
Abstract
Background:
The health impacts of extreme heat and wildfire smoke events are unevenly distributed; climate-sensitive populations are more exposed, more sensitive, and less likely to have the resources to respond. In this article, we describe the process of building a community-academic-local government partnership and conducting a climate survey with climate-sensitive populations to inform city-wide climate adaptation planning efforts in San Francisco, California.
Materials and Methods:
We formed a Community Stakeholder Group (CSG) with seven representatives from community organizations serving residents disproportionately affected by extreme climate weather events. The CSG identified priority populations, developed conceptual models, and developed and disseminated a climate survey.
Results:
CSG member engagement and satisfaction were high; 100% agreed that their opinions were valued and that they could talk openly. 95% and 98% of climate survey respondents (n = 529) experienced at least one negative health outcome during extreme heat and wildfire smoke events, respectively. While 50%–75% of survey respondents implemented simple protective actions, the majority were unable to make substantial material and structural changes to their living environment that could significantly reduce their exposure to extreme heat and poor air quality. Major barriers included the high cost of repairs/materials, being a renter, and being unstably housed or unhoused.
Conclusion:
Our project is unique in the multi-stakeholder partnership formed between local government, community, and academic partners. A major learning from our engagement process is that climate adaptation interventions designed for climate-sensitive populations should incorporate structural changes to living environments and be codesigned with the community, with careful consideration to avoid maladaptive interventions that deepen existing injustices.
INTRODUCTION
Climate change is increasing the frequency, intensity, and duration of extreme heat and wildfire smoke events, both of which have serious adverse health effects. Heat waves are one of the largest weather-related causes of preventable death in the U.S. 1 Wildfire smoke has a significant impact on air quality and is hazardous to human health 2 , particularly in California, where 8 out of the 10 largest wildfires in the state’s history burned between 2017 and 2022. 3 Furthermore, co-exposure to extreme heat and air pollution due to wildfire smoke may have compounding health effects on respiratory and cardiovascular morbidity and all-cause mortality. 4
The health impacts of these extreme weather events are not evenly distributed. 5 Risk factors for susceptibility to these climate-related events have been categorized as intrinsic (e.g., having preexisting medical conditions, age, disability) or extrinsic (e.g., living in low-income housing that does not remain cool, disproportionate chronic exposure to social and environmental hazards). 6 Lower-income and minoritized communities are disproportionately impacted by both risk factors. 7 Older adults, women and young children, people with mobility challenges or disabilities, and persons experiencing homelessness are more vulnerable to adverse health outcomes from these extreme weather events, as they are often the most sensitive, most exposed, or least likely to have the resources to prepare and respond. 8
Over the past 2 decades, many U.S. cities have taken action to reduce the risks of climate change by developing and implementing climate mitigation and adaptation plans. 9 These plans vary in the attention placed on justice (defined as prioritizing communities disproportionately affected by climate change) and equity (defined as equitable distribution of benefits and burdens of climate policies). 10 While a review of climate action plans found that many are increasingly incorporating justice into their plans, 11 there is a lack of research on how disproportionately impacted communities are involved in planning efforts. 12 The involvement of these communities is critical to ensure that strategies selected correspond with the causes of vulnerability and to avoid maladaptation, which creates conditions that may worsen the situation. 13
There is increasing interest in incorporating Community-Based Participatory Action Research (CBPAR) approaches to identify climate adaptation strategies that lead to structural changes that protect the well-being of climate-sensitive populations. 14 The core principles of CBPAR involve developing collaborative, equitable partnerships between researchers and communities in all phases of research and shared decision-making power. 15 While both environmental justice principles and CBPAR approaches place community agency and democratic processes at the center of their theories of change, 16 there are few examples in practice of forming and sustaining community-academic-local government partnerships that further climate justice and lead to actionable change.
Study objectives
In this article, we describe the process of building a partnership between City of San Francisco municipality stakeholders involved in the Health and Air Quality Resilience (HAQR) Project, community-based organizations (CBOs), and academic researchers from the University of California, San Francisco (UCSF) to bring climate-sensitive community priorities into city-wide climate adaptation planning efforts. Our study involved forming and working with a Community Stakeholder Group (CSG) to codevelop and implement a cross-sectional climate survey to better understand resident’s perspectives on the health impacts of extreme heat and wildfire smoke events, acceptable community-level adaptation actions, and barriers and facilitators to implementing these actions.
Setting
This work is based in San Francisco, the most densely populated large city in California. 17 San Francisco is home to approximately 808,437 residents, of whom 37% are Asian, 16% are Latinx, 6% are Black/African American, 5% are multi-ethnic/multi-racial, and less than 1% are Pacific Islander or Native American. 18 Forty-three percent of the population speak a language other than English in the home. 19 The health impacts of climate change are not equally distributed across San Francisco. When considering several factors, including exposure, sensitivity, and adaptive capacity, the San Francisco Department of Public Health (SFDPH) identified neighborhoods in San Francisco as being most vulnerable to extreme heat (Fig. 1).
