in addition to the desire for additional procedures, she underwent revision surgery including fat grafts to her nasolabial folds, revision rhinoplasty, and revision facelift with further thinning of the cephalic portion of the SCM. BMI at the time of second surgery was 28 kg/m2. Preoperative and postoperative images are shown in Figure 3. At two years post-operatively, neck girth was measured to be 38 cm superiorly and 37 cm inferiorly, a reduction of 6 cm and 8 cm centimeters, respectively. Post-operative computed tomography demonstrates the relative low volume appearance of the SCMs (Fig. 4).

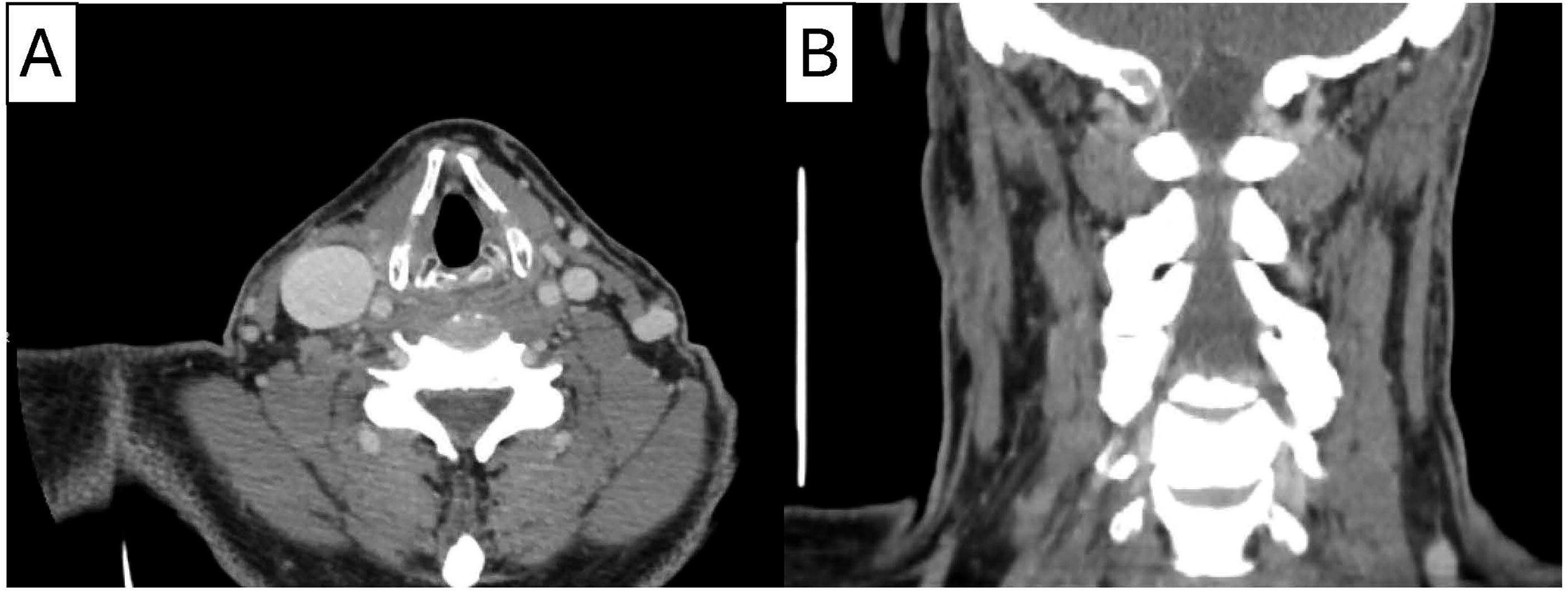
Computed tomography neck
Discussion
FFS of the neck to reduce girth has heretofore only included reductive chondrolaryngoplasty with little regard for lateral neck appearance.8,12 While submental fat excision, liposuction, and platysma tightening can also be performed to enhance the desired neck contour, these procedures may fail to alleviate gender dysphoria caused by extensive neck muscle girth, as they primarily focus on selective recontouring and vertico-lateral suspension. Therefore, we developed a technique to reduce the neck circumference that emphasizes both postoperative cosmesis and maintenance of complete cervical neurovascular function.
