
Abstract
Background:
Port-wine stain (PWS) is a congenital capillary malformation occurring commonly in the head and neck. Left untreated, affected areas may darken and hypertrophy over time, resulting in pronounced disfigurement, risk of spontaneous hemorrhage, and functional impairment. The burden of hypertrophic facial PWS and the benefit of laser therapy have not heretofore been well characterized. Herein, the health utility of these two states is assessed among naïve observers.
Methods:
Naïve observers (n = 262) ranked the utility of four randomized health states (monocular blindness, binocular blindness, hypertrophic facial PWS, and laser-treated facial PWS) by means of visual analogue scale (VAS), standard gamble (SG), and time trade-off (TTO) techniques. Health states are presented using standardized facial photographs.
Results:
Health utilities (VAS, SG, and TTO) were reported as follows (mean ± standard deviation): monocular blindness (0.73 ± 0.21, 0.86 ± 0.21, 0.87 ± 0.18), binocular blindness (0.51 ± 0.26, 0.72 ± 0.27, 0.69 ± 0.27), hypertrophic facial PWS (0.71 ± 0.24, 0.83 ± 0.23, 0.83 ± 0.21), and laser-treated facial PWS (0.87 ± 0.16, 0.91 ± 0.18, 0.92 ± 0.16). Laser-treated facial PWS showed significantly higher utility measures than the untreated hypertrophic state (p < 0.001, all measures), with a difference of 3.24 quality-adjusted life years. Linear regression analysis revealed that non-Caucasian race and higher level of education were associated with lower SG and TTO utility scores for the hypertrophic facial PWS state among naïve observers.
Conclusions:
Societal-perceived utility of hypertrophic facial PWS is similar to that of monocular blindness. Laser-treated facial PWS is perceived significantly more favorably than the untreated hypertrophic state. These findings provide insight into the societal burden of facial PWS and impact of laser treatment, facilitating objective comparisons with other disparate disease states.
Key Points
Introduction
Port-wine stains (PWSs) are congenital capillary malformations characterized by pink cutaneous macular patches at an incidence of 3 per 1000 live births with no gender predilection.1–3 Two-thirds of these malformations present in the cervicofacial region, predominantly distributed along the trigeminal nerve dermatomes.4,5 Although initially pale, pink, and flat, PWSs left untreated grow in size and depth over time. This progressive growth leads to darkening and thickening of the lesion, resulting in nodule formation with risk of spontaneous hemorrhage, inflammation, and chronic infection,6–8 often profoundly impacting the individuals' psychosocial life.9–12 Besides cosmetic disfigurement, PWS hypertrophy may functionally impair sight, speech, nasal breathing, or hearing. 13 Camouflage of lesions in the head and neck is challenging, compelling many patients to seek treatment.
Pulsed dye laser (PDL) irradiation is the current standard-of-care therapy for PWS. 14 Using PDL, light energy is selectively absorbed by hemoglobin in a single-photon wavelength-dependent process known as selective photothermolysis. The targeted hemoglobin coagulates within the ectatic PWS blood vessels sparing injury to adjacent healthy tissues and preserving normal tissue architecture. 15 Such specificity has enabled PDL therapy in infancy,16–18 where the response to PDL therapy is more favorable than later in life. 19 Mature PWSs often require combination PDL therapy with alexandrite laser (755 nm), a near-infrared laser that penetrates 50–75% deeper into tissue than PDL, 20 to selectively destroy deeper PWS blood vessels while minimizing scarring. Although concurrent PDL and alexandrite treatments may achieve significant lightening and arrest of hypertrophic PWS maturation, 21 the economic impact and perceived burden of pre- and post-treatment health states have not been investigated.
