
Abstract
Background:
The need to study and understand cumulative impacts, the combined influence of chemical and non-chemical stressors on health and quality of life, is becoming increasingly recognized. The goal of this study is to understand how residents in fenceline communities experience the cumulative impacts of pollution and other non-chemical stressors on their physical and mental health and to develop meaningful policy solutions to mitigate the harms caused by these cumulative burdens.
Methods:
We used a community-based participatory research (CBPR) approach, partnering with residents in southern Delaware County, PA, experiencing environmental injustice, to design and conduct focus groups. Our focus groups aimed to better understand how residents characterize stressors related to their environmental, physical, and mental health. We used a deductive/inductive hybrid data analysis method to distill the most significant findings from the focus groups.
Results:
We conducted focus groups with residents (n = 22) of four Southeastern Pennsylvania fenceline municipalities. Participants discussed chemical (e.g., air pollution and odors) and non-chemical stressors (e.g., lack of access to green spaces) influencing their physical and mental health. Participants also described how these stressors are interconnected and worsen their health and quality of life. Participants identified solutions (e.g., policy change and community organizing) to mitigate the most pressing stressors.
Discussion:
This study is the first in the area to work alongside community investigators to understand how residents in fenceline communities experience cumulative impacts. Our findings were presented to key community stakeholders to inform future advocacy work to mitigate the cumulative burdens faced by these fenceline communities.
INTRODUCTION
Traditional risk assessment methods have long served as the foundation of environmental decision making in the interest of public health protection. These methods, however, are limited in their ability to consider the collective effects of co-exposures to multiple chemicals, and wholly inadequate in accounting for the added burden of other, non-chemical stressors. 1 A burgeoning body of evidence suggests that non-chemical stressors (e.g., violence, stress, lack of social support, or low socioeconomic status) 2 can also exacerbate a person’s response to chemical exposures. 3
Cumulative impacts are “the totality of exposures to combinations of chemical and non-chemical stressors and their effects on health, well-being, and quality of life outcomes,” 4 The U.S. Environmental Protection Agency (U.S. EPA) recognizes these effects and the limitations of current regulatory approaches to environmental chemical exposures. In response to Executive Orders 13985 and 14008, the U.S. EPA is strengthening the scientific foundation for assessing cumulative impacts and has made prioritizing research in this area a priority. In 2023, the U.S. EPA released Draft Proposed Principles of Cumulative Risk Assessment for evaluating chemicals under the Toxic Substances Control Act. While this represents an important step toward integrating cumulative risk assessment of chemical mixtures into regulatory policy, to date, these principles have not been finalized. 5 The U.S. EPA also supports the practice of cumulative impact assessment, which encourages the consideration of qualitative and quantitative data and encourages direct community engagement in the process of assessing cumulative impacts and making decisions.
While some research studies have used qualitative methods to convey and elevate the complex experiences of communities impacted by environmental and social health concerns,6,7 qualitative research is overall an important but often underutilized method in environmental health research. Specifically, qualitative methods are instrumental for improving how we understand complex exposure pathways 8 and how social factors may impact environmental health and health outcomes. 9 Qualitative methods are also appropriate for exploring explanatory questions (e.g., characterizing how or why certain perceptions or social factors may impact behaviors 10 or health outcomes).
