
Abstract
During the COVID-19 pandemic, nonpharmaceutical public health interventions (NPIs) were implemented worldwide to control the spread of severe acute respiratory syndrome coronavirus 2. However, the incidence of other pathogens, including gastrointestinal (GI) pathogens, was also affected. Here, we reviewed studies assessing the impact of NPIs during the COVID-19 pandemic on the incidence of GI infections, particularly foodborne infections. A systems literature search was conducted in May 2023, using Living Evidence on COVID-19 (COAP) and Scopus. Articles were identified and selected through a screening process with inclusion and exclusion criteria based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement. Data were extracted from each full-text article included in the review. Parameters included were GI viruses, GI bacteria, NPIs against the COVID-19 pandemic, and the associated impact of NPIs on GI pathogens. A total of 42 articles were included in the review, representing 18 countries. Overall, a larger reduction was observed for viral GI infections compared with bacterial GI infections during the COVID-19 pandemic, particularly for norovirus. For bacterial GI infections, Campylobacter and nontyphoidal Salmonella were the most frequently detected pathogens in the majority of the studies, with the largest reduction observed for Shigella and Shiga toxin–producing Escherichia coli infections. The sharp decrease in GI viral infections in most of the included countries is suggested to be related to the disruption of person-to-person transmission due to several implemented interventions (e.g., social distancing and hand hygiene). GI bacterial pathogens, more commonly transmitted via the foodborne route, were least impacted, and their reduction is associated with closure of food-providing settings and travel restrictions. However, the observed changes appear to be multifactorial; alterations in health-care-seeking behaviors and in routinary diagnostic testing have undeniably played a significant role, affecting national surveillance systems. Therefore, although NPIs likely had a substantial impact on the burden of GI infectious diseases, the extent of the true change cannot be fully assessed.
Introduction
Since the beginning of 2020, public health authorities and healthcare providers called to control the coronavirus disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). In the early stages of the epidemic, when no vaccines were available yet, several nonpharmaceutical public health interventions (NPIs) were implemented, such as social distancing, mask mandates, travel restrictions, school and restaurant closures, as well as quarantine measures to control the spread of SARS-CoV-2. Although the target of such NPIs was SARS-CoV-2, changes in the transmission of other pathogens, including those causing mainly respiratory, sexually transmitted, and gastrointestinal (GI) infections, were also observed (Middeldorp et al., 2021; Mughini-Gras et al., 2021; Soo et al., 2020; Ullrich et al., 2021). Moreover, different prevention and control measures were applied at national and regional levels in different countries, depending on the specific evolution of the epidemic (Antunes et al., 2020).
Commonly applied control measures (e.g., handwashing, social distancing, travel restrictions) can also prevent the transmission of GI pathogens (Palmer et al., 2022). Therefore, it has been suggested that some of the measures implemented during the COVID-19 pandemic could explain the observed reduction in GI pathogen transmission as well. A significant decrease in most notifiable diseases, including those caused by GI pathogens, during the COVID-19 pandemic has been well documented in Germany (Ullrich et al., 2021), with similar results being reported in China (Chen et al., 2021), the United States of America (USA) (Ray et al., 2021), and other countries, mainly across Europe.
Transmission of GI pathogens typically follows the fecal−oral route, with consumption of contaminated food or water being often the main transmission pathway, as well as contact with infected individuals, animals, or the environment (Love et al., 2022). Among the main GI bacterial pathogens responsible for GI infections are Campylobacter, Salmonella, Listeria monocytogenes, and Shiga toxin–producing Escherichia coli (STEC), which are mostly associated with foodborne tranmission (Russini et al., 2022), as well as Shigella, which is mainly transmitted directly from person to person and indirectly through contaminated food and water in developed countries (Bassal et al., 2021). The main viral agents of gastroenteritis include noroviruses and rotaviruses, which are also mainly transmitted from person to person, but have a foodborne route as well (Nachamkin et al., 2021; Russini et al., 2022). Understanding the extent to which the measures against SARS-CoV-2 also affected GI infections might significantly contribute to the identification and implementation of prevention strategies to control these pathogens. Moreover, different countries might have adopted different approaches in different periods to control SARS-CoV-2 spread; thus, differences in the potential effects of these measures can be expected.