Health utility assessment allows for quantifying disease severity and preferences for a given health state. The “utility” of a given health state is presented as a normalized value between 0 (representing death) and 1 (perfect health), assessed using visual analogue scales (VASs), standard gamble (SG), and/or time trade-off (TTO) techniques.22–24 Utilities are attractive tools in health economic decision analysis, as they permit direct comparison of disparate disease states. Furthermore, utilities can be transformed into quality-adjusted life years (QALYs), 25 a common measure used to inform health care resource allocation decisions. Although utilities can be elicited from a number of populations, values used in economic evaluations are typically elicited from members of the general population on the premise that allocation of public funds is best guided by societal preference. 26
In this study, the utilities of hypertrophic facial PWS and laser-treated facial PWS states are assessed among naïve observers using standardized facial photographs.
Methods
This study was approved by the Massachusetts Eye and Ear Institutional Review Board.
Research facility and survey tool
A computer-based health utility questionnaire was developed in REDCap 27 and administered at the Harvard Decision Science Laboratory (HDSL; Harvard University, Cambridge, MA). A group of trained research assistants was available on site to provide experimental assistance to participants during survey sessions.
Study participants
Over a 5-month enrollment period, adult volunteers in the HDSL-managed participant pool were invited to enroll in this study through an online advertisement. All volunteers signed an electronic informed consent form before study commencement. Participants completed a questionnaire that involved rating the utility of four health states: monocular blindness, binocular blindness, hypertrophic facial PWS, and laser-treated facial PWS followed by an anonymous demographic survey. The order of health state descriptions was randomized to limit response-shift bias. Participant responses were captured and recorded in the REDCap database hosted behind a secure firewall.
Health state narratives
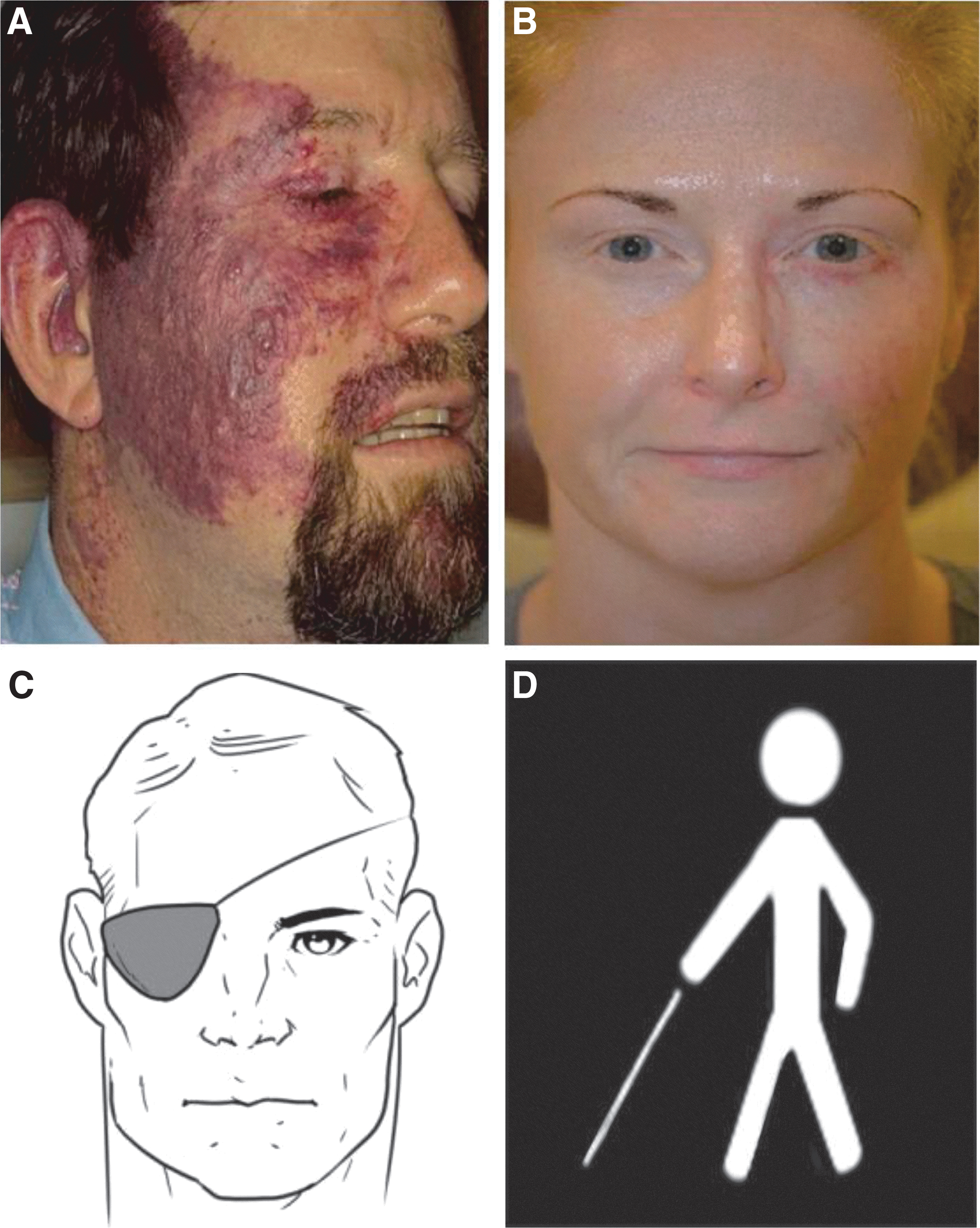
Health state descriptions of hypertrophic facial PWS and laser-treated facial PWS were constructed based on clinical experiences of patients treated at Massachusetts Eye and Ear and expert opinion (O.T.T.). Monocular and binocular blindness health states were included as internal controls to assess individual comprehension and risk tolerance. Clinical narratives were limited to 60 words or fewer to limit respondent fatigue. Each narrative was accompanied by a single image of either a blindness or PWS health state (Fig. 1) to limit repeated measures effect.
(