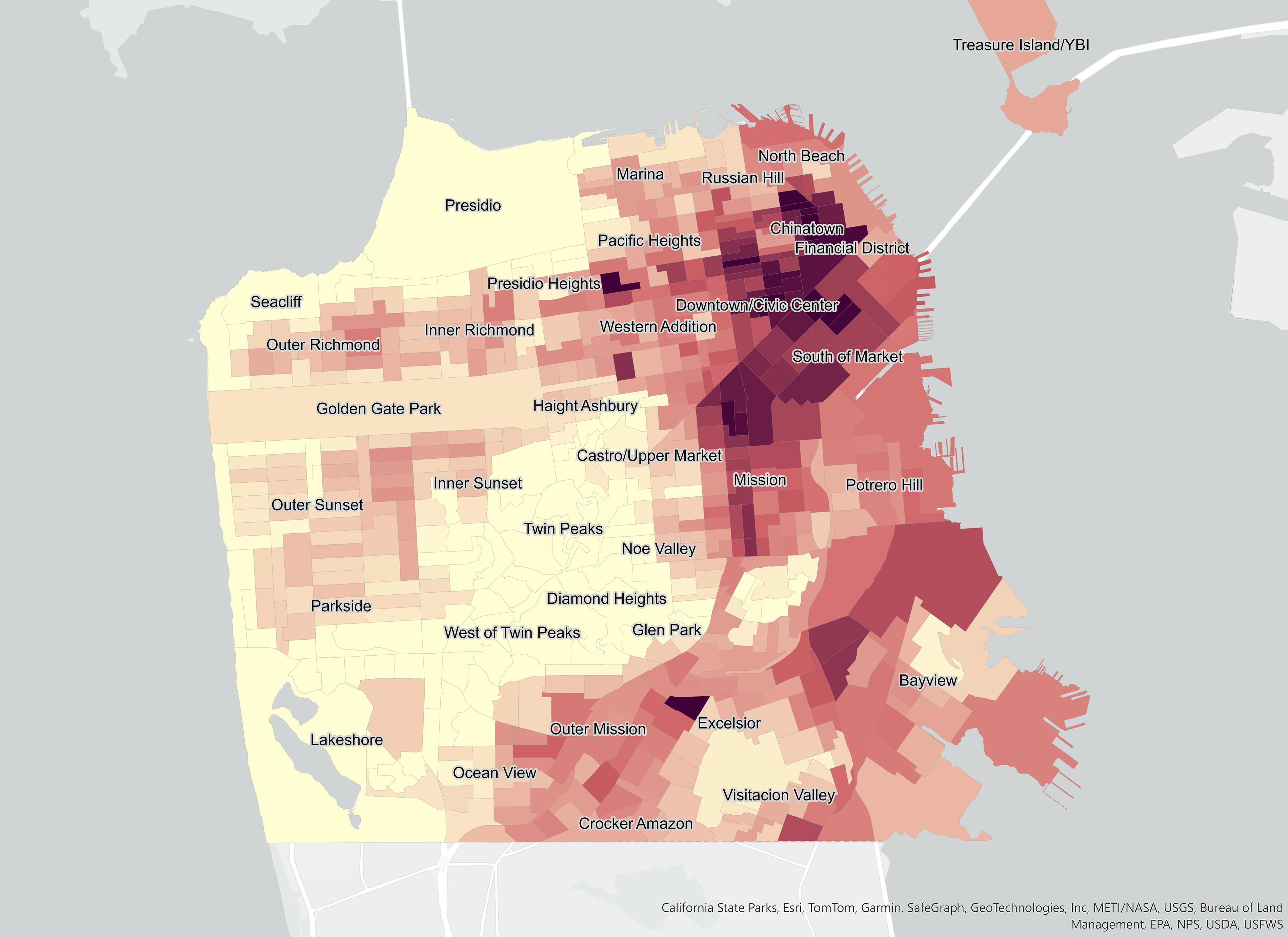
Extreme heat vulnerability of San Francisco, by census tract. Labels on the map indicate San Francisco neighborhoods. Darker colors indicate higher vulnerability to extreme heat events, lighter colors indicate lesser vulnerability.
Health and air quality resilience project
Our CBPAR project collaborated closely with San Francisco’s HAQR project. HAQR, a cross-sectoral initiative led by SFDPH and the San Francisco Office of Resilience and Capital Planning, brings together municipal departments involved in emergency preparedness and response services, housing, and infrastructure, in addition to private, academic, and local community partners to identify and implement medium-to-long-term extreme heat and wildfire smoke adaptation strategies. 20 In the early phases of developing the HAQR Implementation Plan, HAQR was approached by community members and organizations supporting climate-sensitive populations that the process for engagement was superficial and that there was a need to further understand health impacts and resource gaps to prepare, respond, and recover from extreme heat and wildfire smoke events. The HAQR leadership team contacted UCSF and asked for support to conduct formative partnered research to ensure that community priorities were reflected in city-wide climate adaptation planning efforts.
MATERIALS AND METHODS
Study activities took place between February 2022 and August 2023. The project received institutional review board approval from UCSF.
Engagement approach
Our engagement approach acknowledged that historic and present-day decisions by the government on environmental issues have disproportionately impacted low-income and Brown and Black communities. In addition, traditional research models have a history of being extractive and often leave the community as a passive player in the process. Our engagement approach was based on CBPAR principles and shared decision-making with the CSG throughout the research project. The research topic area and method of data collection (survey-based) were informed by broad community concerns that the process to develop the HAQR Implementation Plan did not prioritize input from climate-sensitive communities. The design of the survey instrument, study design (cross-sectional vs. longitudinal), recruitment plan, data analysis, ground-truthing of findings, and dissemination of results were conducted in partnership with the CSG. By creating spaces for learning with and from the community and using multiple communication channels to ensure consistent and open communication, our engagement approach focused on building trust and mutual accountability with community stakeholders.
A key aspect of our engagement approach included hiring (via a competitive contracting process) a community liaison consultant to recruit community partners to the CSG, co-plan agendas/materials, and facilitate CSG meetings to ensure all voices were heard; hold one-on-one check-in sessions with CSG members; and serve as a neutral partner between CBO, local government, and academic partners. We engaged GM Consulting Group, LLC, a Latina-owned community engagement firm with a decade of experience facilitating multi-stakeholder groups across the Bay Area.
Lastly, many of the CBOs we approached to participate in the CSG were responding to multiple local priorities and operating with limited resources. To ensure flexibility for engagement, we split the engagement process into phases and compensated members according to their degree of engagement, which enabled CBOs to participate based on their current capacity and reengage at different time points. This flexibility was valuable as it allowed for long-term relationship building and maximized the diversity of perspectives along the project continuum.
Forming the community stakeholder group
The initial CBPAR planning group—comprised of the UCSF principal investigator, a UCSF staff member, two representatives of the HAQR coordinating committee, and a community liaison consultant—used the San Francisco Heat Vulnerability Index 21 (the Index contains data on 21 variables, including preexisting health conditions, demographic and socioeconomic factors, environmental exposure factors, and infrastructure conditions) to identify neighborhoods most vulnerable to adverse health effects from extreme heat. We also identified other climate-sensitive populations not defined by geography that are disproportionately affected by extreme weather events (Table 1).
