
Abstract
Importance:
Although conventional hump resections are a hallmark of rhinoplasty, there has been a rekindled interest in dorsal preservation (DP) techniques as a means for addressing the dorsal hump, with claims of superior functional and aesthetic results. As such, an understanding of DP, including technical considerations and outcomes, is imperative.
Observations:
DP allows for mobilization of the osseocartilaginous nasal vault as a single unit and thereby prevents disruption of the natural keystone area. The osseous nasal vault is managed with a transverse osteotomy and either a bilateral single lateral osteotomy (pushdown procedure) or bilateral bony wedge resections (letdown procedure) to allow for descent of the nasal dorsum. A variety of approaches to the septum exist, each differentiated by the location of cartilage resection: subdorsal, high-septal, midseptal, or inferior septum. These techniques result in pleasing dorsal aesthetic lines but may be limited by a higher rate of dorsal hump recurrence. Patency of the internal nasal valve (INV) is theoretically improved with DP. Robust series with patient-reported outcomes are lacking, although several reports and early experience at our center with a newly described high-septal resection technique do suggest positive functional and cosmetic outcomes with DP.
Conclusions and Relevance:
With the recent revitalized interest in DP, an understanding of the potential benefits, techniques, and challenges associated with this surgery is helpful. Maintenance of the dorsum as a single unit has implications for maintaining structural integrity at the nasal keystone, pleasing dorsal aesthetic lines, and the patency of the INV. As surgeons continue to develop and employ these techniques, critical assessment of patient-reported outcomes and objective nasal measurements, with an emphasis on comparison with standard hump takedown techniques, will be valuable.
Introduction
Rhinoplasty is one of the most challenging yet rewarding surgical procedures performed by facial plastic surgeons. Studies on social perception point to the primacy of an ideal nasal profile as a main outcome for patients, with the tip being secondary. 1 Despite this, one method, with relatively minor variation, has dominated in practice and teaching.
The classic technique of removing dorsal nasal bone and cartilage as championed by Joseph has become a hallmark of rhinoplasty. 2 Variations in the method center primarily on technique of osteotomy and method of midvault reconstruction. 3 Despite the success of this technique in reduction of a dorsal hump and improving the profile view, the disruption of the natural keystone has long-term implications for maintaining (1) structural integrity of the nasal keystone, (2) pleasing dorsal aesthetic lines, and (3) patency of the internal nasal valve (INV).4,5 Recently, some have suggested that dorsal resection should be replaced by preservation. 6 Although this may seem revolutionary, dorsal preservation (DP) and its evolution are not new. This article provides a review of DP, with an emphasis on indications, technical considerations (including discussion of a modified technique), challenges, and outcomes that may be helpful for the novice DP surgeon.
Historical Context
The idea of preserving the dorsal nasal architecture was introduced in 1899 by the otolaryngologist Goodale.7,8 In an original description of a patient with a dorsal hump, he described removal of subdorsal cartilage and lateral osteotomies to allow for mobilization of the nasal vault. Upon disarticulation of the nasal–frontal junction, the nasal dorsum was lowered to rest on a lowered septum, thereby eliminating the dorsal hump. In 1914, Lothrop described using subdorsal cartilage resection, resection of a wedge of ethmoid bone, bilateral bony wedge resections at the nasomaxillary suture, and a transverse osteotomy at the radix to allow for descent of the dorsum. 9 Subsequently, several authors in France reported success with similar techniques.10,11
In 1946, Cottle, in the setting of nasal fractures, found that while attempting to down-fracture the nasal bones, the cartilaginous septum resisted their movement, and that excision of cartilage at the premaxilla allowed for adequate mobilization. 12 These findings were applied to rhinoplasty, in which the cartilaginous septum was separated from the ethmoid plate and resection of a strip of cartilage at the maxillary spine allowed for descent of the dorsum. Initially, a single lateral osteotomy was performed to allow for down-fracture of the nasal bones—a technique that was termed the “pushdown” (PD) procedure (similar to Goodale's technique). Cottle found that the amount of descent of the nasal bones was limited by the bony attachment of the inferior turbinate to the lateral wall of the nose. Double lateral osteotomies with removal of bone was suggested as a means for overcoming this problem by several surgeons (similar to Lothrop's technique).13,14 This technique would eventually become known as the “letdown” (LD) procedure.
In 1989, Gola described a closed roof rhinoplasty in which septal cartilage was resected in the subdorsal region (similar to Goodale and distinct from Cottle's description of a lower septal resection).15,16 In the 2000s, Saban championed this high-subdorsal technique, describing a superior cut to correspond to the configuration of the preoperative dorsum and the inferior cut to correspond to the shape of the desired dorsum.17,18 He also proposed reasons for why, despite the successes of DP, the techniques were gradually abandoned. 18 First, the septal cartilage cuts as performed by Cottle were deemed to be challenging. Second, the techniques were not thought to be versatile enough for the significantly distorted dorsum. Finally, although DP techniques were commonly performed using closed approaches, greater visibility, control of structures, and improved teaching with the open approach introduced alternative strategies for managing the dorsum. More recently, however, these techniques have regained attention given their value in maintaining the keystone area and dorsal aesthetic lines.