Southern Delaware County, PA, is home to a disproportionate concentration of industrial sources of pollution, including two incinerators and numerous chemical manufacturing and petrochemical processing facilities near residential areas (Fig. 1). 11 Like many states, the Pennsylvania Department of Environmental Protection (PA DEP) grants permits individually to industrial facilities to emit up to a specified amount of hazardous air pollutants each year. 12 Though other states (e.g., New Jersey) 13 now consider the cumulative impacts of emitting facilities in overburdened fenceline communities. The PA DEP’s current regulatory and permitting approach for stationary point sources of air pollution does not consider the co-occurrence and concentration of facilities in a given area, 14 which may exacerbate poor air quality in areas and contribute to elevated pollutant exposures and poor health outcomes in neighboring communities (hereafter: fenceline communities). 15 A community health assessment conducted in early 2024 found that the City of Chester had some of the highest rates of infant mortality and certain respiratory diseases in the Commonwealth of Pennsylvania. 16 In addition to environmental pollution, southern Delaware County residents also share concerns about water safety11 and often face numerous non-chemical stressors associated with poor health such as poor housing conditions, food insecurity, and lack of reliable transportation.2 These communities have high proportions of residents who live below twice the federal poverty level, lack health insurance, and experience housing burdens (i.e., pay over 50% of their income on housing costs). 17 As of 2023, most municipalities in Southern Delaware County are classified as environmental justice areas according to PennEnviroScreen, a novel screening methodology created by the PA DEP to identify communities facing the highest levels of environmental pollution and social vulnerabilities.17,18
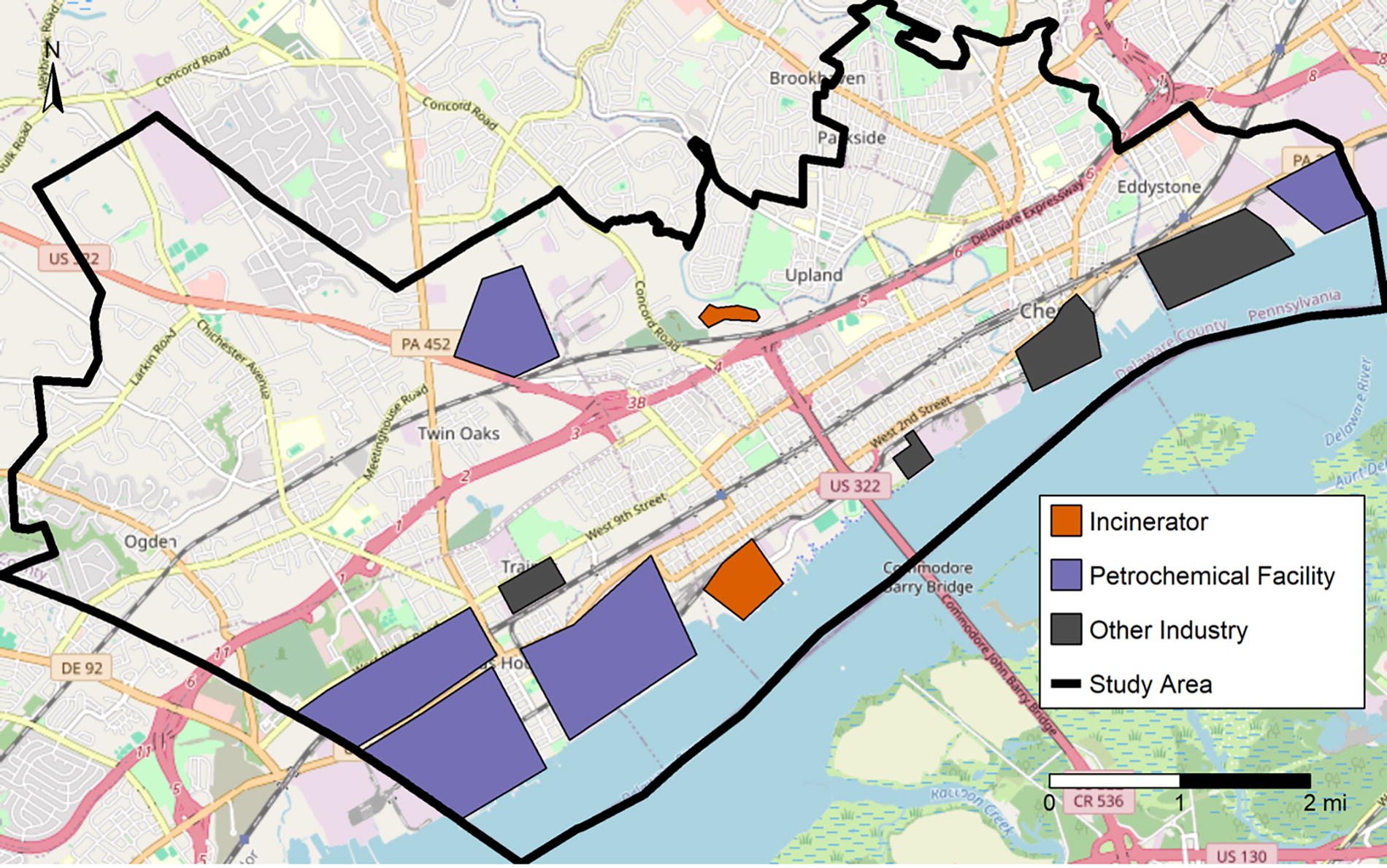
Map of Southern Delaware County study area.