Community Stakeholder Group (CSG) Members, Populations Served & Project Participation
Phase 1: Define priority populations, develop conceptual models, develop climate survey questionnaire.
Phase 2: Climate survey participant recruitment and dissemination.
We used this list of climate-sensitive populations to identify CBOs working closely with these populations across San Francisco. Our team held 15 “coffee break” meetings with identified CBO representatives to better understand their service priorities and to gauge their interest in participating in the CSG focused on two main goals: (1) identify community health concerns related to wildfire smoke and extreme heat events and (2) identify community input on preferred adaptation strategies. Coffee break meetings were held at a convenient time and location for CBO representatives and provided concise, easy-to-understand descriptions of the proposed work, as well as protected time for questions and dialogue. Coffee break meetings provided valuable space for CBOs to provide feedback on how their priorities aligned with the research topic area and to gather input on the CSG leading many aspects of the research, including what survey questions to ask, who to survey, the recruitment process, and to whom and how to disseminate results.
The coffee break meetings led to the identification of seven representatives from CBOs serving climate-sensitive groups and neighborhoods in San Francisco to participate in the CSG (Table 1). While most CBOs approached expressed interest in the project, those unable to commit mentioned limited bandwidth as the primary reason for not participating. The CBOs serving on the CSG were from most of the climate-sensitive populations in San Francisco (see Table 1 for climate-sensitive populations served by the CSG), except for a CBO explicitly serving pregnant women and young children. We divided the project into two phases to provide flexibility in participation based on member bandwidth.
Priority populations, conceptual models, and climate survey development with the CSG
During Phase 1, we held four CSG meetings (Table 2). Following CSG preferences, all meetings were held online via videoconferencing for flexibility and convenience. To ensure CSG members’ perspectives were authentically represented and incorporated into CSG meetings, we conducted brief online engagement surveys following each Phase 1 CSG meeting.
Phase 1 Community Stakeholder Group (CSG) Meeting Dates and Topics Discussed
The CSG used the Stakeholder Engagement in Question Development and Prioritization (SEED) method to further refine priority populations, develop conceptual models to understand how health risks occur, and develop the community climate survey. The SEED method is based on participatory action research principles nested within the socio-ecological model and provides a systematic iterative approach to engage community stakeholders in developing health-related research plans. 22
After refining priority populations, the CSG developed conceptual models for each priority population to visualize the potential health impacts experienced by residents during extreme heat and wildfire smoke events, resources available to mitigate negative health impacts, and barriers faced in utilizing resources. The conceptual models were used to develop an initial draft of the survey, which underwent several revisions with the CSG and was piloted with community members and further refined.
The survey included questions on demographics; health symptoms experienced during extreme heat and wildfire smoke events; preventative actions to prepare for these events; actions taken during previous extreme heat/wildfire smoke events, including barriers and challenges faced; and extreme weather alerts received (see Supplementary Appendix A1 for the final survey).
The survey was translated by a translation service into Spanish and traditional Chinese and edited by bilingual community members to ensure accuracy and cultural appropriateness. The final version of the survey was programmed into Qualtrics XM, an online survey platform. All survey participants received demographic questions. To reduce survey burden, participants were randomized to receive either questions on extreme heat or wildfire smoke.
Between January and July 2023, during Phase 2 of the project, the survey was distributed by participating CBOs via convenience sampling, each leveraging their social/organizational networks to reach their priority populations. Survey participants were provided a $10 gift card after completing the survey.
Survey data analysis
Descriptive statistics of sociodemographic characteristics, health outcomes/concerns, and protective behaviors were calculated. Bivariate tabulations were performed between characteristics, behaviors, and health outcomes/concerns to identify potential relationships across variables of interest. These results were shared and co-interpreted with CSG members.
To facilitate comparison of the survey participant to the CSG priority neighborhoods, sociodemographic data were procured from the U.S. Census Bureau’s American Community Survey (ACS) for years 2017–2021 at the block group level. Graphic information system (GIS) polygons for San Francisco-specific neighborhoods were sourced from the Office of Housing and Planning Department; ACS data were aggregated to these neighborhood polygons using coverage fractions.
Directed acyclic graphs (DAGs) were devised from CSG conceptual models, where survey variables were mapped to the closest abstraction captured in conceptual models (see Supplementary Appendix A2). DAGs are drawn using a structured framework to identify confounders requiring adjustment in exposure-outcome relationships. 23 We fit generalized linear models with binomial and Poisson distribution based on these DAGs to investigate the associations between health outcomes and sociodemographic factors or health behaviors while adjusting for potential confounding. Parametric bootstrapping was utilized to estimate measures of association and 95% confidence intervals (CIs). For variables measured on a Likert scale, both categorical and continuous variants were considered as sensitivity analyses. Survey data were analyzed using R 4.2.3.
RESULTS
Findings from CSG meeting engagement surveys
100% (7 out of 7) of CSG members completed brief online engagement surveys following Phase 1 CSG meetings. 100% agreed/strongly agreed that they could talk openly at CSG meetings and that their opinions were valued by other members. 100% were satisfied/very satisfied with meeting facilitation, online location and length of meetings, and compensation for participation.
Priority populations
Five priority populations were identified by the CSG as most susceptible to the negative health effects of extreme heat and wildfire smoke events (Table 3). Our CSG members provided invaluable insights on populations vulnerable to extreme weather events in San Francisco. They advocated for the inclusion of youth as a priority population, particularly transitional-aged foster youth, a group that faces many challenges in accessing resources and support.
Priority Populations Identified by the CSG
CSG, community stakeholder group.
Conceptual models
The CSG developed conceptual models to visualize the health impacts experienced by residents from priority groups during extreme weather events. The models include health impacts experienced, resources available to mitigate negative health impacts, and barriers to utilizing the resources available. As an example, we have shared the conceptual model developed for adults 65 years of age and older during extreme heat events (Fig. 2).