Surgical Techniques
Preservation rhinoplasty refers to several components of rhinoplasty, including (1) elevating the nasal soft tissue in a subperichondrial–subperiosteal plane, (2) limited excision of alar cartilages, and (3) maintaining the osseocartilaginous dorsum without violation of the bony–cartilaginous interface. 19 The latter, preservation of the dorsum, can be performed with or without the other elements. Although a large majority of DP surgeons describe an endonasal (closed) technique, an external (open) approach can also be performed.15,18–20 Furthermore, use of piezoelectric instruments after wide subperiosteal dissection, as is the senior authors preference, may be helpful for precise osteotomies.
Management of the bony pyramid
The PD and LD techniques fundamentally differ in the approach to the bony nasal pyramid.14,18,20–23 In the PD technique, lateral and transverse osteotomies are performed to allow for en-bloc mobilization of the bony vault (Fig. 1). In the LD operation, similar osteotomies are performed, however, a wedge of bone at the frontal process of the maxilla is removed (Fig. 2). 9 Placement of the resection in the nasofacial groove reduces the risk of visible step-off deformity. In addition, the resection of bone can be performed using a closed approach (with a bone rongeur, manual saw, or needle holder) or in an open manner (using osteotomes or piezoelectric instruments).18,20
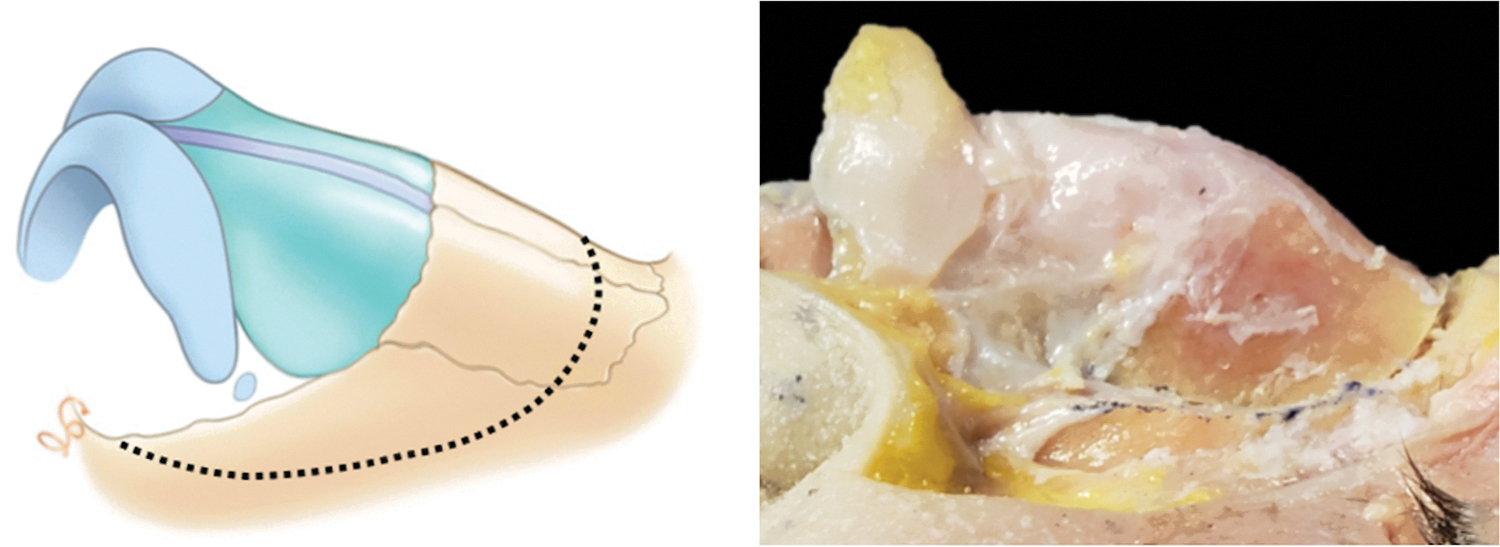
In the pushdown technique, lateral and transverse osteotomies are performed to allow for en-bloc mobilization of the bony vault as shown schematically on the left and on a cadaver on right.
