
Abstract
Reconstructing the nose is one of facial plastic surgery’s most common reconstructive challenges. While the forehead flap is widely utilized in nasal reconstruction, the effectiveness of a single forehead flap for subtotal/total nasal reconstruction is limited. Building on previously described fold-over flap techniques, we introduce a unique trifold forehead flap method for total nasal reconstruction utilizing a single forehead flap. The described technique holds promise for simplifying the surgical process while achieving desirable functional and cosmetic outcomes in total/subtotal nasal reconstruction.
Introduction
Nasal reconstruction poses a common reconstructive challenge with distinct functional and cosmetic considerations. Reconstruction of the nose requires attention to three critical anatomical components: (1) nasal lining, (2) structure, and (3) covering. 1 The forehead flap has been established as a workhorse in nasal reconstruction for larger defects owing to its robust tissue stock, reliable vascular supply, limited donor site morbidity, and excellent cosmetic results.1–3 Various modern techniques have been introduced to expand the use of the forehead flap for nasal reconstruction and improve cosmetic results.2,4 Despite these contemporary methods, subtotal and total nasal reconstruction remains challenging for surgeons.
Millard, Menick, and Burget introduced a three-stage turn-in technique combining nasal lining and coverage, simplifying donor requirements, and refining modern nasal reconstruction.3–5 Menick’s fold-over forehead flap with delayed primary cartilage graft would become one of the most widely used single-modality methods for full-thickness nasal defects. For total nasal reconstruction, surgeons have often used multiple local flaps or free tissue transfer to meet the added tissue requirements of bilateral nasal subunit reconstruction.3,6,7 Integrating multiple flaps to reproduce delicate nasal anatomy aesthetically is exceptionally challenging. To our knowledge, total nasal reconstruction using a single local flap has not been described in modern nasal reconstruction literature. Expanding on fold-over flap techniques described by Menick and Burget, we describe a novel trifold flap method that allows for total nasal reconstruction with a single forehead flap (Fig. 1).

Pre and 2-months post trifold flap patient photos.
Surgical Technique
Stage I
Preliminary operation
The nasal platform is first re-established using other reconstructive methods to restore the lip and cheek subunits before nasal reconstruction (Fig. 2a–c).
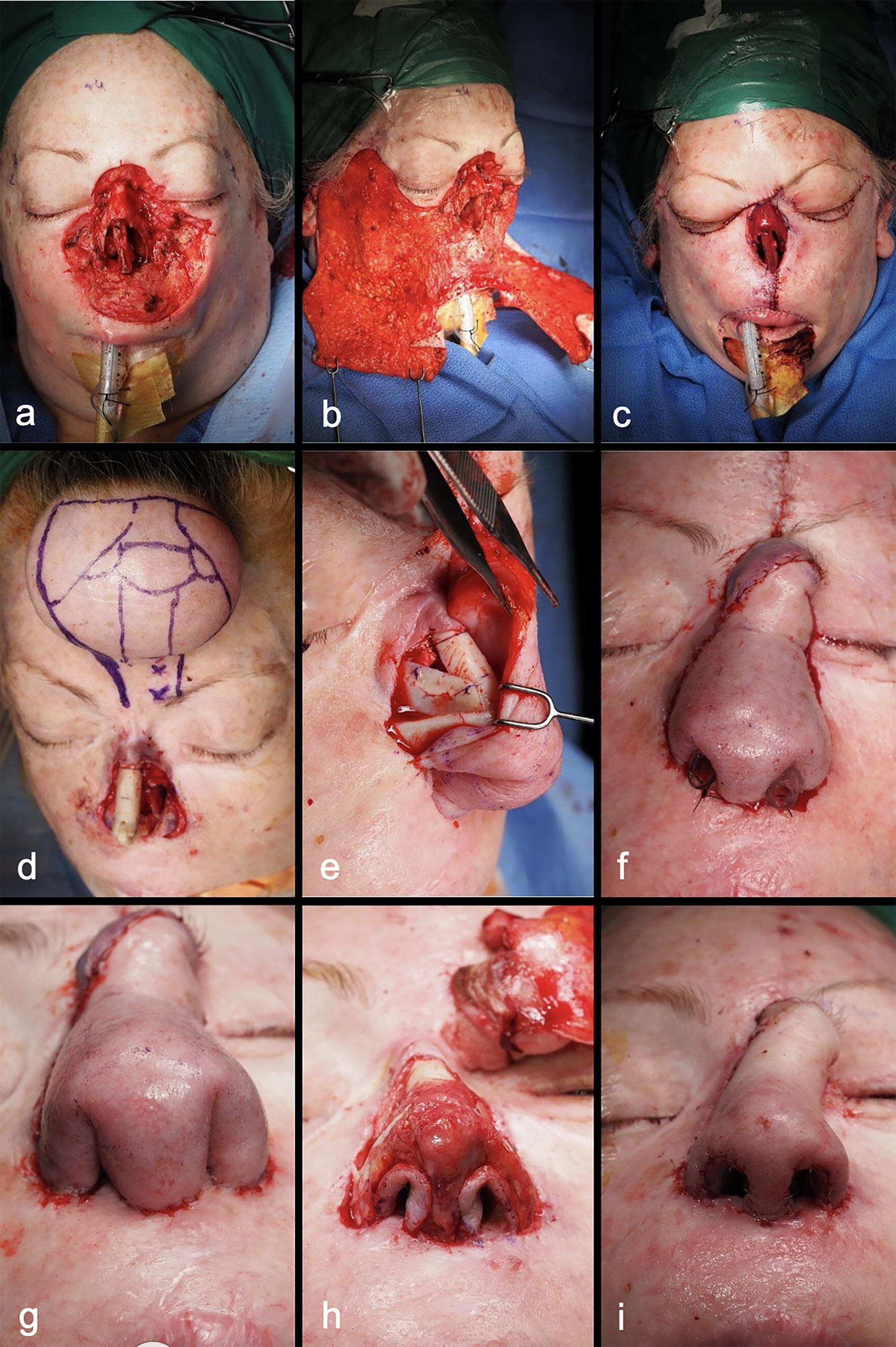
Intraoperative patient photos at various trifold flap stages.