This scoping review aims to synthesize current evidence that measures implemented against SARS-CoV-2 worldwide had also a significant effect on the incidence of GI infections, particularly foodborne infections.
Methods
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement. This set of guidelines applied.
Literature search
A systematic literature search was conducted in May 2023 using two online search databases: Living Evidence on COVID-19 (COAP) which includes research about SARS-CoV-2 and COVID-19 up until February 28, 2022, and Scopus. The databases were searched using the following keywords in Title/Abstract: ‘‘covid-19 measures,” “covid-19 restrictions,” “covid-19 lockdown,” “COVID-19 pandemic,” “gastrointestinal infectious diseases,” “gastrointestinal infections,” “gastrointestinal pathogens,” “foodborne diseases,” “foodborne infections,” “foodborne pathogens,” “Campylobacter”, “Salmonella,” ‘‘STEC’’, “Listeria,” “Shigella,” “Norovirus,” and “Rotavirus.” A manual search was also performed using Scopus for identifying additional articles, aimed to support the choice and selection of the presented articles (Table 1).
Search Strategy for Online Search Databases
Selection process
Selection of articles was done independently by two researchers who screened titles, abstracts, and finally full-text articles using the following inclusion criteria: (1) studies referred to NPIs against SARS-CoV-2 and their impact on foodborne diseases, foodborne pathogens, GI diseases, or GI pathogens in general; (2) studies referred to the specific foodborne and GI pathogens mentioned in the used search terms; (3) studies reported on the incidence or case counts of foodborne and/or GI diseases; (4) articles were written in English; and (5) articles included the period of the COVID-19 pandemic, specifically from January 2020 to May 2022. The snowballing method was also used to identify articles that had not appeared in the original search by applying the same inclusion and exclusion criteria. As a result, a total number of n = 42 articles remained and used in this report. Figure 1 shows a detailed outline of the selection process.
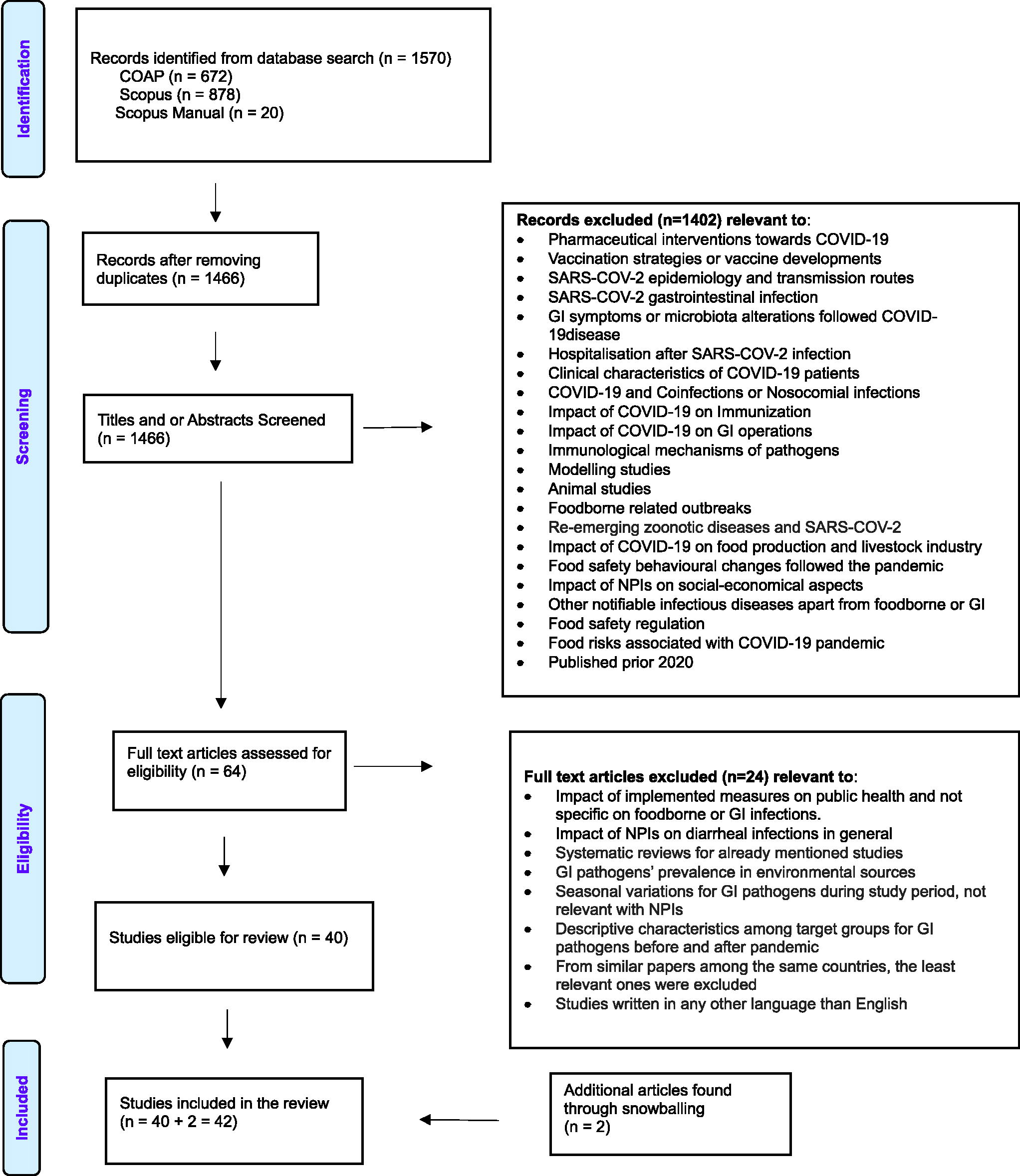
PRISMA flow diagram for study selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Data synthesis