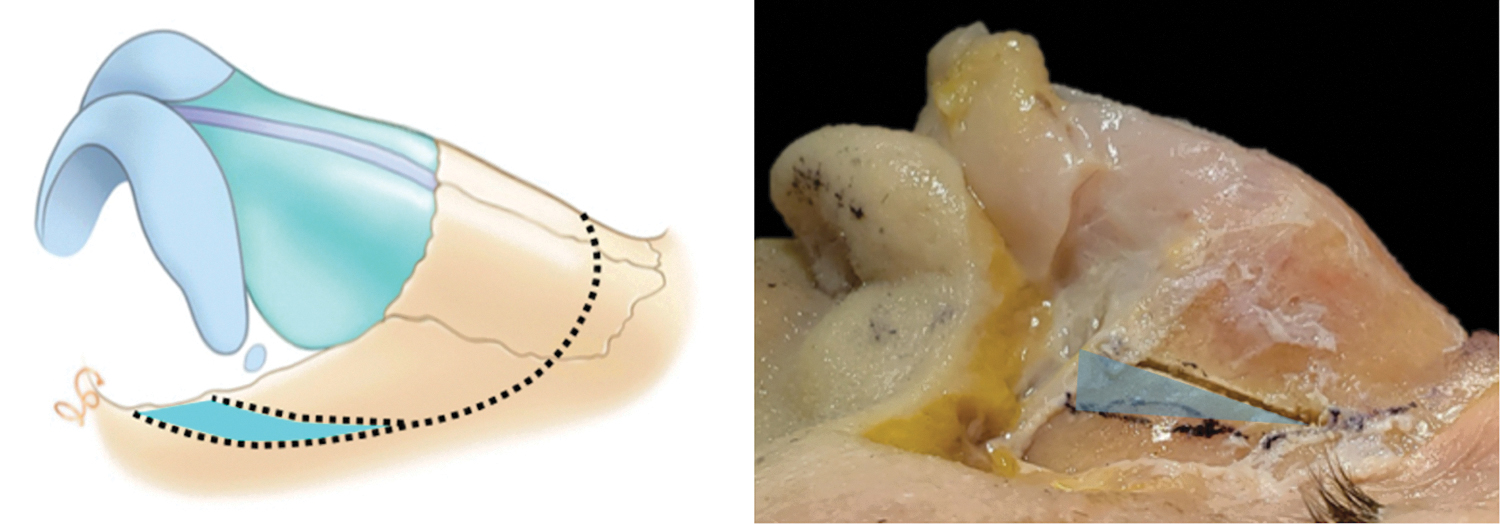
In the LD operation, lateral and transverse osteotomies are performed similar to the PD procedure, with the addition of a second lateral osteotomy that allows for a wedge of bone to be removed at the frontal process of the maxilla. This is shown schematically on the left and on a cadaver on right (wedge of bone to be resected is highlighted in blue). LD, letdown; PD, pushdown.
The decision to use either the LD or PD technique may depend on several factors. If the dorsal hump is >4 mm, a PD technique may not be adequate for the needed descent of the nasal pyramid. Therefore, the LD technique has been advocated for humps >4 mm. 24 In preliminary cadaveric studies at our center, we have found that the PD technique has a narrowing effect on the INV. 25 This is not seen with the LD operation. Whether this has clinical relevance for patients is an area of ongoing research and may have implications for the selective use of the LD over the PD technique.
Management of the septum
Regardless of whether the LD or PD technique is used, resection of the nasal septum is required to allow for dorsal lowering. A variety of approaches to the septum exist, each differentiated by the location of cartilage resection (Fig. 3).
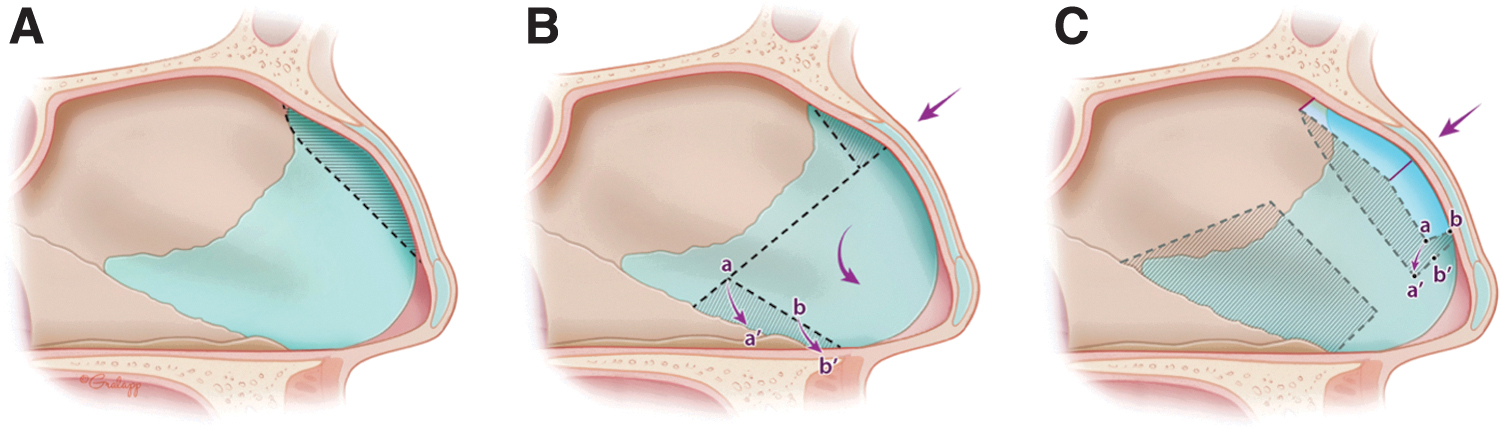