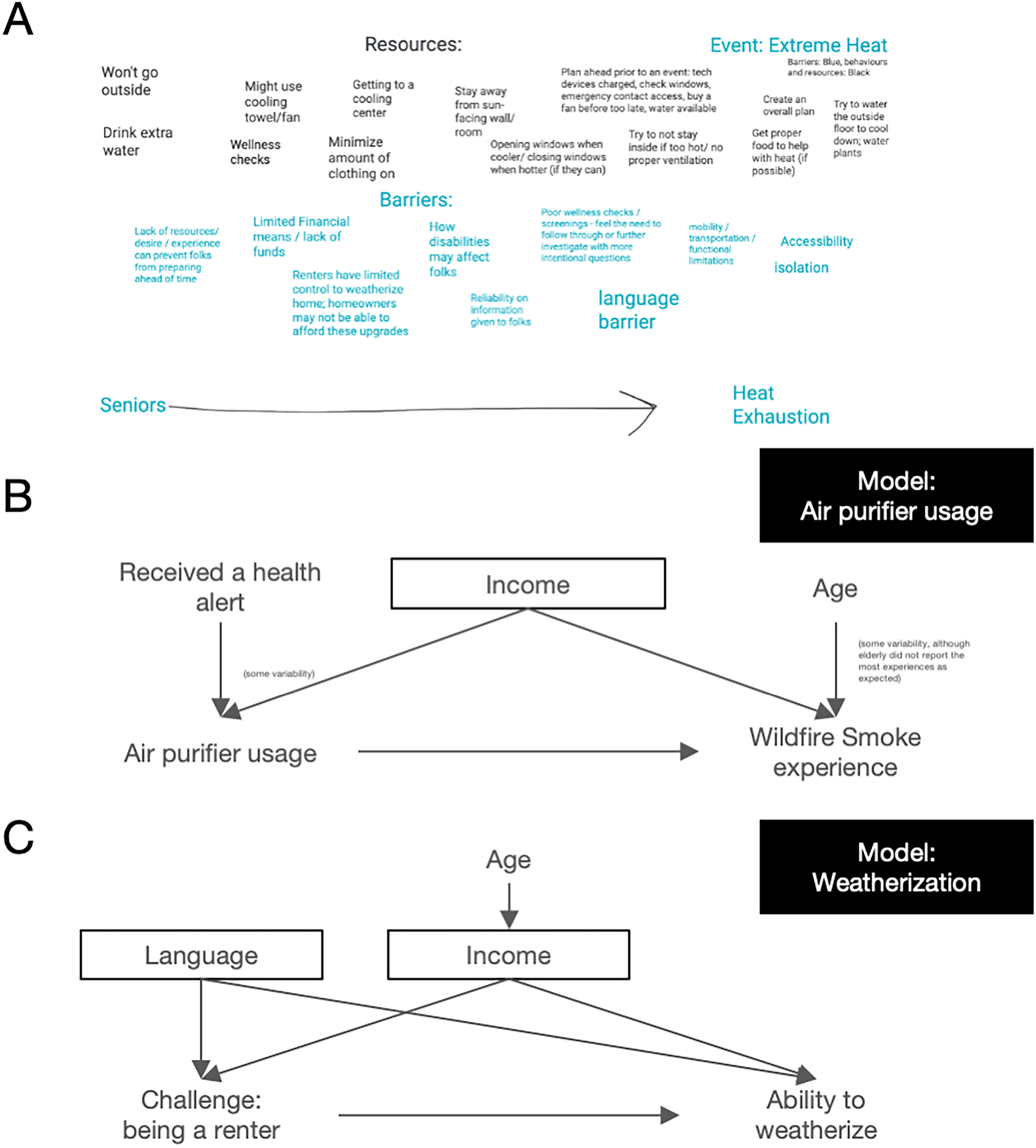
Conceptual models and directed acyclic graphs (DAGs).
Climate survey demographics
Survey completion was high, with 96.7% (n = 529) of participants providing responses to survey questions. About half of respondents were affiliated with NICOS Chinese Health Coalition, a coalition of organizations supporting the health of Chinese Americans in San Francisco with limited English fluency. Leaders4EARTH, an environmental justice organization composed of youth and young adults, contributed about a quarter to the total sample size. Respondents affiliated with the Coalition on Homelessness made up 18% of the sample, and those affiliated with Rafiki comprised 7%. These latter organizations focus on the health of unhoused single adults and older adults with disabilities and/or chronic mobility issues, respectively (Table 4).
Climate Survey Respondent Demographics
A majority (57.3%) of the sample was female-identifying, with a median age of 36. Forty-three percent identified as Asian, 23% Hispanic/Latino, 19% Black, and 4% White, non-Hispanic. Fifty-four percent indicated English was not their primary language spoken at home; 35% and 14% spoke Chinese and Spanish at home, respectively.
Twenty-seven percent of respondents resided in a condo or apartment, 24% in a single-family home, 23% in a rented/shared room, 10% were experiencing homelessness, 9% lived in a single-room occupancy hotel, and 6% were living in a Section 8 apartment or public housing. The median number of people per bedroom was 1.5, indicating some residential crowding. Eighteen percent of respondents reported an annual income of less than $5,000, 30% made between $5,000 and $25,000, 29% indicated making between $25,000 and $50,000, and 7% reported making $50,000 or greater.
Compared with neighborhood-level demographics derived from ACS data, our survey population captured a higher representation of lower-income, racial/ethnic minorities with lower rates of secondary education attainment. Geographically, a large proportion of survey respondents resided in or near CSG priority neighborhoods, such as Downtown/Civic Center, Chinatown, SOMA, Bayview, and Visitacion Valley (Fig. 3).