This study is a component of a broader mixed methods study (i.e., The Assessing Strengths, Stressors, and Environmental justice in SoutheaStern Pennsylvania communities [ASSESS PA] Study), which aims to collect data to improve our understanding of community strengths, stressors, and needs and to describe the cumulative impacts of chemical (e.g., exposure to air pollutants) and non-chemical (e.g., economic hardship) stressors in southern Delaware County fenceline communities. The ASSESS study was implemented in two phases: (1) the development and implementation of a community-based environmental health survey and (2) convening of focus groups to further explore topics included in the survey. The publication of this article follows the notification of and invitation of residents, community leaders, and policy makers to an open meeting aimed at discussing the broader ASSESS study findings and how they can be used to further advocacy efforts to mitigate harm and improve health. In this article, we describe our community-based participatory research (CBPR) approach for conducting focus groups to characterize how residents experience the cumulative impacts of chemical and non-chemical stressors on their physical and mental health and explore strength-based community-generated solutions to mitigate the cumulative burdens they face.
METHODS
CBPR approach
Our multidisciplinary team was committed to a CBPR approach.19,20 Academic investigators at Johns Hopkins University (JHU) worked as equal partners alongside community investigators from the Clean Air Council (CAC) and Marcus Hook Area Neighbors for Public Health (MHNFPH), who are also impacted residents, on all parts of the scientific process, including the conception of project plans, funding acquisition, study design, data collection, data analysis, and interpretation. The CAC, established in 1967, is a member-supported non-profit organization based in Philadelphia that uses a broad array of related sustainability and public health initiatives, using public education, community action, government oversight, and enforcement of environmental laws. Established in 2020, MHANPH is a non-partisan community-based organization dedicated to protecting the health and safety of local communities from toxic pollution. Members are community residents concerned about the cumulative impacts of pollution on local health caused by local refineries, petrochemical plants and other industrial infrastructure. Most members are from the environmental justice areas of Marcus Hook, Chester, Trainer and Upper/Lower Chichester. The group meets approximately monthly and aims to educate the community and coordinate opportunities for resident participation in public health and environmental permitting processes at the state and local levels. Throughout the research process, all investigators convened at least once every 2 weeks to design and implement the ASSESS study.
Participant recruitment
In late 2023, we designed and implemented a community environmental health survey to collect information from residents about their exposures to chemical and non-chemical stressors to quantitatively assess the breadth of chemical and non-chemical stressors among respondents. One hundred forty-three participants completed the initial survey. The final question of the survey asked participants to indicate their interest in participating in a follow-up focus group. Seventy-two participants indicated they were interested and were contacted and invited to participate in a focus group. Twenty-two of these participants agreed to participate in the focus groups. All focus group participants had satisfied the eligibility criteria for the initial survey (i.e., ≥18 years of age and residence in any of the following municipalities: Boothwyn, Chester Township, City of Chester, Eddystone, Linwood, Marcus Hook, Ogden, Parkside, Trainer, Twin Oaks, Upland, and Upper Chichester). We had representation from three municipalities: Chester, Marcus Hook, and Trainer. Chester is an urban/suburban community with 32,605 residents, 70%–85% of whom identify as African American alone or mixed races, and a median income of $39,193. 21 Marcus Hook Borough is a community with a population of 2,433 people, 65% of whom identify as White, and a median income of $47,594.21 Trainer Borough is a residential/industrial community home to 1,976 people, 56% of whom identify as White, and the median household income is $83,906.21
Data collection
A focus group discussion guide was developed collaboratively with the broad research team (Supplementary Data). Open-ended questions (including pre-determined probes) were asked in a similar order to all focus group participants. These questions encouraged participants to explore the key contributors to their physical and mental health and how those factors interact and impact their well-being. Participants were asked to consider solutions to the concerns raised during each discussion. A few examples of discussion questions are: “What are the most pressing issues affecting the environment in your community?” “What factors influence your mental health?” “How do these fit together?”