Goodale's and Lothrop's original descriptions involved a subdorsal cartilage resection, and this technique has been further developed by others including Gola and Saban (Figs. 3A, 4, and 5).9,15,17,18 In this approach, an incision is made immediately under the dorsum, following the contour of the dorsal hump.18,19 A lower cut is then made such that it corresponds to the new height and contour of the intended profile. The intervening cartilage is removed and dictates the degree of dorsal reduction.18,24 A small amount of subdorsal ethmoid bone is resected using a rongeur, scissors, or osteotomes. Any remaining septum on the undersurface of the osseocartilaginous vault may be scored to release any tension that would prevent dorsal flattening. When the nasal vault is lowered, the dorsum can be fixed into position by placement of sutures. 19
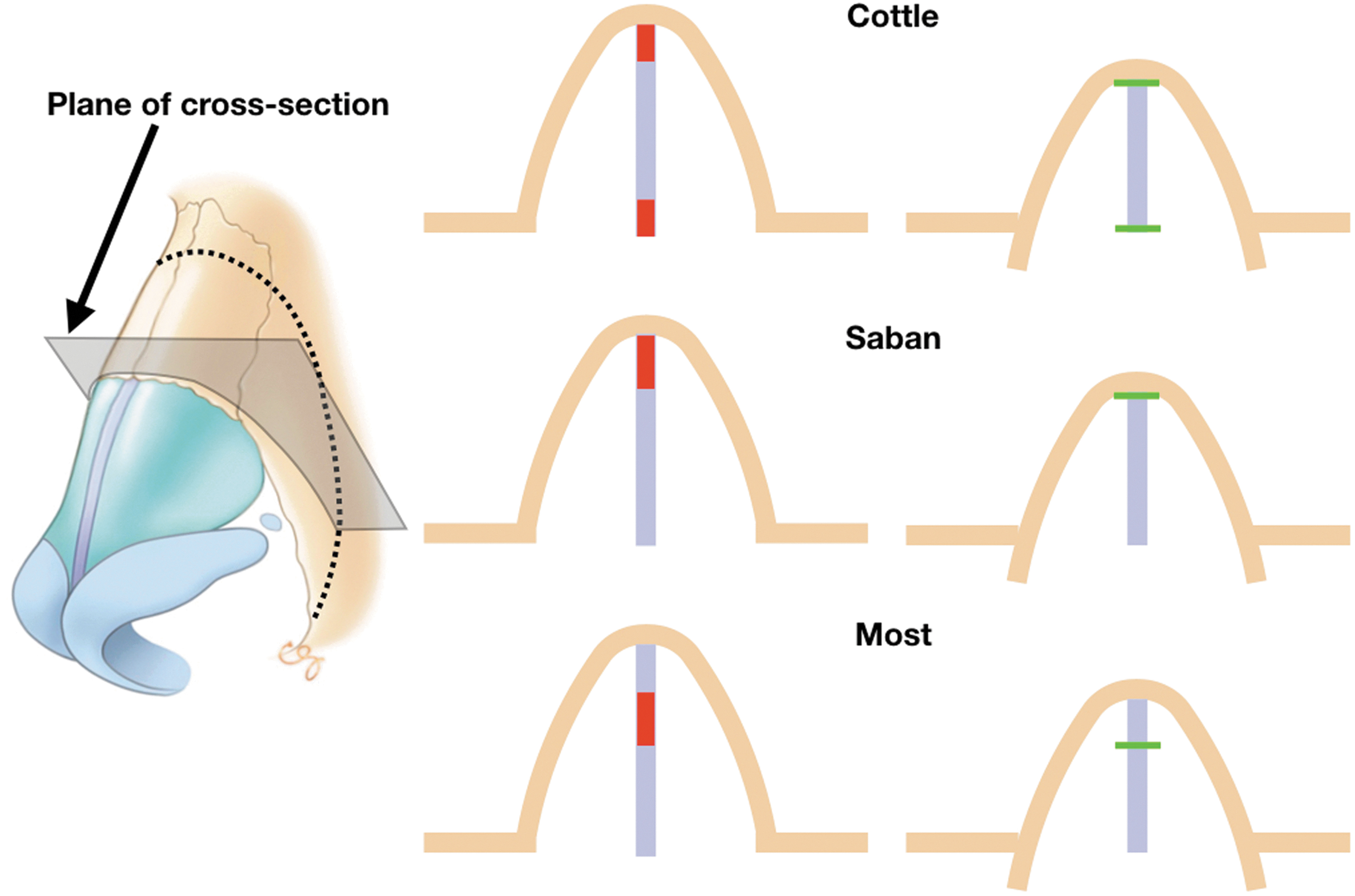
On the left side, 3/4 view of the nose indicates the osteotomy sites for a PD procedure, including area of bony resection, shown in red. The plane of section shown schematically on the right in indicated. Top row: Cottle method, middle row: Saban method, bottom row: senior author's method. Red marks on left column indicate areas of septal and bony resection. Green lines on right column indicate corresponding junctions after inset of nasal pyramid.