Prior to enrolling the patient, a human anatomical specimen study was performed to examine potential variation in CNXI location relative to the GAP. CNXI is an important structure for surgeons in head and neck surgery and preservation of its integrity down to the trapezius muscle is key to allow for full elevation, retraction, and rotation of the scapula as well as maintenance of shoulder function and complete arm elevation.13–15 Occasionally, iatrogenic injuries can occur during lymph cervical node excision, necessitating careful planning and dissection of the region. Preserved neck range of motion has long been established following SCM resection during head and neck cancer surgery. 16
Identifying the course of the GAN and the position of the GAP is essential to the minimal access and aesthetic component of this surgery. As identification of CNXI is challenging through the access afforded by a face/neck lift incision, the GAP serves as a surrogate for the most inferior location of the exit point of CNXI from the posterior border of the SCM. The GAP therefore marks the plane where the SCM can be safely divided with minimal risk of inadvertent injury to the accessory nerve. After transection, it is assumed that the distal 2/3rds of the SCM will retract into the lower neck, where it will undergo progressive denervation atrophy. Denervated muscle typically undergoes atrophy of greater than 50% of the innervated resting volume. 17 The proximal 1/3rd of the SCM is expected to retract into the upper neck, where its bulk will be maintained, as it is still innervated by CNXI. Our patient did experience some contour irregularities of the proximal SCM after the initial transection and consequently underwent revision surgery. Given the known innervation of the proximal SCM, further studies evaluating this technique should assess the possible benefit of simultaneous debulking of the proximal SCM at the time of initial division, which may prevent contour irregularities prompting the need for a second procedure.
Previous investigators have studied the relationship of the GAP and CNXI. Mirjalili et al. showed that distance as measured by ultrasound between GAP and CNXI at the PBSCM was 1.1 cm superiorly to GAN with a range of 0.1–2.1 cm. 18 Another study by Raikos et al. gave the mean value of 0.92 ± 0.55 cm for the GAP-CNXI distance. 19 In agreement with these studies, we found that the GAP was consistently located below the point at which CNXI exited the posterior border of the SCM.
Given that this surgery was only performed in one individual, we are unable to comment on general aesthetic and functional outcomes besides the anecdotal reporting of our patient. After two procedures, our patient demonstrated an excellent final aesthetic and functional outcome of a 6 cm-reduced superior and 8 cm-reduced inferior neck circumference (Fig. 2). Her postoperative neck circumference falls closer to averages of female neck girth of individuals of her age and BMI reported in the literature of 34–36 cm.20,21 Nevertheless, given the novelty of this procedure, a variety of complications may be encountered. Patients should be fully informed about all potential sequelae, most notably risk of temporary or permanent injury to CNXI, need for additional procedures, and potential change in neck strength or range of motion.
Limitations include the paucity of literature attempting to identify if a link exists between increased neck circumference and gender dysphoria. Further research should therefore go into understanding regions of the lower face and neck as it pertains to dysphoria for patients seeking feminization procedures that can corroborate a potential role for this musculoskeletal modification. Among whom conservative measures have disappointed, this minimally invasive SCM transection procedure should only be considered for patients with severe gender-associated neck dysphoria. Like any novel surgical procedure, it should be regarded as experimental and applied following a prolonged informed consent process. As surgeons, we must carefully guard against over-aggressive approaches that may cause inadvertent injury to our patients. In addition, the issues experienced by the patient with some contour irregularity and fullness of parotid region necessitating revision surgery should be investigated further in a larger cohort of patients to ascertain trends and assess if modifications to the technique must be considered. Finally, the patient did lose weight between the first and second surgeries as well as at the time of postoperative follow-up and may have also contributed to the decrease in neck circumference. Limitations of the human anatomical specimen study include the lack of documentation regarding patient sex, height, and neck diameter which may confound the distances measured between neck landmarks and therefore the reliability of the technique. This is especially important given that patient height was shown to be a factor in determining the location of CNXI relative to the PBSCM in a study by Abakay et al. 22
Conclusion
Despite research indicating sex-specific anatomical differences in neck volume and reduced neck girth being associated with perceptions of femininity, techniques for feminizing the lateral neck have not yet been reported. We developed a technique to reduce SCM bulk, performed a proof-of-concept human anatomical specimens study to assess the procedure’s safety in preserving the CNXI, and then performed the technique in a patient who identifies as transgender, with excellent functional and aesthetic outcomes after revision surgery. Further research is necessary to identify if this procedure is associated with improvements in psychosocial outcomes, aesthetic outcomes, and minimal functional deficits in larger sample size cohorts.
Footnotes
Authors’ Contributions
R.M.B.: Conceptualization, data curation, formal analysis, investigation, project administration, visualization, writing—original draft, writing—review and editing. J.K.C.: Data curation, methodology, investigation, supervision, writing—review and editing. J.A.W.: Investigation, supervision, writing—review and editing. P.D.K.: Conceptualization, investigation, methodology, supervision, writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.