
Abstract
Numerous techniques achieve maxillomandibular fixation (MMF), each with benefits and risks. While using Erich arch bars to achieve MMF has remained the gold standard through the last century, the technique has multiple limitations, which have spurred innovative approaches, such as intermaxillary fixation (IMF) screws, hybrid arch bars, embrasure wires, and dental occlusion ties. The surge in new MMF technologies over the past decade prompted this analysis to compare these techniques. A PubMed search was conducted to identify all current FDA-approved modern MMF technologies from 2005 through 2023, evaluating their advantages and limitations. Studies with controlled scientific comparisons of techniques were limited, precluding a systematic review. Analysis showed no definitive data exist to endorse one technique as a universal option. As multiple MMF options offer appropriate stability, a surgeon may choose an approach based upon numerous factors: comminution/instability; need for physiotherapy, including guiding elastics; safety; time of application/removal; and patient comfort. This article guides the selection between techniques based on these factors and presents a decision algorithm to assist surgeons in selecting the ideal MMF technique for each patient.
Introduction
Maxillomandibular fixation (MMF) is the establishment of a rigid construct to immobilize the mandibular and maxillary dentition into occlusion. There are many indications for placing a patient in MMF, including facial fractures, orthognathic surgery, and temporomandibular joint surgery. Arch bar application as a means of MMF first emerged in the 1940s and has remained a standard. The technology, commonly referenced as “Erich arch bars,” was popularized by John B. Erich and described in his 1944 publication: “Traumatic Injuries of Facial Bones (An Atlas of Treatment).” 1 Over the last few decades, multiple alternative FDA-cleared MMF techniques have emerged, each with its benefits and risks over traditional arch bars. These newer techniques have aimed to reduce operating room time, improve comfort and ease of hygiene for the patient, and decrease the risk of wire stick injuries to the operative team without compromising stable occlusive results. These techniques include hybrid arch bars, 2 intermaxillary fixation (IMF) screws, 3 embrasure wires, 4 and dental occlusion ties. 5 The addition of many different techniques and inconsistency with nomenclature has made objective comparisons challenging, such that most of these approaches have little randomized trial data. Without an adequate data repository, we performed an analysis of available evidence on contemporary techniques, which is intended to (1) identify modern MMF options, (2) provide surgeons with a thorough understanding of the strengths and weaknesses of these technologies, and (3) create a decision algorithm to aid in technique selection.
Methods
A PubMed search was conducted to identify assessments of contemporary maxillomandibular fixation techniques from 2005 through 2023, initially using the search terms (1) “maxillomandibular fixation,” (2) “maxillary–mandibular fixation,” and (3) “intermaxillary fixation.” Search results were refined using filters for study type (randomized controlled trial, review, systematic review), English language, and human subjects. The resulting 152 studies were reviewed for relevance, leaving 27 articles. Most of these articles were comparisons between Erich arch bars and IMF screws, with very few articles, including hybrid arch bars, embrasure wires, and dental occlusion ties (likely secondary to their relatively recent FDA approval). Only three articles6–8 included randomized trials of hybrid arch bar systems, another three evaluated IMF screws,6,9,10 one included embrasure wires, 11 and none included dental occlusion ties. This precluded a systematic review. As the purpose of this review was to include all current FDA-cleared techniques, the search terms were expanded to include “hybrid arch bars,” “embrasure wires,” “interdental wires,” and “dental occlusion ties” for the same timeframe. This produced an additional 20 articles. Thus, the final inclusion criteria comprised studies referencing current FDA-cleared technologies for establishing MMF. Articles focused on pediatric mandible fractures were excluded. Morisada et al. provide a 2022 review of the unique aspects of pediatric mandible fracture management. 12 Additionally, those referencing older techniques or older techniques (eyelet wires or “Rapid IMF” circumdental plastic lugs), not studied in the 2005–2023 timeframe, were also excluded. All remaining studies were compiled for this analysis.