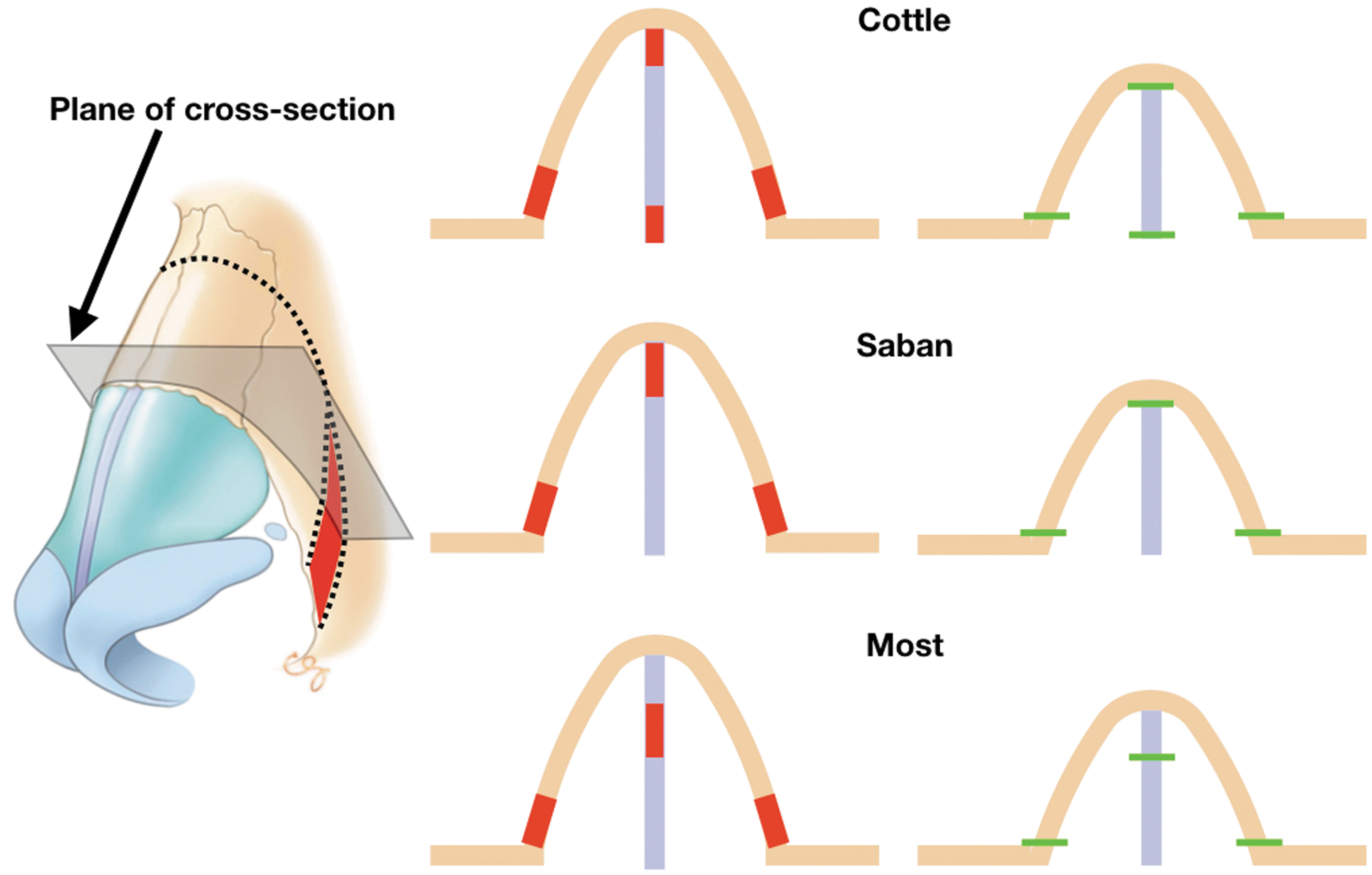
On the left side, 3/4 view of the nose indicates the osteotomy sites for a LD procedure, as well as the plane of section shown schematically on the right. Top row: Cottle method, middle row: Saban method, bottom row: senior author's method. Red marks on left column indicate areas of septal resection. Green lines on right column indicate corresponding junctions after inset of nasal pyramid.
Ishida et al. have described a septal strip excision that is performed closer to the midaspect of the septum (rather than subdorsal). 5 This extends into the caudal aspect of the septum inferior to the anterior septal angle. The osseous septum is left intact. The cartilaginous nasal vault is mobilized inferiorly, and the nasal bones are reduced using an osteotome or rasp. As such, this differs from other DP techniques in which the nasal bones and cartilaginous midvault are treated as a single unit.
An alternative to subdorsal cartilage resection was described by Cottle. This classically consisted of a three-part resection (Figs. 3B, 4, and 5): (1) vertical 4 mm segment at the bony–cartilaginous junction (from keystone to vomer), (2) triangular resection of the ethmoid bone, and (3) inferior strip of cartilage along the maxillary spine (corresponding to the amount of desired dorsal reduction). The remaining nasal septum is sutured to the maxillary spine. This technique may limit the amount of harvestable cartilage for other maneuvers in rhinoplasty.
The senior author has developed a modified septal technique that may be considered an intermediate between the subdorsal and inferior septal resections (Figs. 3C, 4, and 5). In this technique, a high-septal resection is performed, leaving a 3–5 mm subdorsal strut of cartilage. The cut is started posterior to the anterior septal angle, allowing for the preservation of a 1–1.5 cm caudal strut (Fig. 6). A minimal release of the caudal aspect of the upper lateral cartilages (ULCs) allows for improved visualization of the septum and ultimately unimpacted lowering of the dorsum with a caudal strut still in place. A portion of ethmoid bone can either be removed or a longitudinal cut into the bony septum can be performed without resection. To allow for depression and flexion of the dorsum, one or two vertical incisions are made into the subdorsal cartilage at a location that corresponds to the apex of the dorsal hump (Fig. 3). The subdorsal cartilage is then flexed and anchored to the remaining inferior cartilage (Fig. 6). In contrast to the Cottle method, this allows for more reliable resection of the lower septum for purposes of correcting deviations and grafting purposes.