Data were extracted from each full-text article included in this review. The following information was collected: (1) general details, such as author, design of the study, and country; (2) information on the specific GI pathogens, the impact of the COVID-19 pandemic on each pathogen (percentage change in incidence and/or case country compared with pre-COVID-19), per study; and (3) the investigated time period of each study. Data were entered in Microsoft Excel (version 2211).
Results
The initial dataset comprised 1466 articles, from which 42 articles were selected for inclusion in this review (Fig. 1). Studies predominantly addressed GI viruses, specifically norovirus (n = 19) and rotavirus (n = 7), and GI bacteria, including Campylobacter (n = 13), nontyphoidal Salmonella (n = 15), Salmonella Typhi/Paratyphi (n = 4), Shigella (n = 13), STEC (n = 7), and Listeria (n = 5). Four studies offered broader insights into infectious diarrheal diseases, overall GI complaints, or viral GI infections. Six (n = 6) out of the 41 studies examined the impact of the pandemic on GI viruses in hospitalized children.
Table 2 provides an overview of investigated GI pathogens per article by region and country, and Table 3 describes their main outcomes, data source, and study period.
Counties Included in This Review and the Investigated Gastrointestinal Pathogens per Country and Study
EIA, enzyme immunoassay; STEC, Shiga toxin–producing Escherichia coli.
Overview of the 41 Mentioned Studies in This Review, the Investigated Gastrointestinal Pathogens, and the Main Outcomes
Outcomes are associated with the study design and study period, used per study. We report the percentage change for every pathogen in the given comparison period, and it was calculated by us when it was not mentioned in the individual studies, if possible. Investigated pathogens are highlighted in bold (n/c: noncalculated by referenced study or us).
EIA, enzyme immunoassay; STEC, Shiga toxin–producing Escherichia coli; SIP, shelter-in-place.
GI viruses and observed trends, by world region
Observed trends in the pacific
In Australia, during the period of stringent measures (March 15 to May 15, 2020), a 67% reduction in rotavirus incidences was observed in the Northern Territory compared to the corresponding period of the previous 5 years (Xie et al., 2020). Meanwhile, in Central Queensland, Adegbija et al. (2021) reported a 91% reduction in rotavirus notifications from April 1 to September 30, 2020, compared to the same months in the previous 5 years. Examining norovirus outbreaks in Victoria during January–September 2020, Bruggink (2022) observed a 49% decline in outbreaks compared to the same period of the previous decade, although a subsequent increase was noted in 2021.