Advancement of Maxillomandibular Fixation Techniques
For decades, Erich Arch bars remained the gold standard for establishing MMF despite limitations of prolonged operative time and risk of wire stick injuries. Newer techniques were developed to address these and have gained increasing adoption as they not only reduce operating room time and wire-related injuries but also improve comfort and ease of hygiene for the patient. IMF screws were introduced first in 1989. 3 This technique employs screw fixation to the mandible and maxilla, thereby eliminating the arch bars and circumdental wires. However, it limits the sites of vertical fixation across the maxillary and mandibular arches and places tooth roots at risk of injury.10,13–15 Embrasure wires (sometimes described as “interdental fixation”) were first described in 1999. 4 These eliminate the circumdental wires of arch bars as well as the bone (and potential tooth root) trauma of IMF screws. Their use has been limited to intraoperative application to stabilize occlusion during placement of internal fixation hardware. Hybrid systems first appeared in 2012. 2 Multiple manufacturers have proprietary designs (Stryker’s SMARTLock, Johnson & Johnson’s Matrix Wave, Zimmer Biomet’s OmniMax, and KLS Martin’s L1 MMF). They combine the bone fixation capabilities of IMF screws with increased lateral stability and additional sites of vertical fixation offered by arch bars. However, they retained the risk of bone and tooth root trauma like IMF screws. 16 Most recently in 2017, 5 dental occlusion ties (Invisian’s Minne Ties) were released combining the application efficiency of embrasure wires with the potential for nonoperative applications and postoperative MMF, which embrasure wires lacked due to their difficulty removing in emergency circumstances. Pictures of these techniques are shown in Figure 1. Less commonly used techniques, such as Ernst ligatures, Ivy loops/eyelet wires, Gilmer wiring, Stout wiring, etc., are not discussed in this study but have been compared in prior reviews (McGinn and Fedok in 2008 17 and Akadira and Omitiola in 2012). 18 Although manual stabilization during surgery is not unreasonable in selected fractures (as demonstrated by data published by Bell and Wilson for noncomminuted mandibular angle fractures undergoing Champy plate fixation 19 ), it does not create a durable or rigid MMF construct and was therefore excluded from this review.