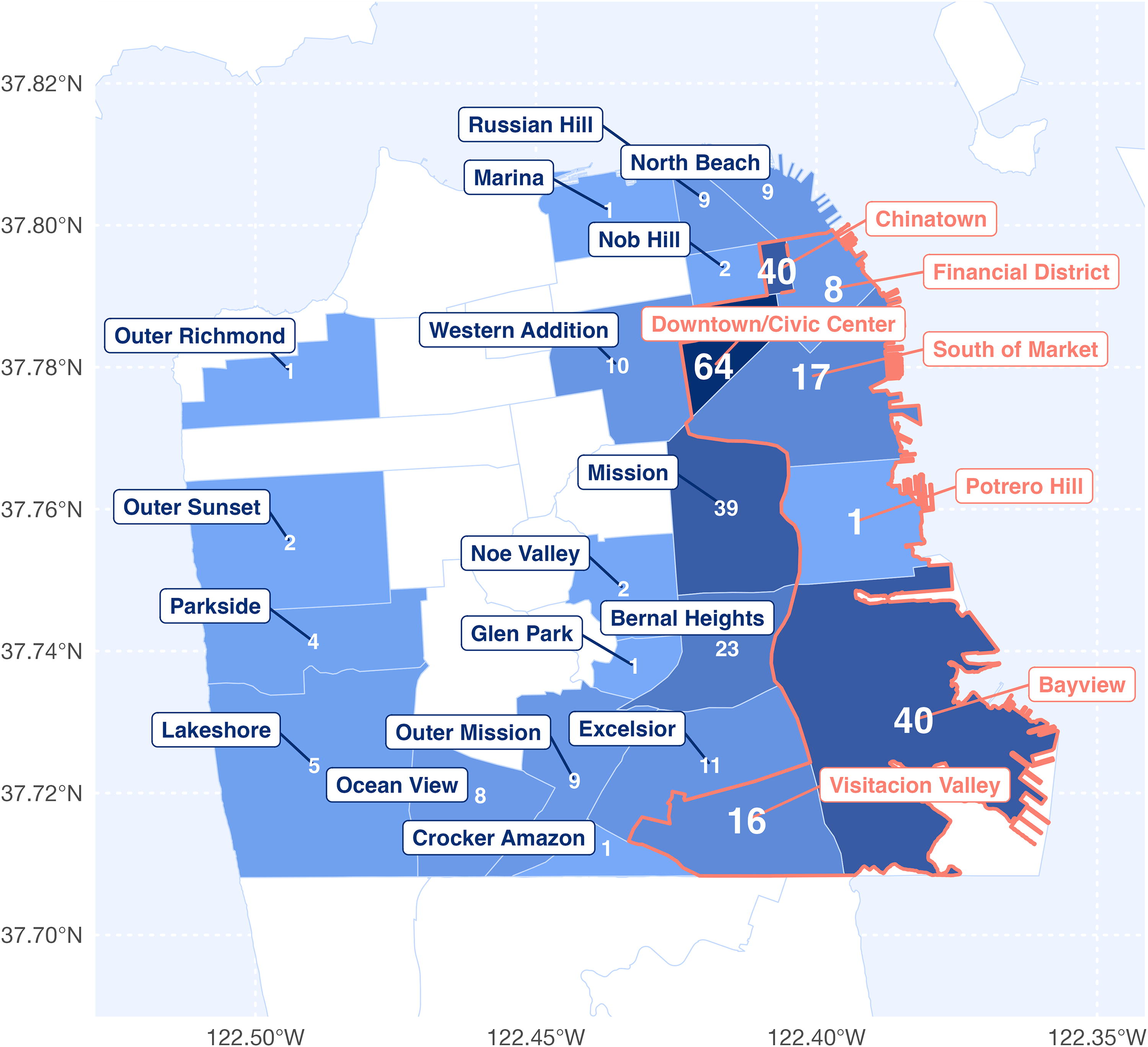
Geographic distribution of climate survey respondents. Annotated numbers on map indicate the summed number of completed surveys with provided addresses.
Climate survey health outcomes
95% and 98% of respondents indicated experiencing at least one health outcome (i.e., breathing problems, fatigue, exhaustion, chest pain) because of extreme heat and wildfire smoke events, respectively. Fatigue, dehydration, and heat exhaustion were the most common outcomes due to extreme heat, while fatigue, headaches, and breathing problems were most common due to wildfire smoke (Fig. 4a, 4b).
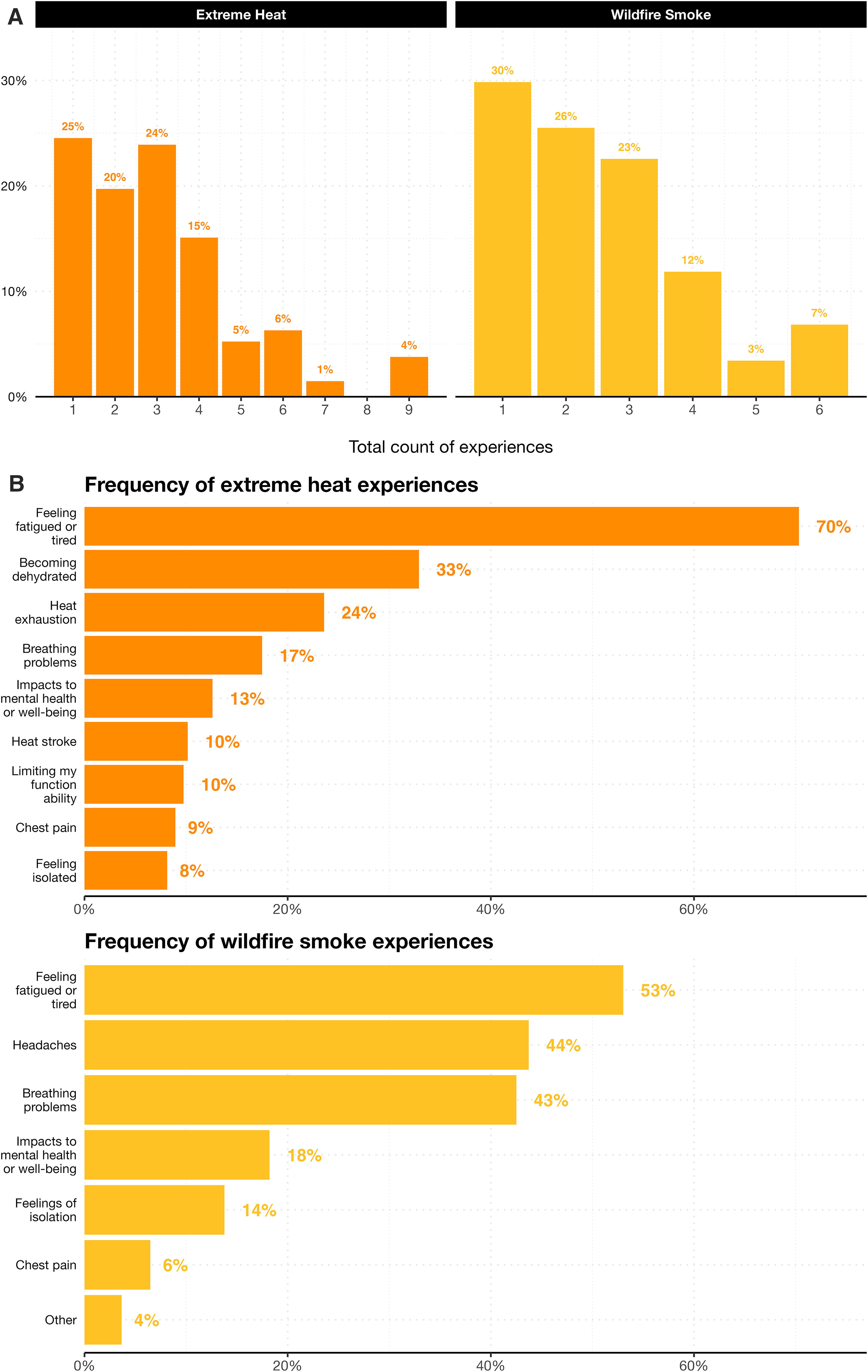
Health impacts experienced during wildfire smoke and extreme heat events.