Observed trends in North America
Analyzing outbreak data in the USA, Lennon et al. (2020) reported a 49% decrease in weekly norovirus outbreaks in February–June 2020 compared to the same months in 2019. In Philadelphia, Nachamkin et al. (2021) observed that the percentage of norovirus positivity stool went from 3.9% during 2016–2019 to 1.4% from March through December 2020. In Texas, Palmer et al. (2022) reported an immediate decrease in norovirus PCR positivity percentage in the week that social distancing was mandated, based on laboratory data from nine states. Moreover, Kambhampati et al. (2022) saw that the number of norovirus outbreaks in 12 states decreased three-fold during the 2020–2021 surveillance years and returned to prepandemic levels in 2021–2022. In Northern California, Bulterys et al. (2021) noted a 79% and 55% decrease in positive norovirus and rotavirus laboratory tests, respectively, during March–September 2020, compared to pre-COVID-19 years. Last, Burnett et al. (2022) reported a 73% and 85% decline in rotavirus enzyme immunoassay positivity and PCR positivity, respectively, between 2007–2019 and 2020–2021.
Observed trends in Western/Northern Europe
In Germany, Eigner et al. (2021) reported a consistently low monthly positivity rate for norovirus-positive samples from May to December 2020 (nearly 0%), contrasting with rates of 4–11% in May to July 2019. Ullrich et al. (2021) reported substantial decreases in rotavirus (−83%) and norovirus notifications (−79%) between weeks 10–32 in 2020 compared to the same weeks in 2016–2019. Furthermore, 3- to 20-fold lower positivity ratios were reported for norovirus by Mack et al. (2021) based on laboratory data from a large regional laboratory in Western Germany. The ratio for rotavirus was also lower but not statistically significant. Terliesner et al. (2022) observed that the mean monthly rate of children who tested positive for rotavirus in the Berlin University Children’s Hospital decreased by 87% from January to May 2020 compared to the same prepandemic period. They also reported an absence of seasonality, with no increase after withdrawal of NPI measures in June 2021, but a slight increase corresponding to the prepandemic seasonality in January 2021. Between February and November 2020, almost no cases of rotavirus were reported by Maison et al. (2022) at their pediatric clinic. However, after the second lockdown ended in March 2021, a rise in rotavirus cases outside the usual season was observed, comparable to the number of cases in 2019. During 2020, an increase in positive norovirus infections was observed compared to prepandemic years (2017–2019), while during the summer of 2021, these infections were detected slightly more frequently compared to previous years since 2017–2020.
Love et al. (2022) reported a 38% decrease in norovirus laboratory-confirmed cases in 2020 in England, compared to 2015–2019. Hayes et al. (2023) described a substantial drop in norovirus cases during the first lockdown, with less than 10 weekly cases compared to a weekly 50–200 cases in 2018. They remained low until restrictions were eased.
In Finland, Kuitunen et al. (2022) reported a 70% lower incidence of norovirus detections in primary care for gastroenteritis in 2020 and a 46% lower incidence in 2021 compared to 2018–2019 in children aged 0–14 years. A 64% and 72% lower incidence was observed for rotavirus in 2020 and 2021, respectively. The incidence of norovirus remained low throughout 2020 but experienced a rapid increase in March 2021, surpassing the prepandemic levels. Rotavirus cases, however, remained at low levels.
Observed trends in Southern/Central Europe
From March 15, 2020, to March 15, 2021, a 69% and 49% decrease in prevalence and relative incidence, respectively, was observed for norovirus in hospitalized children with viral gastroenteritis in Spain, compared to the same period prepandemic Maldonado-Barrueco et al. (2022). For rotavirus, the prevalence and relative incidence decreased by 67% and 40%, respectively.
In Poland, Czerwińska and Szenborn (2020) observed a 63% drop in rotavirus, norovirus, and adenovirus cases from January 1, 2020, to March 15, 2020, compared with corresponding data from 2019.