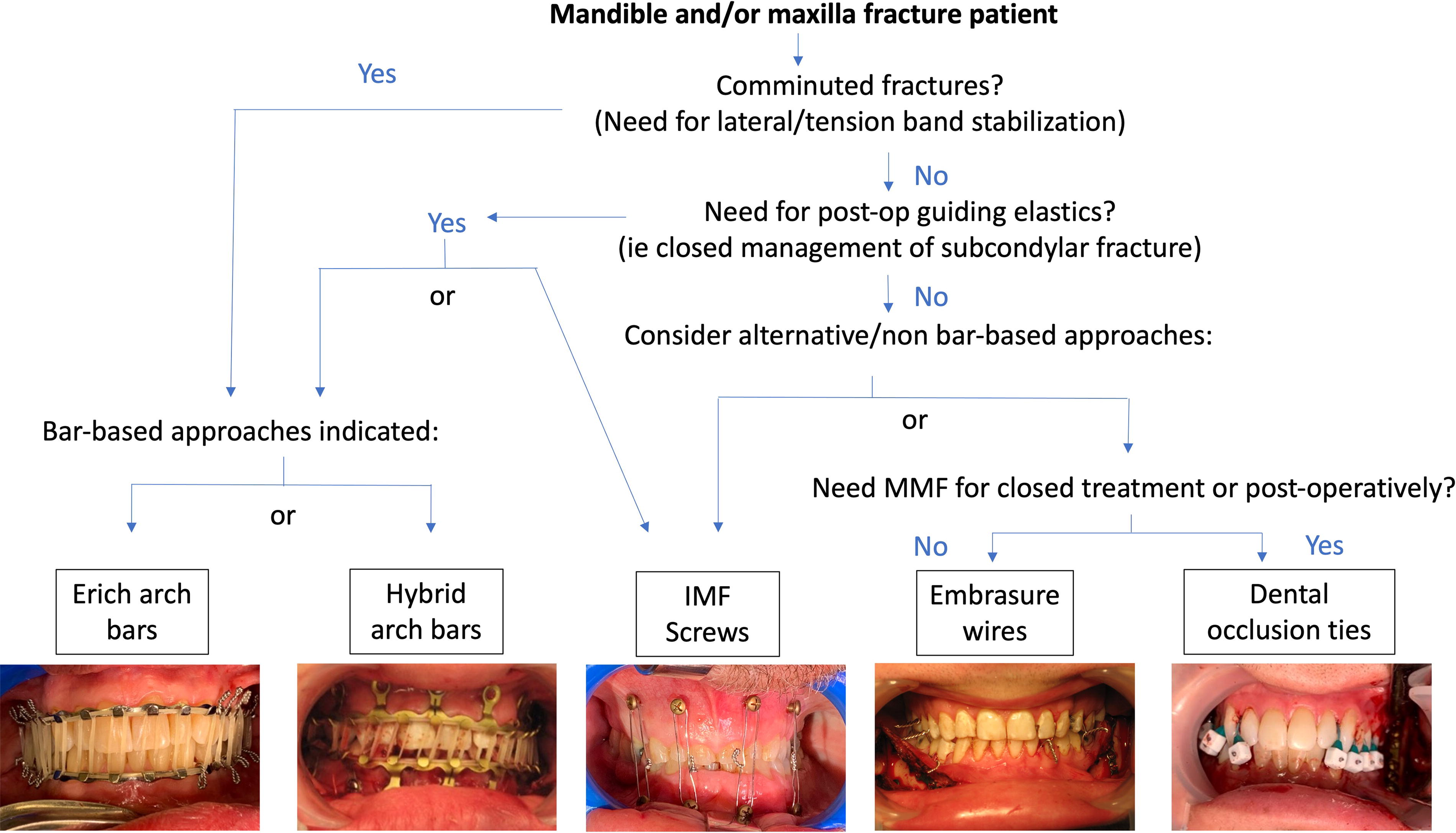
Maxillomandibular fixation selection decision algorithm. Erich arch bars and hybrid arch bars provide the best stability for comminuted fractures and versatility for applying guiding elastics. These techniques are preferred if dealing with unstable fractures or if expecting to need ongoing physiotherapy to restore normal occlusion. If, however, fractures are noncomminuted and postoperative care will not require extended physiotherapy, a surgeon can consider less-invasive techniques (IMF screws, embrasure wires, and dental occlusion ties) for patient comfort, decreased tooth roots/gingiva/nerve injury risk, and reduced surgical team sharps injury risk.IMF, intermaxillary fixation.
The Evidence Basis for Comparing MMF Techniques
In contrast to the relatively large number of methods surgeons can use to establish MMF, there are a limited number of robust clinical studies to determine which method may be most advantageous. Evidence-based guidelines in mandible fracture care are limited. 20 In 2013, a Cochrane review titled “Interventions for the management of mandibular fractures,” 21 assessed available literature and concluded there was inadequate evidence to demonstrate the superiority of any single technique over others. The review attributed the lack of high-quality evidence to “clinical diversity, variability in assessment tools used, and difficulty in grading outcomes.” Two years later, Falci et al. published a noninferiority evaluation of screw-based hybrid systems and stated: “There is not enough evidence to conclude that the Erich arch bar is the best intermaxillary fixation method in cases of oral and maxillofacial fractures.” 22
Even with the growing body of literature emphasizing the advantages of newer techniques mitigating some of the challenges associated with Erich arch bars, they have remained the “gold standard” and surgeons must retain a working knowledge of how to use them.