Tissue expansion (optional)
Tissue expansion can help improve perfusion of a larger forehead flap 8 and may be completed if indicated. Indications for tissue expansion include short forehead length, insufficient hairless flap length, and thicker skin types less conducive to folding without compromising blood supply. Tissue expansion was completed using a 7.5 × 6.0 × 1.5 cm subgaleal expander filled to a volume of 85 cc over 6 weeks. The first-stage forehead flap surgery was completed 6 weeks after achieving the desired volume.
Stage II
First-stage trifold forehead flap
To begin the first stage trifold forehead flap, the skin and support structures are prepped for acceptance of the paramedian forehead flap. The nasal framework is created using cadaveric or costal cartilage via L-strut creation secured to the facial skeleton (Fig. 2d). Additional grafting is performed as indicated.
The template for the paramedian forehead flap is designed to integrate both lining and external coverage using foil suture packaging. The template is then used to mark the donor forehead tissue centered on the corresponding supratrochlear artery (Fig. 2d). A full-thickness paramedian flap is then raised. The flap is then rotated in the usual fashion over the defect. The distal corners of the flap are then in-folded bilaterally to reconstruct nasal vestibular and septal lining defects. The in-folded edges of the flap are sewn to previously elevated mucoperichondrial flaps at the intranasal recipient site. In-folding the distal corners creates a central third corner that is then positioned over the septal construct to generate a columella and caudal septal lining. The lateral alar component is then curled medially toward the neo-columella, recreating the gentle alar curve in the base view of the nose (Fig. 2e, g). A split-thickness skin graft (optional) is harvested for the posterior pedicle surface. Nasal stents are placed to restore airway patency as needed until the intermediate operation (Fig. 2f).
Stage III
Intermediate operation
Incisions of the flap’s distal borders and bilateral alar rim incisions are made to lift the proximal resurfacing portion flap off the lower nasal third (Fig. 2h). The soft tissues on the surface of the lower nasal cartilage constructs are thinned, and the cartilage is sculpted. The nasal lining is then thinned to widen the nasal vestibules. The reflected soft tissues overlying the lower lateral cartilages are then thinned before the closure of the flap back over the lower nasal construct (Fig. 2i).
Stage IV
Pedicle division
The pedicle is divided and inset per surgeon preference. Thinning of the proximal lining flap is done during pedicle division to reconstruct the superior third of the nose.
Postoperative course
The presented patient has been followed for over 18 months since the final surgery for pedicle division. Nasal cones were used to improve the patency of the nasal airway in the first 6 months after surgery and were not needed thereafter. Kenalog was injected once 6 months post-pedicle division to diminish edema and scarring at the alar rim. Distal flap edges healed well to mucosal flaps with no dehiscence or perforation.
Conclusion
The paramedian forehead flap is the leading method for nasal reconstruction with excellent functional and cosmetic results. Previously, total nasal reconstruction using multiple local flaps or free flaps has been described. We introduce a novel approach to total nasal reconstruction using a single forehead flap. By expanding upon established techniques using a tri-fold flap method, we present an alternative approach to total nasal reconstruction that leverages structural tissue properties to better recreate the aesthetic and functional features of the nose in a simplified, adaptable, and reproducible procedure.
Footnotes
Acknowledgments
The authors thank the patient for allowing us to share the details presented in this case. This article was published with the patient’s written consent.
Authors’ Contributions
T.C. wrote the article and conducted a literature review. S.R.O. contributed the presented case, article design, and article revision. S.R.O. and Z.A.K. co-developed the described surgical technique. Z.A.K. critically revised the article. All authors reviewed and approved the final version of the article.
Author Disclosure Statement
T.C., S.R.O., and Z.A.K. have no disclosures. An AI-generated voice was used to narrate the accompanying video.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.