Observed trends in Southeastern Europe—Western Asia
Duman et al. (2022) reported a 35% reduction in the monthly median positivity rate of rotavirus among children admitted to hospitals in Turkey between April 2020 and July 2021 in comparison to January 2018 to March 2020.
Observed trends in (South) East Asia
In South Korea, a significant 40% and 32% reduction was observed in the incidence of norovirus and rotavirus, respectively, following the implementation of pandemic measures from March 2020 to February 2021, compared to the same period in 2018–2019 (Ahn et al., 2021).
Hibiya et al. (2022) reported a 94% reduction in norovirus incidence in 2020 in Japan compared to the same period in 2019. In addition, Fukuda et al. (2021) described findings from a multicenter study, where they found a marked decrease in viral gastroenteritis (28% for norovirus and 3% for rotavirus) among hospitalized children during the post-COVID-19 period (July 2020–February 2021) compared to the prepandemic period (July 2019–February 2020).
A significant 5.56-fold increase in rotavirus cases in Thailand was observed by Yorsaeng et al. (2022) during early 2020 compared to 2019, which significantly declined during and after the lockdown in 2020. After an initial spike in early 2020, significantly less norovirus cases were observed compared to the same weeks of 2019, especially during the easing and new wave periods.
In China, Wang et al. (2022) observed that the monthly incidence rate of GI diseases and viral GI diseases decreased by 45% and 64% in 2020, respectively, compared to 2015–2019. Li et al. (2021) reported a 50% reduction in the positivity rate of rotavirus in Children’s Hospital in Hangzhou in 2020 compared to 2019. In the work of Chan (2022), the positivity rates for GI viruses in Hong Kong were lower in early 2020 compared to 2013–2019, most notable for rotavirus with a 70% reduction, and a 56% decrease for norovirus. In January 2021, however, norovirus and rotavirus rates were back at prepandemic levels. In Southern China, Lu et al. (2021) reported a 23% decrease in infectious diarrhea cases from January to August 2020, compared to the same time period in 2015–2019. However, after schools reopened in September, the number of cases was higher than pre-COVID-19.
GI bacteria and observed trends, by world region
Observed trends in the Pacific
In the Northern Territory of Australia, Xie et al. (2020) reported a 42% and 19% reduction from March 15, 2020, to May 15, 2020, in nontyphoidal Salmonella and Shigella monthly incidence, respectively, compared to the same period in 2019. Davis et al. (2022) described a reduction in nontyphoidal Salmonella notifications of 27% in 2020, compared to the previous 5 years. In Central Queensland, Adegbija et al. (2021) reported 26% and 8% less disease notifications for nontyphoidal Salmonella and Campylobacter, respectively, during the first 6 months of 2020, while the number of STEC notifications remained the same compared with the previous 5 years.
Observed trends in North America
Based on national surveillance data, Ray et al. (2021) described a decrease in incidence of foodborne enteric infections in 2021 compared to 2017–2020, caused by Campylobacter (−23%), Salmonella (−22%), STEC (−37%), Shigella (−41%), and Listeria (−27%). In 2021, the incidence was only significantly lower for Salmonella (−10%), but to a lesser extent (Collins et al., 2022). In Canada during 2020, there was a noted decrease in the number of reported cases for Salmonella, Shigella, Escherichia coli O157, and non-O157 STEC compared to the previous 5-year period, with the number of reported cases for Listeria monocytogenes in 2020 remaining consistent with those from the previous 5 years as reported by Dougherty et al. (2023). In Philadelphia, Nachamkin et al. (2021) described a reduction of Campylobacter, nontyphoidal Salmonella, and Shigella in March–May 2020, which then restored to prepandemic levels. In California, a 50% decrease in Shigella’s positivity rate was detected by Bulterys et al. (2021) after shelter orders took place in 2020. On the contrary, the rate for Campylobacter, Salmonella, and STEC infections remained largely unaffected.
Observed trends in Western/Northern Europe
In the Netherlands, Mughini-Gras et al. (2021) observed a significant decrease in nontyphoidal Salmonella cases based on national surveillance data, which ranged between 55% and 37% depending on the quarters of 2020 and 2021 compared with 2016–2019.