Each focus group was facilitated by a community investigator (i.e., the facilitator). A different community investigator served as a note-taker, and an academic investigator was present for technical support and other needs. The facilitator obtained oral consent from each participant before recording the discussion. To protect participants’ privacy, all were encouraged to use pseudonyms for the duration of the discussion and were permitted to participate without their video.
The academic investigator used a Google Jamboard to record key themes and ideas discussed during the focus group to facilitate the discussion. The Jamboard was visible to all participants via the Zoom screenshare function throughout the focus group. The facilitator, notetaker, and technical support person were familiar with the focus group guide and had successfully completed Basic Human Subjects Research training requirements from the JHU Institutional Review Board. Participants were offered a $50 gift card after completing the focus group session.
Data management and analysis
The focus groups were recorded and transcribed using Zoom's automatic transcription function. Each transcript was reviewed and cross-checked with the audio recording for accuracy. Audio recordings and transcripts were stored on a password-protected server only accessible to the research team. We anonymized the focus group transcripts prior to coding and analysis.
We used ATLAS.ti Version 23 (Berlin, Germany) to support the analysis of the focus group transcripts, employing a hybrid inductive and deductive thematic analysis approach.
We identified different thematic codes we anticipated finding in the focus groups. These a priori codes were informed by our research questions and from input from the diverse study team. We developed a codebook to support the identification and classification of these codes.
Two investigators reviewed transcripts following the steps outlined in the Framework Approach, 22 a five-step process designed to support qualitative research. These steps including becoming familiar with the transcripts, developing and refining the thematic codes, charting and organizing the data, and interpreting the findings. After initial familiarization, the two researchers independently coded a subset of the transcripts (approximately 10% of the transcript material) using the initial codebook. The coding was then compared and reconciled through consensus. Through this process, the codebook was further refined, and emergent codes were identified. The balance of the transcripts was then coded independently by both of the researchers. After all the transcripts were coded, the researchers met to discuss the codes, review, and refine the themes. The final version of the codebook was shown to community investigators and each code was described. All investigators were given time and space to provide constructive feedback. These feedback sessions held between March and April 2024 helped the data analysis team identify and interpret the main themes present in the data.
The themes presented aimed to represent multiple perspectives, and for a theme to be identified as “key,” we tried to analyze how robust the conversation was between participants. As a team, we had regular discussions surrounding what themes were recurring. We decided to conclude the focus groups after conducting six sessions as the discussions continued to focus on similar themes. At this point, the remaining invited participants had not responded to our invitations or indicated they were no longer interested in participation.
Ethical considerations
All human subject research study tools and protocols were reviewed and approved by the Johns Hopkins Institutional Review Board (IRB00024902).
RESULTS
Study participants
Twenty-two residents participated in a total of six focus groups (Table 1) via Zoom between January and February 2024. Participants predominantly identified as female (82%) and non-Hispanic White (55%). The 22 participants were residents of Chester, Upper Chichester, Marcus Hook, or Trainer municipalities. Participants ranged in age from 20 to 71 years (mean = 49; standard deviation = 14 years) and had resided in the area for between 1 and 59 years (mean = 28 years; standard deviation = 19 years). Each focus group discussion lasted 52–87 minutes (mean = 67.5 minutes; standard deviation = 15 minutes).
Summary of Participants’ Demographic Characteristics (n = 22)
Findings by Theme
We present four themes that emerged from the six focus groups: (1) environmental influences on physical and mental health, (2) economic and social influences on physical and mental health, (3) cumulative impacts, and (4) community strengths and solutions. To provide further insight on these ideas, we use a combination of summarized data and illustrative quotes to elucidate further the key themes identified.