The hypertrophic facial PWS narrative depicted a 46-year-old man with an untreated nodular PWS distributed in the right maxillary nerve dermatome. The lesion involved the right cheek, temple, eyelids, upper lip, nose, and pinna. The patient reported several prior episodes of spontaneous ulceration and hemorrhage. His case was chosen to illustrate the natural evolution of a facial PWS left untreated by the fifth decade of life (Fig. 1A).
The laser-treated facial PWS narrative depicted a 36-year-old woman with a lightened PWS on the left side of her face, distributed in the left maxillary dermatome involving the temple, eyelids, upper lip, and nose. This patient received 90 dual-laser treatments averaging one treatment every 2 months between the ages of 15 and 36 years. Her case was chosen to illustrate the typical ability of a combination of PDL (595 nm) and alexandrite (755 nm) laser treatments to reduce the PWS lesion severity over time (Fig. 1B).
The pictorial supplements for monocular blindness and binocular blindness are shown in Figure 1C and D. These supplements have become standard visual aids to depict monocular and binocular blindness in health utility studies.28,29
Health state utility assessment
Health utilities were measured using standard and widely employed VAS, SG, and TTO measures. 30 Participants were asked to imagine themselves as the described patients in each health state, as has been done for numerous published health utility studies.28,29,31,32
The VAS component was administered according to previously published practices,28,29,31,32 consisting of a continuous sliding scale with death and perfect health anchored at opposite ends (see Supplementary Data—Top Frame Figure, which illustrates the VAS). In this method, participants were asked to rate their perceived health in the given state using a sliding bar scale, consisting of 1-point increments between 0 (death) and 100 (perfect health). The following formula was used to calculate the VAS score: VAS/100.
The SG component was assessed by asking participants to imagine themselves in the given health state and choose either to remain in that health state or take a chance in choosing treatment that held some probability of failure (death) and some probability of success (perfect health) (see Supplementary Data—Middle Frame Figure, which illustrates the SG technique). A six-level iterative ping-pong method was employed in which the risk of taking treatment varied from 1% to 97.81%, whereas the corresponding chance of survival varied from 99% to 2.19%, respectively. An asymmetric titration search routine generated up to six different iterations of risk-taking scenarios until a final inflection point of accepted risk was found. The following formula was used to calculate the SG score: (100 – percent risk of death at the point of indifference)/100.