Climate survey protective health behaviors
Respondents engaged in a variety of personal, infrastructural, and material protective behaviors to decrease their exposure to extreme heat and wildfire smoke. However, they also faced structural and economic challenges while attempting to implement protective behaviors or access resources.
To alleviate the immediate effects of extreme heat, respondents drank water (76%), wore lightweight clothing (75%), closed blinds/curtains (67%), used fans (61%), and avoided outdoor activity (54%). For wildfire smoke, respondents closed windows (58%), avoided going outdoors (53%), and 53% wore face respirators/masks (44% of these wore N95/KN95s). However, cited challenges included the cost of fans (26% and 28% for extreme heat and wildfire smoke events, respectively) and having an outdoor job (18% and 15%) as major barriers to engaging in these behaviors. While 56% and 65% of respondents used air conditioning or air filtration devices if they owned such a device during extreme heat and wildfire smoke events, respectively, ownership was low overall (23% for air conditioning, 27% for air filtration devices). Ownership was disproportionately lower for those who were unstably housed, did not consider English their primary language, or were older.
For supplies preparation, 58% of respondents had a two-gallon supply of water set aside for extreme weather events, 54% had a high-quality mask for wildfire smoke, and 48% had a 2-week supply of food and medication. Respondents cited unstable housing/experiencing homelessness and the cost of supplies as major challenges in adequate preparation.
While a small proportion of respondents indicated they weatherized their residence in preparation for extreme heat (20%) and wildfire smoke events (17%), a larger proportion planned to repair or weatherize their residence (28% and 37%, respectively). Costs, being a renter, or being unstably housed/unhoused were the most reported challenges to weatherization.
Climate survey model results
Priority research questions were defined and ranked by the CSG. DAGs were devised for these research questions and informed by the conceptual models developed during collaborative sessions with CSG members. DAGs informed statistical models fitted to gain inference into highly prioritized questions among community stakeholders (Tables 5, 6, 7 and 8).
Descriptive Statistics for Model 1
Descriptive Statistics for Model 2
Descriptive Statistics for Model 3
Statistical Model Concepts, Specifications, Estimates, and Confidence Intervals (CI)
Indicates statistical significance at p < 0.05, 95% confidence intervals do not cross the null value.
Factors associated with receiving a wellness check
Increasing age was positively associated with the odds of receiving wellness checks (a preventative health visit from a local organization to susceptible individuals) during prior extreme heat events when adjusting for comorbidities (defined as actively using a durable medical device). One additional year of age was associated with 1.07 times greater odds of receiving a wellness check (95%CI: 1.02, 1.11). No associations were observed when examining for factors associated with receiving a wellness check during prior wildfire smoke events.
Being a renter and engaging in weatherization
Reporting facing challenges as a renter was strongly associated with decreased odds (estimate: 0.09; 95%CI: 0.01, 0.87) of engaging in weatherization for wildfire smoke compared with those who did not report facing challenges as a renter, after adjusting for English fluency and income. We did not observe a similar association for engaging in weatherization to prepare for extreme heat events.
Distance and accessing respite centers during extreme heat and wildfire smoke events
Among survey participants who provided addresses, increasing distance to the nearest public respite center was negatively associated with using said respite center; a 1 kilometer (km) increase in distance to a center was associated with decreased odds of using the center “Most/All of the time” compared to “Rarely/Never” by a factor of 0.88 (95%CI: 0.77, 0.99) and 0.89 (95%CI: 0.79, 0.97) for wildfire smoke and extreme heat events, respectively, after adjusting for access to transportation.
DISCUSSION
Research on the process of forming and maintaining empowered community-academic partnerships working toward environmental and climate justice has found that trust, bidirectional learning, and open communication are essential to ensure that community partners impacted by environmental decisions have community agency to speak for themselves and participate as equal partners in the research. 24 Our study adds to this literature by sharing our process of utilizing CBPAR approaches to form a community-academic-local government partnership and our formative research to codevelop and disseminate a climate survey among multiple climate-sensitive populations, which is unique as most research to date focuses on one specific climate-sensitive population, such as adults aged 65 and older.
Findings from our CSG meeting engagement surveys show that CSG members were highly satisfied with group dynamics, meeting logistics, and compensation for their participation. Furthermore, 100% agreed or strongly agreed that they could talk openly and honestly at CSG meetings and that their opinions were respected and valued. These findings suggest that our engagement approach facilitated trust building and enabled a productive group environment essential for the coproduction of high-quality research. We have worked closely with the CSG to ensure broad dissemination of results, including publishing a community report that was shared with the CSG and HAQR, several report-back “town hall” meetings, and developing and disseminating visual handouts tailored to climate-sensitive priority populations and the community at large.