Environmental influences on physical and mental health
Participants identified a variety of physical and mental health concerns impacting themselves and other community members. Key physical health concerns included respiratory diseases, symptoms (e.g., headaches), and chronic diseases (e.g., cancer, diabetes). The most frequently identified mental health concerns were stress, depression, and anxiety. Participants highlighted shared environmental stressors, both chemical and non-chemical, in their community that they attribute their negative physical and mental health impacts (Table 2). Odors and air pollution/poor air quality were the environmental stressors discussed most often and in the greatest detail as a main influence. For example, participants described odors and air pollution as inescapable, pervasive, and impacting their daily activities, physical health, and well-being.
Summary of Participants’ Most Pressing Environmental Stressors in Their Community and Their Impact on Physical and Mental Health
“…there's an awful smell like rotten eggs”—Participant 6
“Asthma, COPD, bronchitis. I've had pneumonia of unknown origin… different things like that. I feel like with the dust and the… air quality, I feel like it's a significant detriment to breathing conditions.”—Participant 17
“And then you're in a house because it's not even like it's a fleeting smell… It could be an hour. It could be three. So you're kinda putting your life on hold, trying to be as safe and healthy as possible.”—Participant 22
Non-chemical environmental stressors were also brought up. Noise was discussed as a concern by several participants.
“Well… it's [the car park] right off my backyard! So they’re about a mile behind our houses here, and the noise just it. It gets unbearable at times.”—Participant 10
Lack of access to adequate green spaces was discussed in several focus groups:
“But they’re [green spaces] just too few and far between and spread so far out… that you really have to have transportation and everything else to… access those different things.”—Participant 17
Participants also noted that even when they wanted to go outside and had access to green spaces, sometimes they avoided it due to environmental concerns, such as the poor air quality. This conflict presents a conundrum that some participants acknowledged: they can go outside and breathe in the polluted air, or they can stay inside and remain socially isolated. These sentiments illustrate the kinds of difficult decisions that fenceline communities face daily.
“I think it comes back to air quality for me. I think most of the issues that I have that would be caused from the environment would be just those bad odors, and then almost always having nausea or a headache on those days… really kind of eliminate being able to get outside and… participate in physical activity because of it just doesn’t seem safe to, especially… with kids, you can’t take them outside to play because you don’t want them sucking up all this this odor into their lungs, not knowing really what it is.”—Participant 5
Most importantly, participants explicitly linked how chemical and non-chemical stressors directly impact their physical and mental health symptoms and diagnoses simultaneously, illustrating how these factors can (and often) act together to worsen health (Table 2). Table 2 summarizes selected salient statements previously mentioned and explicitly link each to the related health impacts.
Economic and social influences on physical and mental health
Participants identified non-chemical stressors in their communities and their life circumstances that can negatively impact their physical and mental health. Many participants noted that lacking financial and other resources to support health is a significant source of stress in their lives.
“Not having a job, you know, not being able to afford your rent and stuff, that could also lead to depression. You’re just trying to figure things out pretty much, and you can cause yourself to be anxious.”—Participant 20
“It’s hard to have good mental health when you’re stressing about health care.”—Participant 13
Focus group participants also noted physical harm associated with the lack of accessible healthy foods in their communities.
“We don’t have the proper stores to shop in to get fresh fruits, fresh items, and processed food is part of what’s killing us.”—Participant 8
Some participants also expressed continued feelings of social isolation brought on by the COVID-19 pandemic, highlighting the need for targeted efforts to address this ongoing vulnerability.
“I think the Covid has had a big issue with the community, and our mental health as well. We’re much more isolated, or at least I am. I don’t attend a lot of social indoor functions. I think that takes away from your support system.”—Participant 7
This list is not exhaustive, and other non-chemical stressors were brought up during the six focus group sessions the ASSESS study team conducted, including housing, crime and safety, and education.