In the TTO component, participants were asked to choose between “trading off” a certain number of years of life to live in perfect health or to live a specific number of years in the described health state (see Supplementary Data—Bottom Frame Figure, which illustrates the TTO technique). In each health state scenario, 36 years of life was designated as the fixed time horizon, which correlated with average life expectancy (∼80 years) and the development of localized hypertrophy and nodularity in facial PWS patients by the fifth decade of life. 33 In a manner similar to the SG method, a six-level iterative ping-pong method was employed in which years traded-off varied from 1 to 35.81, whereas corresponding years kept in a state of perfect health varied from 35 to 0.19 until an indifference point was found. The following formula was used to calculate the TTO score: (36 years – number of years traded off at the point of indifference)/36 years.
Statistical analysis
Utility scores were normalized to a standardized utility scale ranging from 0 (death) to 1 (perfect health) and assessed for normality and homogeneity using the Shapiro–Wilk test and Levene statistic, respectively. Responses in which a participant rated monocular blindness as having a higher utility than binocular blindness across one or more of VAS, SG, or TTO measures, or provided identical utility ratings across all health state scenarios, were excluded from analysis. Means and standard deviations (SDs) of VAS, SG, and TTO scores were calculated and one-way analysis of variance (ANOVA) with post hoc pairwise comparison using Scheffe's method was used for intergroup comparisons.
Simple linear regression and ANOVA models were employed to assess univariate associations between observer demographic variables (e.g., age, gender, race/ethnicity, income, education, and marital status) and each of the utility scores (VAS, SG, and TTO) for the different health states. Multivariable linear regression models were then used to determine which demographic variables remained significant predictors of utility scores while adjusting for other variables. To adequately control for the balance of variables and avoid significant multicollinearity issues, a stepwise regression approach was used to optimally add or remove variables (p < 0.05 for addition, p > 0.10 for removal) from the models. Regression models were checked for multicollinearity and violations of model assumptions by examining variance inflation factors and residual plots, respectively. All tests were performed using IBM SPSS Statistics commercial software (v25; IBM Corp., Armonk, NY), with significance level (α) set at 0.05 (two-tailed) with Bonferroni correction.
Results
Demographics
During a 5-month enrollment period, 327 volunteers were recruited and completed the survey at the HDSL. Of the 327 sets of individual responses, surveys from 262 participants (mean [SD] age, 31.6 [13.5] years; 126 women [48.1%]; 131 men [50.0%]; 5 unknown [1.9%]) met a priori inclusion criteria and were included in the final analysis. Sixty-five surveys were excluded given that individual participants—in ranking binocular blindness as higher than, or equal to, monocular blindness (on any one or more of VAS, SG, or TTO measures)—exhibited failure to comprehend the survey tools. The median household income distribution of included participants ($50,001–$75,000) was representative of the U.S. population, 34 while demographics skewed toward younger individuals with a higher level of education. Demographic characteristics of study participants are summarized in Table 1.
GED, general education development; SD, standard deviation.
Health utility outcomes
Health utility values ranged from 0 (death) to 1 (perfect health with no facial PWS) and are reported in Table 2. Mean ± SD utility scores (VAS, SG, and TTO) for hypertrophic facial PWS (0.71 ± 0.24, 0.83 ± 0.23, 0.83 ± 0.21) ranked significantly higher (were more favorable) than scores for binocular blindness (0.51 ± 0.26, 0.72 ± 0.27, 0.69 ± 0.27; p < 0.001, all measures), while approaching scores for monocular blindness (0.73 ± 0.21, 0.86 ± 0.21, 0.87 ± 0.18). Post hoc comparisons demonstrated that laser-treated facial PWS (0.87 ± 0.16, 0.91 ± 0.18, 0.92 ± 0.16) significantly improved health utility across VAS, SG, and TTO measures (p < 0.001, all measures) when compared with the hypertrophic facial PWS health state (Table 3).