Love et al. (2022) described a decrease in GI laboratory-confirmed cases during weeks 1–31 of 2020 in England. Particularly nontyphoidal Salmonella, Shigella, and Campylobacter showed a substantial decrease, and no decrease was observed for STEC and Listeria compared to the previous 5 years. Hayes et al. (2023) also reported a lower number of Shigella cases in England during the pandemic from March 2020 to February 2022.
A 22% reduction of nontyphoidal Salmonella cases and a 45% reduction of Campylobacter cases were reported by Ullrich et al. (2021) in Germany. However, the largest reduction was observed for Shigella, with an 83% decrease.
In Denmark, the number of nontyphoidal Salmonella and Campylobacter cases decreased by 53% and 30%, respectively, as described by Nielsen et al. (2022).
Observed trends in Central/Southern Europe
In Switzerland, the number of Shigella, nontyphoidal Salmonella, and Campylobacter cases in 2020 decreased by 82%, 41%, and 59%, respectively, compared with 2016–2019 (Steffen et al., 2020). In addition, the number of typhoid and paratyphoid Salmonella cases was reduced by 50%.
The transmission of Campylobacter and nontyphoidal Salmonella was suppressed during the COVID-19 pandemic in Spain, with a number of infections being reduced by 70% and 75%, respectively, in 2020, compared to 2019 (de Miguel Buckley et al., 2020).
Observed trends in East Asia
Lai et al. (2021) demonstrated an overall 23% reduction in the incidence of 8 out of 11 investigated notifiable fecal–oral transmitted infectious diseases in Taiwan from January to September 2020 compared to 2019. Specifically, the number of cases for paratyphoid fever, typhoid fever, and listeriosis were reduced by 100%, 65%, and 23%, respectively, while a slight increase was observed for shigellosis.
Lin et al. (2021) also reported a 58% and 100% decrease in the number of typhoid and paratyphoid Salmonella cases in 2020 compared with the past decade.
In South Korea, Ahn et al. (2021) revealed that the Campylobacter incidence was either similar or higher in some months of 2020 compared to the previous 5 years, while Salmonella rates decreased but not significantly. On the contrary, Kim et al. (2022) showed a 59% reduction in the cumulative incidence among children over 3 months until 18 years of age with an invasive Salmonella infection during weeks with restrictive measures.
In China, a statistically significant 25% decrease in typhoid fever and paratyphoid incidence rates was described by Chen et al. (2021) in 2020 compared to 2019, and a 36% reduction in the monthly incidence rates of typhoid fever in 2020 compared to the previous 5-year average by Wang et al. (2022).
Observed trends in the Middle East
In Israel, an 86% reduced incidence of Shigella was observed in Israel during March–July 2020 compared to 2018–2019, followed by a lower 33% and 30% reduced incidence for Salmonella and Campylobacter (Bassal et al., 2021).
Discussion
Studies included in this review showed marked changes in GI pathogen incidence during the COVID-19 pandemic across 18 countries. The incidence of viral GI infections seemed to have decreased more relative to that of bacterial GI infections. This may reflect the relatively more important role of person-to-person transmission in the epidemiology of those viruses, as most NPIs for SARS-CoV-2 were indeed meant to reduce contact between people. Differences in analytical methods, study designs, and periods may explain some of the different outcomes observed among studies. To our knowledge, this is the first review on the effect of the COVID-19 pandemic on the incidence of foodborne pathogens.