Cumulative impacts
Several participants explained how environmental, physical, and mental health stressors are not isolated but connected and overlap. Participants further noted how these stressors often interact with each other and highlighted the nuance of the compounding effects of these influences on their well-being. They explained how these impacts can often lead to one another, sometimes having a cyclical nature:
“I think all of them play a part together and separately. If you have bad soil because of the refineries, or the air quality doesn’t give plants the nutrients that [they] need… that’s going to affect the food that you make and the food that you eat. It’s [going to] make you have asthma and not be able to go outside, and because there’s no fresh air to enjoy, so I think all of them play a part and interconnect with each other.”—Participant 2
“If you’re not physically healthy, your mental health is affected, and vice versa: if your mental health is not healthy, [it] can affect your physical health, which also ties into, you know, being able to sustain a job to get that income that you need to obtain the resources to be healthy. It really just all ties in together. We always separate the two [physical and mental health], but it really is a combination that is a domino effect each way…”—Participant 4
One participant also expressed that with everything going on around them [the large number of industrial facilities], it felt as if they “live in the Bermuda Triangle” (Participant 17), meaning it felt as if living in their communities was dangerous, reflecting the theories of missing ships and planes surrounding the infamous Bermuda Triangle. 23
Another participant noted how the interaction of multiple stressors often require them to prioritize one health concern over another.
“The pollution is very pressing, but if you get shot, then you don’t have a chance. If you are killed or maimed, so that that seems worse than the pollution. Although the pollutions insidious… other communities don’t live in this kind of fear”—Participant 19
Given the harsh realities communities in southern Delaware County are enduring, some participants believed there were community concerns and threats greater than pollution.
Participants also emphasized a disconnect between what resources are needed and the resources that are provided to address them, specifically highlighting the inequities they perceive:
“But when things happen in in more affluent areas, the counselors show up. They stay there, they get wraparound services, etc… That doesn’t happen when you’re in what they call the “hood,” or places that aren’t necessarily affluent. They just… everybody shows up and just thoughts and prayers, and that’s the end of it. But it’s gonna take more than just thoughts and prayers for us to really increase the mental health of these smaller communities or communities. We have to really put boots on the ground, put resources on the ground.”—Participant 5
Community strengths and solutions
Despite the environmental, physical, and mental health challenges, participants identified numerous strengths and assets in their communities. Participants expressed pride in their community’s diversity, small-town feel, and the care embedded in interpersonal community connections. Participants in this area stay because neighbors are swift to support and show up for one another when they encounter challenges:
“The thing that I’m most proud of in our community is just how, if somebody needs something, everybody will rally around and get it for them. We’ve had … people who have gone through medical issues, and the community just comes together. And they do beef and beers [fundraisers]. They… do 50/50 [raffle] tickets. They will come together to… make sure that everybody has what they need, and that’s one of the big reasons why I stay here and why, my kids will stay here until who knows when.”—Participant 2
Most participants emphasized how they felt supported in their communities:
“… [It’s] small and everyone knows everybody. And for the most part, everyone looks out for each other”—Participant 20
Ultimately, most participants wanted policymakers to prioritize protecting these communities from further industrial emissions by capping the amount of pollution and limiting the construction of new industrial facilities. We present Table 3 to demonstrate the different solutions prioritized by this community, and provide examples provided by residents themselves. Recognizing these communities’ strong connections, four types of solutions to achieve this shared goal emerged from the focus group discussions. These community-driven solutions included (1) investment in community resources and advocacy, (2) policy action to prevent future industrial development, (3) better planning and transparency to protect communities against harm, and (4) community coalition-building to help enact these changes (Table 3). These solutions demonstrate the communities’ continued commitment to leveraging their greatest strength (i.e., their ability to work together and help each other when in need).
Summary of Focus Group Participant-Identified Solutions
DISCUSSION
We used a CBPR approach to explore how residents of a fenceline community experience and describe the cumulative impacts of chemical and non-chemical stressors. This study is among the first to work alongside community investigators to qualitatively explore how chemical and non-chemical stressors impact residents’ health and well-being. Participants described how environmental concerns directly impacted their well-being and quality of life, making direct links to respiratory conditions (e.g., asthma) and other diseases/health conditions such as cancer, diabetes, depression, and anxiety. Participants also described the compounding effects of environmental, physical, and mental health stressors in their communities. They characterized their experiences of cumulative impacts in ways that highlighted the synergistic qualities of chemical and non-chemical stressors: the sum of the stressors combined is more impactful than simply adding each together. On top of this, at multiple points in our focus groups, we noted a recurring theme: when faced with multiple harsh realities, several participants described making trade-offs between various health-related concerns. Specifically, as outlined in the Environmental Influences on Physical and Mental Health section through the discussions surrounding spending time outside and breathing polluted air, or staying inside and experiencing social isolation, participants appeared to make decisions with a “lesser of two evils” sentiment in mind. Similarly, as described in the Cumulative Impacts section, when discussing how violence and pollution are experienced side-by-side, sometimes pollution seemed less risky to residents. These dynamic tensions add a layer to the experience of cumulative impacts that have yet to be characterized qualitatively in this community.