Our climate survey found that climate-sensitive priority populations on average experience between 1–2 negative health outcomes during extreme heat and wildfire smoke events. While 50%–75% of survey respondents implemented simple individual or household protective actions, the majority were unable to make substantial material and structural changes to their living environment that could significantly reduce their exposure to extreme weather events, especially among older adults, persons unstably housed, and households for whom English was not their primary language. Major challenges to implementing higher-impact structural measures include the high cost of repairs/materials, being a renter, and being unstably housed or unhoused.
Most studies identified in our literature review of climate adaptation research conducted in partnership with climate-sensitive populations focused on medically vulnerable adults or older adults, populations that have experienced the highest mortality rates following heat waves. 25 Studies have found that many unique physiological, socioeconomic, psychological, and contextual factors should be considered when designing interventions for older adults. 26 Furthermore, research has found that older adults who are socially isolated, living alone and/or on low incomes, face more barriers in taking protective actions during extreme heat events. 27 A study among medically vulnerable adults during prescribed wildfire burns found that participants were able to implement lower-cost protective actions, but even with advanced notice of the planned burn, few were able to implement more effective costly interventions, such as the use of air purifiers. 28 This is consistent with our study findings that higher-cost material and structural interventions are challenging for medically vulnerable and older populations to implement, especially those living on low incomes.
The next step with our community-academic-local government partnership is to use the survey results to coidentify and test promising strategies to increase the uptake of adaptive strategies among climate-sensitive populations. A recent study conducted in the San Francisco Bay Area piloted two climate adaptation interventions—a smartphone app delivering extreme weather alerts and education and portable air cleaners to improve indoor air quality—chosen in partnership with low-income, frontline communities. 29 They initially considered implementing a weatherization program, but this component was abandoned due to community concerns about housing displacement. 30 In-depth interviews found that participants faced challenges in navigating the app and that some participants did not use the portable air cleaners 31 , highlighting the need for more formative research and iterative conversations with end users to effectively adapt interventions to their context.
Study strengths
Our study is unique in that we did not see examples in the literature of community-academic-local government partnerships conducting formative, participatory research focused on gathering input from climate-sensitive populations on their health concerns related to wildfire smoke and extreme heat events and their preferred climate adaptation strategies. It is also unique in that multiple, diverse local government and community partners participated as key partners in this research. A survey of early adopters of citywide climate adaptation planning efforts found that often only two city departments are involved—departments of environment and land-use planning—while health departments are rarely engaged. 32 The HAQR project, a key partner in this work, is co-led by the health department and includes representatives from numerous city departments. Other key features that contributed to the success of this project include the engagement of a community liaison consultant and securing 2 years of project funding, which provided more time to form the partnership and funds to compensate community members for their contributions.
Limitations and challenges
Our cross-sectional climate survey with convenience sampling provides a one-time snapshot of the health effects experienced among climate-sensitive subpopulations and barriers and facilitators to implementing protective actions. This research design is subject to numerous biases that may affect internal study validity and generalizability of findings to other communities. A limitation of our convenience sample is that persons with disability/mobility issues were not well represented as they were harder to recruit, while limited English-speaking populations were overrepresented due to strong recruitment networks. Prospective longitudinal studies with more robust quasi-experimental designs could help to better understand adaptive capacity among climate-sensitive subpopulations over time and identify and control for potential confounders. In addition, our climate survey was predominantly quantitative, providing useful data on health impacts experienced, protective actions taken, and barriers and challenges faced among climate-sensitive priority populations, but it offers limited understanding of why or how this is the case. Future studies employing qualitative or mixed methods will be helpful to explore these issues in more detail.
CONCLUSION
Our primary study finding that climate-sensitive residents from all priority populations predominantly implement low-cost, simple individual and household protective actions but face challenges in implementing higher-impact material and structural interventions highlights the need to carefully consider how to address underlying social vulnerability within urban climate adaptation planning efforts. Given the social vulnerabilities and climate injustices already faced by climate-sensitive populations, careful consideration should be given to avoid implementing maladaptive interventions that deepen existing injustices.
We believe that community-academic-local government partnerships employing CBPAR methodologies that authentically involve community members as equal partners hold great promise to identify innovative climate adaptation strategies that promote climate justice and prevent maladaptive responses. The involvement of local government provides a unique opportunity to access governmental resources, promote policy actions, and secure longer-term funding to implement structural climate adaptation strategies over time. Finally, given the increased severity and frequency in which extreme weather events are occurring and the risk for co-occurring climate events (i.e., co-occurring extreme heat and wildfire smoke events), communities may benefit from prioritizing multiple-event strategies that incorporate structural changes to living environments for the highest impact and the best use of finite resources.
Footnotes
ACKNOWLEDGMENTS
The authors thank the full Community Stakeholder Group, the Health and Air Quality Resilience Project, and all climate survey participants. In addition, the authors thank our community liaison consultant, Giuliana Martinez, for her expert facilitation during Community Stakeholder Group meetings and her contributions to this research project.
AUTHORS’ CONTRIBUTIONS
L.D.M. conducted research administration and wrote the article. A.N. analyzed data, drafted Tables, and figures, and assisted in writing and editing the article. A.M., A.A.B., G.M., M.L., and W.Y. provided guidance, review and editing throughout the article development. N.T. conceived the research idea, provided guidance on the research, and provided review and editing throughout the article development. All authors approved the final version of the submitted article.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
This work was supported by a Eugene Washington Patient-Centered Outcomes Research Institute (PCORI) Engagement award entitled, Building Capacity for Research to Address Climate-Impacted Health Conditions, #EACB-23028 and an U.S. Environmental Protection Agency (EPA) award entitled, Partnering for Resilient Opportunities to Eliminate Cumulative Toxic (PROTECT) Health Effects from Wildfire PM2.5 in Environmental Justice Communities, #84048101.