GI viruses and NPIs
The sharp decrease in norovirus and rotavirus infections observed in most studies is often mentioned to be likely related to disruptions in the usual fecal–oral (transmission) route due to constraints in contact between people, especially among children during periods of school closure, among others. The number of hospitalized cases due to GI viruses typically increases during the winter, reaching a peak between January-March in the northern hemisphere (Eigner et al., 2021). However, a steep decrease in the incidence of these viral infections was observed during the winter of 2020 in most studies. As assumed by several authors, a combination of social distancing, remote work and study, increased hand hygiene and cleaning in general, and face masking have been suggested to hinder the transmission of GI viruses too (Adegbija et al., 2021; Ahn et al., 2021; Chan, 2022; Czerwińska and Szenborn, 2020; Duman et al., 2022; Eigner et al., 2021; Hayes et al., 2023; Li et al., 2021; Love et al., 2022; Maldonado-Barrueco et al., 2022; Nachamkin et al., 2021; Ullrich et al., 2021; Wang et al., 2022; Xie et al., 2020; Yorsaeng et al., 2022). Norovirus is also highly contagious through the consumption of contaminated food and water, giving opportunities for frequent outbreaks in institutions and restaurants (Eigner et al., 2021). Similarly, domestic and international border closures prevented the importation of cases from endemic countries, closure of restaurants and other institutions, as well as restricted classroom-based education among children (Bulterys et al., 2021; Eigner et al., 2021; Ullrich et al., 2021; Xie et al., 2020) appeared to have contributed as well. Eigner et al. (2021) also suggested preventing behavioral changes preceding the restriction measures in Germany (i.e., social distancing measures, hand sanitizers) as a justification for the decrease in positivity rates already from February, thus 1-month prior to the implementation of these measures. Specifically for young children, the main suspect of the decreased viral incidence for norovirus and rotavirus is the reduced child-to-child contact as the result of the closing of classrooms and playgrounds, as suggested by Maldonado-Barrueco et al. (2022) in Spain and by Fukuda et al. (2021) in Japan.
With the lifting of control measures, multiple countries reported an increase in the number of rotavirus infections (Kambhampati et al., 2022; Li et al., 2021). The increase in norovirus outbreaks during the first quarter of 2021 in Australia was predominantly associated with childcare settings (Bruggink, 2022). Outbreaks in healthcare settings in Australia (including aged care) were fairly limited at that time, while prior to the COVID-19 pandemic, the majority of outbreaks were attributed to healthcare settings. Bruggink (2022) associated this shift in the outbreak demographics with increased compliance in personal protective equipment by healthcare workers and restriction in visitors, but also with reduced diligence of young children around hand hygiene. Also, other countries reported the return of rotavirus and norovirus activity to pre-COVID-19 levels after an initial decrease, which is suspected to be due to waning immunity that led to an increased susceptible population, while measures were still in place (Chan, 2022; Love et al., 2022).
GI bacteria and NPIs
Bacterial pathogens faced relatively less significant decreases in incidence during the COVID-19 pandemic. Generally, Campylobacter and nontyphoidal Salmonella had lower reductions compared to Shigella and STEC infections. The highest reduction of shigellosis could be due to the predominant transmission route in some countries, that is, person-to-person, compared to salmonellosis and campylobacteriosis, which are most often foodborne (Bassal et al., 2021; Dougherty et al., 2023; Love et al., 2022). Therefore, most arguments previously suggested for the viruses (e.g., social distancing, increased hygiene) would also apply to Shigella (Bassal et al., 2021; Lai et al., 2021). The shift toward preparing food at home due to stay-at-home orders, along with less eating out, fewer social gatherings, improved handwashing, and the implementation of safer food handling practices, likely contributed to the reduction in Campylobacter and nontyphoidal Salmonella infections (Nachamkin et al., 2021; Ray et al., 2021; Xie et al., 2020). Moreover, the closure of restaurants and food service providers in schools, hotels, and catering businesses may have also contributed to decreased exposure (Davis et al., 2022; Steffen et al., 2020).
Since GI infections can often be acquired abroad while traveling, several studies also highlighted the contribution of entry and travel restrictions (e.g., international or non-essential national traveling) in the reduction of bacterial pathogens (Collins et al., 2022; Lin et al., 2021; Love et al., 2022; Mughini-Gras et al., 2021; Nielsen et al., 2022; Ray et al., 2021).
The return of bacterial GI pathogen incidence to pre-COVID-19 levels in some countries, only a few months after implementing the measures, cannot be fully explained (Nachamkin et al., 2021). A possible reason could lie in their normal yearly variations (Xie et al., 2020) and their typical increasing trends during summertime (Bassal et al., 2021). However, the variety of potential transmission pathways makes it difficult to identify the causative factors (Ahn et al., 2021).