Considering the complex nature of cumulative impacts as demonstrated above, participants identified several potential solutions that deeply aligned with and built upon key community strengths that may aid in our ability to fully understand a community’s experience of cumulative impacts. These findings reflect the existing quantitative literature examining how cumulative impacts interact with health,2 but our work applies an innovative lens by exploring the qualitative, lived experiences of people living with cumulative impacts.
This study has several limitations, including lack of generalizability to the broader population of Southern Delaware County. Our pool of potential participants may have been limited due to our requirement to have previously participated in the environmental health survey. Participants were predominantly female and resided in only a quarter (3/12) of eligible municipalities. Thus, our findings may not fully reflect the experiences of people living in other communities in the study area. It is also possible that participants in the focus groups represent the most outspoken residents and not necessarily the most impacted residents. We were also unable to assess saturation (as is typical in qualitative studies) and instead were resource-limited by the number of participants who were eligible and interested in participating in the focus groups. We conducted focus groups until all eligible and interested participants could do so. While qualitative methods are well-suited for delving into the lived experiences and diverse perspectives of participants, these methods do not allow for the quantification or generalization necessary to assess prevalence and establish causal relationships.
The study also has many strengths, notably our use of the CBPR approach, which resulted in better cooperation and collaboration throughout the scientific process, including data collection and analysis. We believe having an impacted community resident and community investigator facilitate the focus groups cultivated a greater trust among participants, which may have inspired a more candid responses than if an academic investigator had facilitated. Community investigators provided critical insights and context that were instrumental in interpreting the data and generating key themes throughout the analysis.
Empowering community residents with the data and disseminating findings to the broader community and key stakeholders is a critical element of our approach. Key findings from these focus groups were integrated with the findings of the community environmental health survey into a technical report that was shared with stakeholders (e.g., elected officials, community advocates, and residents) at a public community meeting hosted by the community investigators before the submission of this article. At this hybrid meeting, the study team presented study findings to approximately 90 attendees (over 60 in person and 30 on Zoom). The study team presented the findings and sparked a discussion between community residents and local community and political representatives that quickly turned to next steps for community organizing and advocacy. The next steps will include an advocacy campaign to explore legislative policies aimed at mitigating and preventing the impacts of chemical and non-chemical stressors. While every community faces a unique combination of chemical and non-chemical stressors, this work contributes to the broader body of literature demonstrating the feasibility of community-based science and the range of cumulative impacts faced by communities. In addition to state and local policy advocacy and change, a better understanding of community-level cumulative impacts may offer opportunities to advance cumulative risk assessment methods to inform national policies. Studies of cumulative impacts may gather data on relevant combinations of stressors and may quantify combined stressor-health effect relationships. This challenges the U.S. EPA and many states’ current siloed approach to media-specific (e.g., water, air, soil) programs and regulations.
CONCLUSION
We used a CBPR approach to learn more about how residents in a fenceline community experience the cumulative burdens of chemical and non-chemical stressors. This work demonstrates how qualitative methods, when employed alongside a CPBR approach, can improve our understanding of cumulative burdens and generate data and solutions to support advocacy efforts to prevent the exacerbation of harm in already overburdened communities.
Footnotes
ACKNOWLEDGMENT
The authors thank the participants who shared their time and stories.