Suitability of an MMF Technique
The two paramount concepts in MMF are: (1) providing adequate stabilization (both vertical stability of the rigid MMF construct, and lateral stability of the mobile dentate segments), and (2) planning for physiotherapy with guiding elastics. The indication for MMF (facial fracture management vs orthognathic or temporomandibular joint surgery) and severity or location of dental arch disruption will often dictate the degree to which both are needed. These tenets are essential because inadequate stability can result in persistent malocclusion or nonunion, and the inability to provide bite retraining may compromise occlusive outcome or lead to trismus (if prolonged rigid fixation is required). Table 1 summarizes indications and contraindications for various MMF techniques, offering a surgeon a simplified summary of whether a technique is suitable for the given indication. (The authors also recommend using the online AO Surgery Reference for detailed explanations, videos, and instructions dedicated to MMF applications and CMF facial trauma care). 23 When considering stability and versatility for postoperative physiotherapy (guiding elastics), Erich arch bars can generally be utilized for all cases. All other techniques provide at least a slightly lower grade of inherent stability, which may preclude their use. Conversely, if the patient’s fracture pattern or indication for MMF offers some inherent stability, multiple techniques are viable and may be selected based on other strengths and weaknesses.
MMF techniques indications/contraindications comparison
MMF, maxillomandibular fixation; EAB, Erich arch bars; IMF, intermaxillary fixation; HAB, hybrid arch bars; EW, embrasure wires; DOT, dental occlusion ties.
+, indicated; -, contraindicated.
Relative Strengths and Limitations of Individual Techniques
Many factors have been compared between MMF techniques, including cost, time of application and removal, required anesthetic, and duration of MMF. Quantitative comparisons of these details are summarized in Table 2. Risks also vary by technique, including the risk of damage to surrounding structures, including bone, teeth (periodontal disease), tooth roots, nerve, and soft tissue. Finally, the risk of sharps injuries to the surgical team varies.4,7 Each of these is evaluated below.
MMF techniques, application, and removal comparison
Embrasure wires are only employed for intraoperative MMF.
MMF, maxillomandibular fixation; EAB, Erich arch bars; IMF, intermaxillary fixation; HAB, hybrid arch bars; EW, embrasure wires; DOT, dental occlusion ties.
Erich arch bars
While arch bars provide the most stable construct of all the options, they cause considerable soft tissue trauma to the gingiva and adjacent mucosa. Postoperative complications related to extragingival trauma, limited dental hygiene increasing risk of caries, and constrained nutrition are notably higher with Erich arch bars in comparison to other techniques.17,31 Operative time required for the application of Erich arch bars is much longer when compared with newer screw-based or embrasure wire techniques.26,37–39 Finally, the risk of wire stick injuries during application is highest with this technique with a 50% glove puncture rate in some studies.40,41
Screw-based techniques
IMF screws
IMF screws may be used for rigid fixation or guiding elastics. They provide rapid placement (10–27 min), and low risk of wire stick injury to the surgical team.6,9,10,42 Postoperatively, they may be removed in the clinic using local anesthesia. 10 When compared with traditional Erich arch bar systems, oral hygiene (based on plaque deposition) is much better in patients with IMF screws. 10 However, all screw-based techniques carry the risk of tooth root injury. Studies quantifying this risk have measured it between 4–12.5%.10,13–15 Additional studies demonstrate that this risk is dramatically decreased by avoiding predrilling, postulating that if no predrilling is employed, the screws can “glance off” the tooth roots. 15 Additionally, gingival overgrowth can occur, 31 particularly when placed in the loose (unattached) gingiva. This can cause patient discomfort and difficulty with removal. The placement of screws in the gingiva can also interfere with access to the gingivobuccal sulcus for exposure incisions. The necessary placement of IMF screws further from the occlusal line can induce a lingual cant to the loose alveolar segments when tightening rigid fixation wires. In contrast to Erich arch bars, IMF screws provide no lateral stabilization of tooth segments and rely on interdigitating dentition (or dentures), and noncomminuted fractures to create a rigid MMF construct through dental splinting. In patients who require prolonged MMF or guiding elastics, IMF screws may not be appropriate as they have a 5–25% chance of loosening to the point of failure or avulsion.10,43
Hybrid arch bars
As with IMF screws, the risk of sharps injury with hybrid arch bars is dramatically decreased relative to Erich arch bars, placement can be rapid (7–42 min), and removal can be performed in the clinic.7,16,24,44,45 Hybrid systems provide points of anchoring rigid fixation closer to the occlusal line, decreasing potential lingual cant seen with IMF screws. Compared with arch bars, hybrid systems carry a lower risk of gingival injury/recession. As a screw-based system, they carry a similar risk of tooth root injury as IMF screws. 16 The screws are shorter, but (for most manufacturers) the same diameter. While this provides multiple points of fixating the arch bar to the alveolus and greater stability for prolonged guiding elastics, it also creates more potential sites for gingival overgrowth. Like IMF screws, hybrid systems may obstruct access to the gingivobuccal sulcus, interfering with incision closure. In comparison to IMF screws, good dentition is helpful (but not as critical) for establishing solid MMF with this technique. With multiple sites of fixation and a rigid bar, some lateral stability is afforded by the use of hybrid systems.