Values are reported as mean ± SD.
One-way ANOVA (bold indicates significant at α = 0.05).
ANOVA, analysis of variance; PWS, port-wine stain; SG, standard gamble; TTO, time trade-off; VAS, visual analogue scale.
Post hoc Scheffe test for pairwise comparisons (bold indicates significant at α = 0.05).
Linear regression
Simple linear regression showed no univariate associations between observer income or marital status and utility scores (VAS, SG, and TTO) for the hypertrophic facial PWS health state (Table 4). Thus, observer age, gender, race/ethnicity (dichotomized into Caucasian and non-Caucasian cohorts), and education level, all variables significant in simple linear regression analysis, were entered as predictor variables in a stepwise manner in the multivariable regression models for VAS, SG, and TTO scores (Table 5). Observer gender was the only significant predictor of the VAS score, with males reporting lower scores on this measure (β = −0.060, 95% CI: −0.118 to −0.002, p = 0.041) than their female counterparts. Observer race/ethnicity was a significant predictor of SG and TTO scores for hypertrophic facial PWS, with Caucasians reporting higher scores for SG (β = 0.075, 95% CI: 0.019–0.130, p = 0.009) and TTO (β = 0.057, 95% CI: 0.007–0.106, p = 0.025) than their non-Caucasian counterparts. Finally, level of education showed a negative correlation with scores for SG (β = −0.221, 95% CI: −0.373 to −0.068, p = 0.005) and TTO (β = −0.180, 95% CI: −0.316 to −0.045, p = 0.009) for the hypertrophic facial PWS state. The models fit the assumptions of linear regression and variance inflation factors were low, indicating multicollinearity was insignificant.
Simple linear regression/ANOVA models (bold indicates significant at α = 0.05).
B, unstandardized regression coefficient; CI, confidence interval; REF, reference variable; SE, standard error.
Multivariable linear regression (bold indicates significant at α = 0.05).
R 2 , coefficient for multiple determination.
Discussion
Facial PWS is a debilitating condition that has significant functional and psychosocial impact on affected individuals. Although prior studies have demonstrated quality-of-life impairment secondary to facial PWS,35–37 this is the first study to objectively quantify the utility of hypertrophic and laser-treated facial PWS health states among a convenience sample of community volunteers. One previous study investigated TTO and willingness to pay for laser therapy among patients who had already undergone treatment for facial PWS, but was limited by a small sample size and preclusion of VAS and SG methods. 38 Thus, the health state burden of hypertrophic facial PWS and the benefit of laser treatment as assessed from the public's perspective remain uninvestigated and highly relevant. Herein, societal-derived utility of these health states was measured objectively using standardized and well-established methods (VAS, SG, and TTO)39,40 among naïve observers.