1
Kristie L Ebi et al., ‘Hot Weather and Heat Extremes: Health Risks’, The Lancet 398, no. 10301 (21 August 2021): 698–708, https://doi.org/10.1016/S0140–6736(21)01208–3; CDC, ‘Extreme Heat’, Centers for Disease Control and Prevention, 30 May 2023, ![]() .
.
2
4
Noam Rosenthal et al., ‘Population Co-Exposure to Extreme Heat and Wildfire Smoke Pollution in California during 2020’, Environmental Research: Climate 1 (1 December 2022): 025004, https://doi.org/10.1088/2752–5295/ac860e; Md Mostafijur Rahman et al., ‘The Effects of Coexposure to Extremes of Heat and Particulate Air Pollution on Mortality in California: Implications for Climate Change’, American Journal of Respiratory and Critical Care Medicine 206, no. 9 (1 November 2022): 1117–27, ![]() .
.
5
Nick Watts et al., ‘Health and Climate Change: Policy Responses to Protect Public Health’, The Lancet 386, no. 10006 (7 November 2015): 1861–1914, https://doi.org/10.1016/S0140–6736(15)60854–6; Seth B. Shonkoff et al., ‘The Climate Gap: Environmental Health and Equity Implications of Climate Change and Mitigation Policies in California—a Review of the Literature’, Climatic Change 109, no. 1 (1 December 2011): 485–503, ![]() .
.
6
Shonkoff et al., ‘The Climate Gap’.
7
8
Nick Watts et al., ‘Health and Climate Change: Policy Responses to Protect Public Health’, The Lancet 386, no. 10006 (7 November 2015): 1861–1914, https://doi.org/10.1016/S0140–6736(15)60854–6; Seth B. Shonkoff et al., ‘The Climate Gap: Environmental Health and Equity Implications of Climate Change and Mitigation Policies in California—a Review of the Literature’, Climatic Change 109, no. 1 (1 December 2011): 485–503, https://doi.org/10.1007/s10584–011-0310–7; Yu Yu et al., ‘Acute Health Impact of Wildfire-Related and Conventional PM2.5 in the United States: A Narrative Review’, Environmental Advances 12 (1 July 2023): 100179, https://doi.org/10.1016/j.envadv.2022.100179; Michael T. Schmeltz and Peter J. Marcotullio, ‘Examination of Human Health Impacts Due to Adverse Climate Events Through the Use of Vulnerability Mapping: A Scoping Review’, International Journal of Environmental Research and Public Health 16, no. 17 (September 2019): 3091, ![]() .
.
9
Harriet Bulkeley, ‘Cities and the Governing of Climate Change’, Annual Review of Environment and Resources 35, no. 1 (2010): 229–53, https://doi.org/10.1146/annurev-environ-072809–101747; Harald Fuhr, Thomas Hickmann, and Kristine Kern, ‘The Role of Cities in Multi-Level Climate Governance: Local Climate Policies and the 1.5°C Target’, Current Opinion in Environmental Sustainability, 1.5°C Climate change and urban areas, 30 (1 February 2018): 1–6, ![]() .
.
10
11
Diezmartínez and Short Gianotti.
12
13
Benjamin K. Sovacool, ‘The Complexity of Climate Justice’, Nature Climate Change 3, no. 11 (November 2013): 959–60, https://doi.org/10.1038/nclimate2037; E. Lisa F. Schipper, ‘Maladaptation: When Adaptation to Climate Change Goes Very Wrong’, One Earth 3, no. 4 (23 October 2020): 409–14, ![]() .
.
14
Leona F. Davis and Mónica D. Ramírez-Andreotta, ‘Participatory Research for Environmental Justice: A Critical Interpretive Synthesis’, Environmental Health Perspectives 129, no. 2 (February 2021): 026001, https://doi.org/10.1289/EHP6274; Christopher Bacon et al., ‘Introduction to Empowered Partnerships: Community-Based Participatory Action Research for Environmental Justice’, Environmental Justice 6, no. 1 (February 2013): 1–8, ![]() .
.
15
Meredith Minkler and Nina Wallerstein, eds., Community-Based Participatory Research for Health: From Process to Outcomes, 2nd ed (San Francisco, CA: Jossey-Bass, 2008); B. A. Israel et al., ‘Review of Community-Based Research: Assessing Partnership Approaches to Improve Public Health’, Annual Review of Public Health 19 (1998): 173–202, ![]() .
.
16
Bacon et al., ‘Introduction to Empowered Partnerships’.
18
‘U.S. Census Bureau QuickFacts’.
19
‘U.S. Census Bureau QuickFacts’.
20
23
24
Bacon et al., ‘Introduction to Empowered Partnerships’; Todd B. Ziegler et al., ‘Shifting from “Community-Placed” to “Community-Based” Research to Advance Health Equity: A Case Study of the Heatwaves, Housing, and Health: Increasing Climate Resiliency in Detroit (HHH) Partnership’, International Journal of Environmental Research and Public Health 16, no. 18 (January 2019): 3310, ![]() .
.
25
Athanasios Burlotos, Caleb Dresser, and Vivek Shandas, ‘Portland’s Response to the Western North American Heatwave: A Brief Report’, Disaster Medicine and Public Health Preparedness 17 (3 November 2023): e522, https://doi.org/10.1017/dmp.2023.184; Brooke G. Anderson and Michelle L. Bell, ‘Weather-Related Mortality’, Epidemiology (Cambridge, Mass.) 20, no. 2 (March 2009): 205–13, ![]() .
.
26
Alana Hansen et al., ‘Perceptions of Heat-Susceptibility in Older Persons: Barriers to Adaptation’, International Journal of Environmental Research and Public Health 8, no. 12 (December 2011): 4714–28, https://doi.org/10.3390/ijerph8124714; Jason L Rhoades, James S Gruber, and Bill Horton, ‘Developing an In-Depth Understanding of Elderly Adult’s Vulnerability to Climate Change’, The Gerontologist 58, no. 3 (8 May 2018): 567–77, ![]() .
.
27
28
29
30
Herbert et al.
31
Herbert et al.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.