AUTHORS’ CONTRIBUTIONS
A.L.: Conceptualization, data curation, formal analysis, visualization, writing—original draft. A.A.C.: Conceptualization, data curation, funding acquisition, formal analysis, visualization, investigation, methodology, writing—review and editing. L.S.: Conceptualization, funding acquisition, investigation, methodology, writing—review and editing. K.N.W.: Conceptualization, funding acquisition, investigation, methodology. E.S.M.: Conceptualization, funding acquisition, investigation, methodology. T.N.: Conceptualization, funding acquisition, methodology. E.A.: Conceptualization, funding acquisition, methodology. P.F.D.: Conceptualization, funding acquisition. M.A.F.: Conceptualization, methodology, writing—review and editing. R.D.K.: Conceptualization, investigation, methodology, writing—review and editing. K.E.N.: Conceptualization, funding acquisition, supervision, writing—review and editing. S.N.L.: Conceptualization, funding acquisition, investigation, methodology, project administration, supervision, visualization, writing—review and editing.
ETHICAL CONSIDERATIONS
All human subject research study tools and protocols were reviewed and approved by the Johns Hopkins Institutional Review Board (IRB00024902).
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
This project was supported by pilot funding from the Johns Hopkins University Community Health Addressing Regional Maryland Environmental Determinants of Disease (CHARMED) P30 Center NIEHS P30ES032756. P.F.D., K.E.N., S.N.L., and A.A.C. received financial support from the Bloomberg Philanthropies (Grant ID 2021-100480). A.A.C. was supported by NIEHS Training Grant T32ES007141 and the 21st Century Cities Initiative at Johns Hopkins University.
1
2
3
Payne-Sturges, Devon C., Tanya Khemet Taiwo, Kristie Ellickson, Haley Mullen, Nedelina Tchangalova, Laura Anderko, Aimin Chen, and Maureen Swanson. “Disparities in toxic chemical exposures and associated neurodevelopmental outcomes: a scoping review and systematic evidence map of the epidemiological literature.” Environmental Health Perspectives 131, no. 9 (2023): 096001.
5
6
Williams, Paige, Anita Zuberi, Debra Hyatt-Burkhart, and Jennifer Padden Elliott. 2023. “‘People Should Not Have to Live Under These Conditions’: Using Focus Groups to Inform the Development of a Community-Led Intervention Addressing Air Quality and Health Equity.” https://home.liebertpub.com/env, November. ![]() .
.
7
8
9
Wang, Suwei, Molly B. Richardson, Mary B. Evans, Ethel Johnson, Sheryl Threadgill-Matthews, Sheila Tyson, Katherine L. White, and Julia M. Gohlke. 2021. “A Community-Engaged Approach to Understanding Environmental Health Concerns and Solutions in Urban and Rural Communities.” BMC Public Health 21 (1). ![]() .
.
10
11
Alford, Echo & Chiger, Andrea & DeCarlo, Peter & Fox, Mary & Kennedy, Ryan & Lightner, Alexis & Lupolt, Sara & Nachman, Keeve & Miari, Eve & Snyder, Lora & Nixon, Thom & Warren, Kearni. (2024). Assessing Strengths, Stressors and Environmental justice in SoutheaStern (ASSESS) Pennsylvania Communities: Environmental Health Study Summary Report. 10.13140/RG.2.2.36504.61443.
12
13
14
15
15 Tehrani, Mina W., Fortner Edward C., Robinson Ellis S. Chiger Andrea A., Sheu Roger, Werden Benjamin S., Gigot Carolyn, Yacovitch Tara, Bramer Scott Van, Burke Thomas, Koehler Kirsten, Nachman Keeve E., Rule Ana M., DeCarlo Peter F. 2023. “Characterizing metals in particulate pollution in communities at the fenceline of heavy industry: combining mobile monitoring and size-resolved filter measurements.” Environmental Science Process Impacts. Accessed November 2024. ![]() .
.
16
17
19
Balazs, Carolina L., and Rachel Morello-Frosch. “The three Rs: How community-based participatory research strengthens the rigor, relevance, and reach of science.” Environmental justice 6, no. 1 (2013): 9–16.
20
Israel, Barbara A., Amy J. Schulz, Edith A. Parker, and Adam B. Becker. “Review of community-based research: assessing partnership approaches to improve public health.” Annual review of public health 19, no. 1 (1998): 173–202.
22
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.