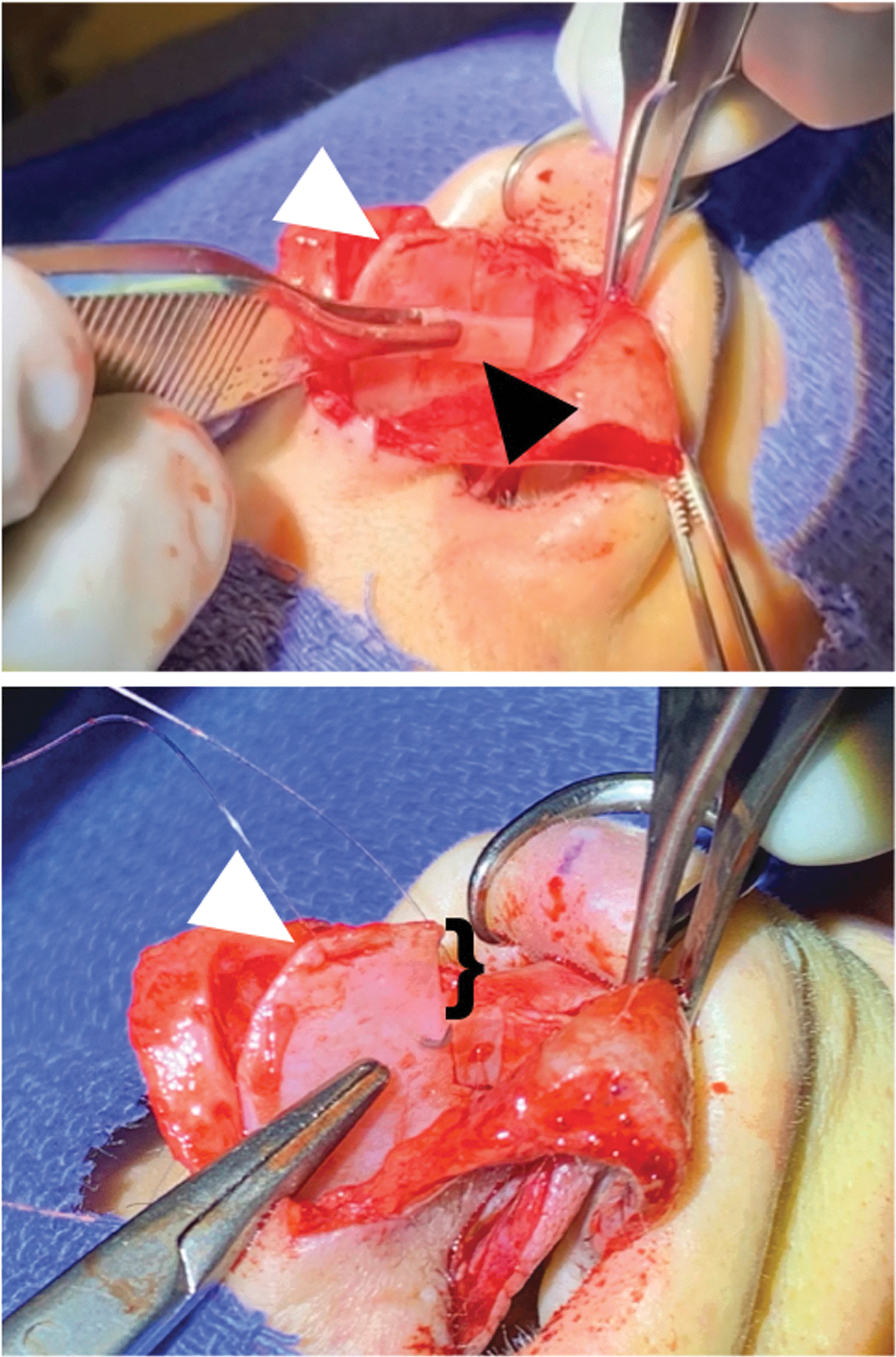
Intraoperative views of midsectional septal resection, as described by the senior author. In the top image, the upper midseptal strip resection (black arrow) is shown in the forceps, in the process of removal. In the lower image, the dorsal segment of cartilage is shown sutured to a new lower position. The drop in dorsal height, as measured on the preserved caudal septal strut, is indicated. White arrow indicates the anterior septal angle in both images.
Most importantly, this technique allows for a caudal strut that remains anchored to the maxillary spine without the need for attempts to stabilize the septum to bone (allowing for subsequent tip stabilization). In addition, spreader grafts may be placed with this method. In comparison with subdorsal resection techniques, the septal resection does not extend to the anterior septal angle (caudal septum remains entirely intact). This can be trimmed secondarily or left in the original more projected location to allow for adjustment of the tripod complex. Finally, in the event that the caudal strut has to be removed (e.g., anterior septal reconstruction), keeping a subdorsal strut of cartilage allows the new caudal strut to be stabilized to the dorsum.26,27
Indications
Interestingly, Saban notes that 41% of his patients still undergo conventional Joseph hump resections. 18 In general, DP is limited to primary cases and in patients with a moderately kyphotic hump. 20 However, if a patient has had a prior DP procedure, a secondary procedure using similar techniques is possible. 24 Patients with tension noses or a predominance of cartilage and shorter nasal bones are also considered good candidates for DP surgery. Those with a greater bony component, deep nasofrontal angle, or irregular bony pyramid are considered poor candidates for DP. 18 However, in an open approach in which a radix graft can be placed and with the use of ultrasonic rhinoplasty saws that allow for gentle correction of subtle irregularities, a greater number of patients may benefit from DP techniques.