Intradental techniques
Embrasure wires
Embrasure wires originally utilized a pair of 24-gauge stainless steel wires “placed through the contact point of the lower premolars from the buccal aspect” and passed through the “upper premolars from the palatal aspect” to form a loop. 4 Wires are applied bilaterally and then twisted to pull the patient’s dentition into rigid occlusion. Using larger diameter wires (20 or 22 gauge) applied through the interdental spaces between the premolars or molars relies less on narrow dental spaces. 26 Studies have emphasized the value of using embrasure wires instead of arch bars in appropriate patients showing no significant difference in postoperative complications and statistically significant time savings, measuring embrasure wire application and removal in two minutes for each.4,26,27,38,46 Rapid application and low-profile construct make embrasure wires ideal when stabilizing good native occlusion for subsequent open reduction and internal fixation. Embrasure wires pose no risk to tooth roots. Importantly, this approach is inappropriate for patients with poor (or wide) interproximal contacts, edentulous patients, gross dental mobility, or severe periodontal disease, in addition to patients with comminuted fractures. Like IMF screws, embrasure wires alone provide only a vertical force supporting occlusion with no lateral stability, although they can be used with bridle wires or ivy loops. There is also no option to apply postoperative MMF stabilization or elastics.
Dental occlusion ties
Dental occlusion ties have seen increasing use in mandible fractures 34 and temporomandibular joint replacement since FDA clearance in 2017. 35 The technology offers similar application efficiency to embrasure wires. In contrast to other MMF technologies, dental occlusion ties are blunt-tipped, polymer-based, “zip tie” style devices that largely eliminate sharps injury risk and wire-associated patient discomfort. Similar to embrasure wires, the devices are threaded through the apical embrasures between teeth and around their contact points. 5 They come in 1.0 and 0.7 diameters, comparable to 18- and 21-gauge wires. A balance of these devices is applied bilaterally to the dentition. In contrast to embrasure wires, these devices can remain for postoperative MMF as they are relatively easy for patients to cut and remove in emergent situations. Like IMF screws and embrasure wires, these devices are intended to apply a vertical force to reinforce occlusion and establish MMF. They do not provide a lateral force vector, although they can be used as a bridal wire around adjacent teeth. As such, they are contraindicated in patients with comminuted fractures, poor or limited dentition, and patients needing guiding elastics.
Choosing an Optimized MMF Technique Using Case-Based Examples
To illustrate using the above factors in determining the optimal technique for MMF, a decision algorithm is illustrated in Figure 1. This algorithm is applied in the following clinical scenarios, and key clinical indications considerations are summarized in Table 3.
The bold text indicates the criteria that are used in figure 1 to navigate the decision algorithm.
MMF, maxillomandibular fixation; IMF, intermaxillary fixation.
Case 1: A 32-year-old man fell off his bike sustaining a comminuted right mandibular body and left displaced condyle fractures. On exam, two right molars are loose adjacent to the body fracture. Treatment included open reduction with internal fixation of the fractures, including intraoperative and postoperative MMF. Erich arch bars were chosen for extra MMF stability and the ability to stabilize loose teeth with the circumdental wires. Postoperative progressive physiotherapy was achieved with guiding elastics applied to the arch bars to manage the displaced left condyle fracture that was not amenable to open reduction/fixation.