Additional factors besides NPIs explaining changes in GI pathogens
Although NPIs undoubtedly decreased the number of GI infections, the reasons behind the detected changes are complex and multifactorial. Other factors include changes in healthcare-seeking behavior, as shown by a drop in general practitioner and emergency department visits, as well as less hospital admissions due to diseases other than COVID-19. This was coupled with high pressure on diagnostic services and reduced healthcare capacity, leading to potential under-ascertainment and under-reporting of GI infections (Bassal et al., 2021; Burnett et al., 2022; Collins et al., 2022; Dougherty et al., 2023; Eigner et al., 2021; Lennon et al., 2020; Love et al., 2022; Ullrich et al., 2021). Even though a change in eating habits may have occurred, that is, people ate more often at home, individuals still remained at risk for foodborne infections, supporting the aforementioned hypothesis of under-ascertainment and underreporting (Ullrich et al., 2021).
Most importantly, during public health emergencies, the efficacy of routinely services might be negatively affected. For instance, a reduced ability to properly conduct public health surveillance and outbreak investigation, especially for foodborne outbreaks, was reported in the USA (Kintziger et al., 2021). Because most notification systems depend on infectious disease diagnoses by physicians and laboratories (Ullrich et al., 2021), disruptions in their way of working and patient behaviors might impact the number of cases captured by the systems. Therefore, the extent of the true change in GI infection incidence attributed to NPIs or these other factors cannot be fully discerned.
Limitations and future research
While our study provides a comprehensive overview of the impact of NPIs on GI infections during the COVID-19 pandemic across various countries, there are some limitations that should be taken into consideration. First, world regions were not equally represented in this review, since no studies were included from Africa and Central and South America. Therefore, findings may not reflect all continents. Second, the reported changes in incidence and other epidemiological metrics were analyzed in the context of the periods during which the NPIs were implemented per study. However, we did not report the specific timing, duration, or strictness of each measure across different regions, which also impacted the reported changes in incidence. Third, the search terms used in this review were chosen to target specific pathogens (e.g., STEC instead of the broader term E. coli) to maintain a clear and precise focus on the study’s objectives and to avoid many articles matching the search terms that would not be relevant. However, it may have led to the exclusion of some relevant studies that used broader terms to define, for example, STEC. Fourth, studies that were published after the data extraction in May 2023 may have offered additional insights or revealed different trends that were not captured in this review.
In order to determine the effects of specific NPIs on foodborne disease incidence and herewith insight into the importance of specific pathways, such as the closure of food establishments, future studies could group together countries and/or periods with similar type and strictness of NPIs. Comparison should take into account the differences in public health infrastructure, surveillance systems, and diagnostic practices across different countries and regions. However, because measures such as travel restrictions and closure of food establishments were likely often implemented at the same time, it can be difficult to determine their independent effect on the incidence of foodborne pathogens.
As the world moves to a post-COVID-19 pandemic period, ongoing surveillance of GI pathogens is needed to monitor whether the observed reductions during the pandemic are sustained or whether incidence rates return to prepandemic levels. For example, increased circulation of some foodborne pathogens could occur due to increased population susceptibility and could last several years, as was predicted for norovirus (Lappe et al., 2023).
Conclusions
A substantial reduction in the incidence of reported GI infections appears to have occurred during the COVID-19 pandemic, with a relatively larger impact on viral vs. bacterial GI pathogens. This is most likely due to the generally higher proportion of viral vs. bacterial infections acquired through person-to-person contact instead of, for example, foodborne transmission, as the implemented NPIs were meant to control SARS-CoV-2, a virus transmitted by person-to-person contact. However, the reasons behind these observed reductions remain difficult to discern at full, as they are likely to be multifactorial in nature. Other factors, such as disruptions in healthcare-seeking behaviors and diagnostic practices, may have also played a significant role in the observed trends. Consequently, the extent of the reduction attributed to NPIs cannot be fully determined. Nonetheless, findings provide insights into which and how potential interventions might also help controlling GI pathogens.
Footnotes
Authors’ Contributions
A.L.: Methodology, data curation, and writing the original draft. L.M.-G.: Conceptualization, methodology, reviewing and editing, and supervision. R.P.: Conceptualization, methodology, data curation, review and editing, and supervision.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding has been received for this review.