Straight deviations in the nose can be addressed with an asymmetric wedge resection of bone in an LD procedure. However, in the setting of a high-septal deviation, a standard Joseph hump takedown can be considered if the side of the septal deviation is away from the side of the nasal bone deviation (Fig. 7). In this favorable scenario, after a hump takedown, the nasal bone can be mobilized medially toward the deviated septum. In an unfavorable scenario, the septum deviates to the same side as the deviated nasal vault, and thereby limits how much the nasal bone ipsilateral to the deviation can be medialized (if doing a standard hump takedown). Here, a LD procedure would be preferred in our practice.
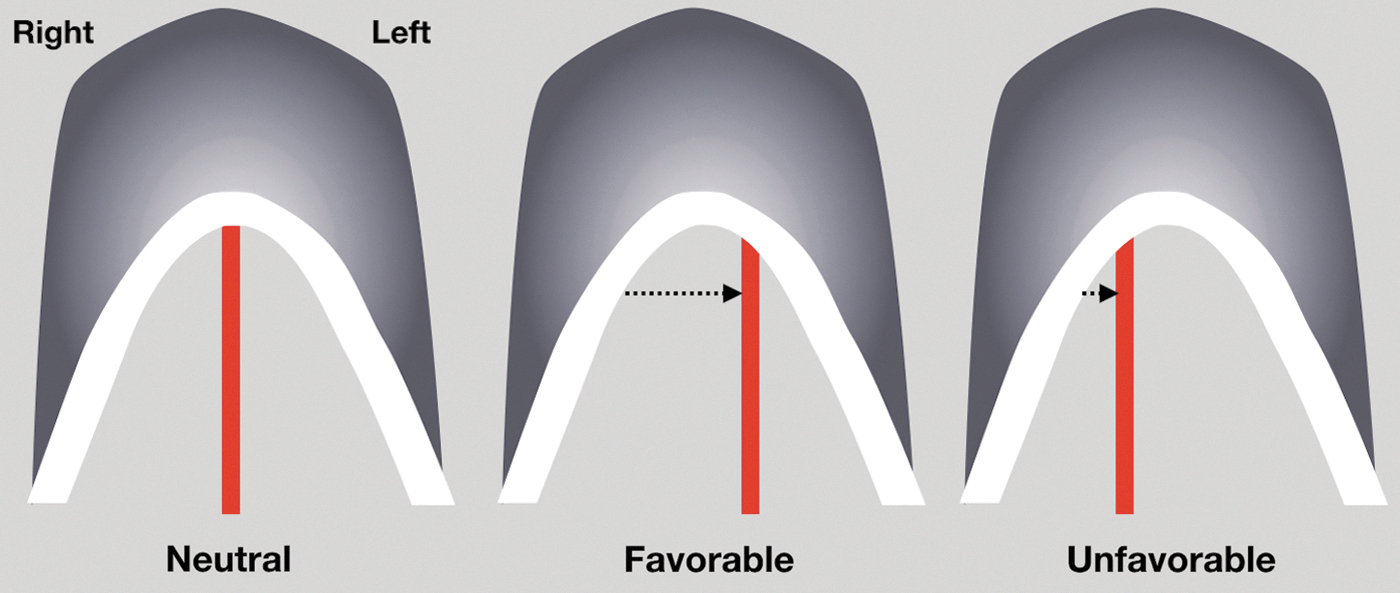
On a sagittal view, if attempting to mobilize the nasal vault to the left, a favorable and unfavorable configuration of the septum and nasal bone relationship is shown. In the favorable scenario, the side of a septal deviation is in the same direction of the desired nasal bone movement and, therefore, the nasal bone can be effectively mobilized medially toward the deviated septum. In an unfavorable scenario, the septum deviates opposite to the side of intended nasal bone movement and thereby limits how much the nasal bone can be medialized. A standard hump takedown (with effective medialization of the nasal bones) can be employed with success in favorable scenarios, whereas a LD procedure is preferred in unfavorable scenarios.
Surgical Outcomes and Challenges
Despite our recent implementation of DP techniques, we have found that it has resulted in consistent maintenance of dorsal aesthetic lines with successful reduction of dorsal humps. DP prevents the irregularities that can arise with osteotomies to close open-roof defects and prevents the need for midvault reconstruction. Using the modified high-septal technique, an open approach, and piezoelectric instruments has allowed for precise osteotomies and septal cuts without the need for endoscopic visualization. Although there is slight tip rotation with this technique, an open approach allows for the exposure and ability to modify the tip with previously used strategies (i.e., suture modification and cephalic trim). Thus, the modified high-septal resection method through an open approach allows for combining preservation and structural rhinoplasty concepts. Figure 8 shows 6-month postoperative results of two patients undergoing this technique.

Representative photographs of two patients undergoing a LD procedure with a high-septal resection technique. Improvements in external nasal contour with dorsal reduction are noted when comparing preoperative (left) and 6-month postoperative (right) images.
Several authors have shared their success with DP techniques; however, robust patient-reported outcomes or nasal airway measurements are lacking. Gola provides a comprehensive description of DP with the subdorsal resection technique and states that he has had immense functional and aesthetic success in a series of >1000 patients, but does not include any subjective or objective data. 16 Saban et al. have reported on 320 patients undergoing endonasal DP surgery (PD and LD) with endoscopic subdorsal septal resection. 18 A “definite improvement” in nasal respiration was reported by 309 patients. Thirty patients were given the Nasal Obstruction Symptom Evaluation questionnaire, and of these, 90% reported improvements in nasal breathing.