Case 2: A 26-year-old woman was assaulted, sustaining a unilateral left condylar fracture with joint involvement and loss of height. Examination reveals a right anterior open bite. Treatment goals include providing stable MMF to allow healing, yet options for early mobilization to prevent ankylosis of the involved joint. Hybrid arch bars were selected to provide stable MMF with versatility in applying guiding elastics for physiotherapy while avoiding the sharps risk and prolonged operative time required for Erich arch bar application.
Case 3: An 18-year-old is struck in the left jaw by a baseball resulting in noncomminuted, nondisplaced fractures to the left mandibular angle and right condyle. Without comminution or displacement of fractures, rapid healing is anticipated. MMF will likely be for short-duration support and/or comfort without a need for prolonged postoperative guiding elastic physiotherapy. Early mobilization is generally advocated to prevent ankylosis of the right condyle. IMF screws are chosen for speed of application, minimal gingival and bony trauma from screws, decreased patient discomfort compared with arch bars and hybrid arch bars, avoidance of sharps risk, unobstructed access to the angle fracture, and easier in-clinic removal.
Case 4: A 28-year-old male falls during a seizure striking his face on a curb resulting in a noncomminuted but markedly displaced right-angle fracture. Good dentition and a noncomminuted fracture enable stable reduction. The ORIF hardware is “load-sharing” with the stable reduction, increasing the likelihood that he will heal without additional postoperative MMF support. Postoperative rigid MMF is necessarily avoided given his seizure history. Embrasure wires are chosen for intraoperative MMF as they minimize gingival tissue trauma compared with other techniques, minimize sharps risk, avoid obstruction to the angle fracture, and provide a time-efficient method of achieving MMF.
Case 5: A 52-year-old woman strikes her jaw on the dash in a car accident, resulting in noncomminuted, moderately displaced right body and left angle fractures. Intraoperative and postoperative MMF is desired for stability while healing, but guiding elastics are not anticipated to be needed as her occlusion is favorable. Dental occlusion ties are selected to minimize gingival trauma and sharps risk while providing a fast application in the OR and stable MMF until they are removed in the clinic. Like IMF screws and embrasure wires, dental occlusion ties also avoid obstructing access to the mandibular angle fracture.
Conclusion
Establishing proper (and stable) occlusion is paramount for the treatment of fractures and orthognathic and temporomandibular joint surgeries. As a result, MMF remains a critical step in the surgical management of pathologies involving the mandibular and maxillary dentition. While many techniques may be available, the two critical suitability considerations are: 1) the ability of the technique to provide adequate stabilization based on fracture pattern, location, and baseline occlusion, and 2) the need for postoperative physiotherapy. The decision algorithm in Figure 1 provides a framework for considering these criteria and other inherent strengths and weaknesses of each technique to optimize patient outcomes while minimizing costs, time, and risks to both the patient and the surgical team.
Footnotes
Authors’ Contributions
A.W.J.: Conceptualization, methodology, and writing—original draft and review & editing. S.A.: Conceptualization, methodology, and writing—original draft and review & editing. S.B.: Conceptualization, methodology, and writing—original draft and review & editing.
Author Disclosure Statement
Dr. Alan Johnson receives royalties from the University of Minnesota for inventing dental occlusion ties. Dr. Scott E Bevans, MD is AO Faculty. He does not receive honoraria or any direct payments for participation in AO courses. Dr. Scott Bevans is in the United States Army. Reference herein to any specific commercial products, process, or service by trade name, trademark, manufacturer, or otherwise, does not necessarily constitute or imply its endorsement, recommendation, or favoring by the United States Government. Sarah Akkina: No conflicts of interest.
Disclaimers
The views expressed in this study are those of the authors and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the U.S. Government.
Funding Information
No funding was received for this article.