Several studies have shown that patients' quality of life, psychosocial adjustment, and self-esteem are negatively impacted by a facial PWS,35–37,41 with emotional distress correlating with size and darkness of the PWS, resulting from progressive dilation of the ectatic vasculature. Our study has demonstrated that a sample of naïve observers equates the burden of living with hypertrophic facial PWS (0.71 ± 0.24, 0.83 ± 0.23, 0.83 ± 0.21) to that of monocular blindness (0.73 ± 0.21, 0.86 ± 0.21, 0.87 ± 0.18), a recognized functional impairment associated with known utility decrements. Participants were willing to theoretically undergo treatment that carried a 17% chance of death and sacrifice 17%, or 6.12 years, of their remaining 36 years of life to attain perfect health (e.g., normal facial appearance with no PWS). Based on these reported health utility scores, hypertrophic facial PWS is perceived to be comparable with other aesthetically and functionally compromised conditions such as cleft lip and palate (SG: 0.84; TTO: 0.85) 42 and unilateral microtia with deafness (SG: 0.86; TTO: 0.83), 43 but less burdensome than unilateral flaccid facial palsy (SG: 0.79; TTO: 0.78), 31 including flaccid facial palsy (SG: 0.71; TTO: 0.72) and postparalytic facial synkinesis (SG: 0.75; TTO: 0.74). 28
The significantly higher utility scores reported for the laser-treated facial PWS state than those reported for the hypertrophic facial PWS state (VAS: +0.16; SG: +0.09; TTO: +0.09; p < 0.001 all measures) lend support to the societal benefit of laser treatment over observation in this disease. Assuming laser treatment increases the utility state of hypertrophic facial PWS by 0.09 over a remaining average life expectancy of 36 years, it would comprise a gain of 3.24 QALYs. Using a cost-effectiveness threshold of $100,000 per QALY, 44 laser treatment of hypertrophic facial PWS would be cost-effective at $324,000, assuming treatment achieved 100% blanching results without adverse complications. Although not a formal cost-effectiveness study, there is value in applying these findings toward understanding how the general U.S. population perceives and valuates the effectiveness of laser treatment in lessening the burden of facial PWSs.
This study possesses significant limitations. Most importantly, clinical vignettes comprised different adult patient examples for each health state, which may limit the generalizability of our results to a wide spectrum of facial PWS patients. Although effort was made to minimize potential confounders through selection of a common race, defect size, and location, the latter of which are known to naturally influence observer perceptions and ratings of facial stimuli, 45 factors such as age, race, gender, and perceived attractiveness were not accounted for. Patient positioning, expression, lighting, and inclusion of both sides of the face were not standardized, nor were a series of demographically balanced photograph pairs employed, which would have yielded better representation of the treated and untreated health states. The fact that the two PWS viewpoints demonstrate pathology on opposite sides of the face, and that only the right face is shown in the untreated scenario, introduced another important confounder since research supports that the left and right facial hemispheres may be perceived differently.
Other weaknesses include the fact that, although study participants represent a socioeconomically diverse sampling of the U.S. population, our sample was largely comprised of younger, highly educated individuals recruited in a single city, which is not representative of the whole of society. Herein, only societal preferences were assessed, which may differ from patient-assessed utilities of various PWS disease states. Prospective studies are currently underway to gain deeper insight into how facial PWS patients valuate the impact of their disease.
Furthermore, the “ideal” study design would be to include the same patient—before and after laser treatments—to eliminate all of the aforementioned variables. However, most patients with access to laser therapy begin treatments in infancy, and the only mature nodular birthmarks are those wherein patients have not had access to laser and surgical therapies. Laser treatments are also delivered over decades, and not all PWSs develop morphologically at the same rate, nor do all develop mature nodular lesions.
The final VAS, SG, and TTO multivariable models explained only 3.6%, 6.1%, and 4.8% of the observed variance between demographic factors, respectively, suggesting that disfigurement of hypertrophic facial PWS was universally perceived as similar across disparate demographic groups in this study. In future research, random selection of multiple patients with varying degrees of facial PWS could be employed to control for inherent sources of variance within this dermatological condition. Furthermore, although this study's findings provide insight into the societal-perceived burden of untreated and laser-treated hypertrophic facial PWS states and have a high potential for use in health economic evaluations, readers should assess the suitability of applying our findings to their own population.
Conclusions
Societal health utility evaluation of hypertrophic facial PWS appears similar to that of monocular blindness, with observers willing to sacrifice 6.12 years of remaining life, or undergo treatment carrying a 17% chance of death, to reverse the condition. Laser-treated facial PWS demonstrates significantly higher naïve-observer assessed utility in comparison with a hypertrophic facial PWS state. Future studies are required to verify this preliminary finding in a larger sample of treated and untreated states, using standardized views, photographic lighting conditions, and same sidedness. It will also be important to further clarify the burden of varying manifestations of facial PWSs and cost-effectiveness of available therapies.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.