Tuncel and Aydogdu reported on 520 patients undergoing successful closed PD or LD surgery with subdorsal cartilage resection. 24 Ishida et al., using a midseptal cartilage strip resection technique without preservation of the dorsal keystone, note satisfactory functional and aesthetic results in a series of 120 patients. 5 No patient-reported measures or evaluation of nasal obstruction is discussed in either of these studies.
At our center, early experience with 16 patients who underwent DP rhinoplasty (8 LD, 8 PD) has demonstrated excellent aesthetic and functional outcomes at last follow-up (mean ± SD: 117 ± 63 days). Seven of these patients underwent a combined functional and aesthetic operation, including two patients who underwent an anterior septal reconstruction (which is possible with the high-septal resection technique). In each patient, the validated standardized Cosmesis and Health Nasal Outcomes Survey with an obstructive (SCHNOS-O) and cosmetic (SCHNOS-C) domain was recorded pre- and postoperatively (scores ranging from 0 to 100, 0 being no obstruction or no aesthetic concerns).28,29
Preoperatively, the mean (SD) SCHNOS-O and SCHNOS-C scores were 39.4 (29.7) and 62.3 (18.0), respectively. Postoperatively, the scores significantly improved to 20.3 (15.8, p = 0.003) and 6.9 (10.9, p < 0.001), respectively. Similar comparisons were made in patient visual analog scale (VAS) results including a functional scale (0–10, 0 being no obstruction) and a cosmetic scale (0–10, 0 being no satisfaction with appearance): preoperatively mean (SD) functional and cosmetic VAS scores were 3.9 (3.0) and 2.6 (1.4), respectively, and improved to 1.94 (1.7, p = 0.016) and 8.8 (1.1, p < 0.001) postoperatively. No patient experienced any short-term complication including epistaxis, infection, or aesthetic deformity (saddling or persistent hump).
The recurrence of a dorsal hump with DP surgery is an important long-term consideration. In patients who underwent a midlevel septal strip resection, Ishida et al. report a 15% partial hump recurrence rate. 5 Saban, who reports a lower hump recurrence rate (3.4%), has suggested that keeping a subdorsal cartilaginous strut is, in part, responsible for this since (1) precise evaluation of the amount of dorsal lowering required is more difficult and (2) even a small residual amount of subdorsal septum prevents the shape of the dorsum from changing. 18
However, Tuncel and Aydogdu, in a series of 520 patients, report a 12% rate of hump recurrence with a subdorsal resection technique. 24 The authors recommend a subperichondrial/subperiosteal dissection, scoring any small amount of the septum remaining at the keystone area, performing lateral keystone dissection, and considering the LD procedure over the PD technique as means to prevent a hump relapse. As would be expected, larger humps have a greater risk for recurrence. In the high-septal strip resection described here, a vertical cut performed through the remaining subdorsal cartilage at the apex of the hump, lateral disarticulation of the ULC and the ascending process of the maxilla, and multiple suture fixation of the dorsum (and subdorsal cartilage) to the lower septum are means to prevent recurrence of the dorsal hump.
In the senior authors early experience, a technical challenge has been prevention of excessive posterior displacement of the upper nasal vault (i.e., the radix). As the entire nasal vault is disarticulated through osteotomies and septal separation from surrounding rigid structures, it is possible that this segment can over mobilize. Anteriorly, this is limited as the ULC fusion (in the subdorsal resection techniques) or the subdorsal cartilage (in the high-septal resection technique) rests on the underlying septum. If this occurs at the osseous nasal pyramid, deepening of the radix, or a palpable step-off may occur. To prevent this, the senior author makes a longitudinal cut into the ethmoid bone rather than resecting a segment of the bone. If this does occur, a radix graft using soft tissue or morselized cartilage may be used for camouflage.
Although DP techniques are employed primarily for ensuring a superior aesthetic outcome and reduction of midvault reconstruction required, there is a suggestion that they may be superior with regard to compromise of the INV.18,20 A comparison between these techniques, however, has not been performed and is an ongoing area of research at our center. Based on anatomical considerations, the PD technique, which involves the advancement of the bony nasal pyramid medial to the piriform aperture, could theoretically result in nasal obstruction more so than the LD technique. Preliminary data from cadaveric studies at our institution support this idea. Therefore, consideration of the technique employed in DP, particularly in patients with baseline functional complaints, may prevent postoperative nasal obstruction. More robust series with patient-reported outcomes are needed to better evaluate functional outcomes with DP.
Conclusions
With the recent revitalized interest in DP, an understanding of the potential benefits, techniques, and challenges associated with this surgery is helpful. Maintenance of the dorsum as a single unit has implications for maintaining structural integrity at the nasal keystone, pleasing dorsal aesthetic lines, and the patency of the INV. Technical modifications, such as the high-septal excision discussed herein, allow for a variety of approaches to DP. As surgeons continue to develop and employ these techniques, critical assessment of patient-reported outcomes and objective nasal measurements, with an emphasis on comparison with standard hump takedown techniques, will be valuable.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.