
Abstract
Background:
Scientific evidence shows that hazardous industrial facilities are disproportionately distributed among socially deprived communities; however, environmental distributive justice research in Europe is still in its early stages, and the combined effect of contamination and socioeconomic deprivation on health has seldom been assessed. This study aims to assess environmental health inequalities in communities (i.e., municipalities) followed up by the Italian epidemiological surveillance system of contaminated sites (SENTIERI).
Methods:
Municipalities close to major Italian contaminated sites of interest for remediation were classified into least and most deprived according to regional quintiles of deprivation; standardized mortality ratios (SMR) for general, neoplastic, and premature mortality were aggregated using meta-analysis (meta-SMRs with 90% confidence interval [CI]). Findings were stratified by geographical macro-area.
Results:
Fifty-five percent of southern municipalities are in the most deprived group. Meta-SMRs show a significant excess for men in the most deprived group (general: 104 [90% CI 103–106]; neoplastic: 104 [90% CI 102–106]; premature: 102 [90% CI 100–104]) and for general mortality in women in both least deprived (102 [90% CI 100–103]) and most deprived municipalities (105 [90% CI 104–107]). The findings are confirmed at a macro-area level. General mortality is highest in southern women in the most deprived group (106 [90% CI 104–108]).
Discussion:
There is an unequal distribution of major contaminated sites by municipality deprivation level in the South of Italy. Evidence of the Italian North–South divide is present for inequalities associated with contaminated sites.
Conclusions:
Findings from SENTIERI should be integrated with evidence from ad hoc local epidemiological monitoring systems to provide information for decision-making processes at different administrative levels.
Introduction
There is wide evidence that contaminated sites tend to be disproportionately located next to socioeconomically deprived communities. 1 Deprivation itself is also directly associated with poor health: thus, such populations can be affected by the double burden of social and environmental risk factors. 2 Furthermore, in the case of contaminated sites resulting from pollution of large industrial plants, the socioeconomic evolution of communities living in their neighborhood is strictly interconnected with the presence of the sources of contamination (e.g., most of the labor force of the industries came from local populations). 3
Distributive justice is one of the main dimensions of environmental justice, which concerns equity in risks and benefits from economic activities causing hazardous contamination. 4 Studies on inequalities and inequities in the distribution of contaminated sites are abundant 5 : most of them have been conducted in the United States, where the concept itself of environmental justice emerged in association with racial and ethnic discrimination, 6 whereas in Europe environmental justice issues are predominantly perceived, analyzed, and framed in terms of social categories. 7 Research on environmental health inequalities and inequities associated with contaminated sites is at its early stages in Europe. However, the number of such studies is growing, generally showing a disproportionate distribution of environmental pressures in socioeconomic fragile communities or disadvantaged groups. 8
In the last Conference of the ministries of the Environment and the Health sectors of the WHO European Region, the combined topic of “contaminated sites and waste management” was identified among the seven priorities for action, highlighting the need for minimizing the effects of environmental chemical contaminants on vulnerable communities and groups. 9 Furthermore, in the WHO Europe second assessment report on environmental health inequalities, the need of defining priorities for remediation activities at the country level, having identified areas and contaminated sites with the highest levels of inequity, was identified among the strategic mitigation action for the topic of contaminated sites. 10
SENTIERI project (Epidemiological Study of Residents in Italian Contaminated Sites) is a national surveillance programme, funded by Italian Ministry of Health since 2006, and coordinated by the Italian National Health Institute (ISS), which evaluates the health profile of general populations (∼6,000,000 subjects) residing in those municipalities (>300) included in 46 main Italian sites of interest for environmental remediation.
The aims of the project, which adopts an ecological study design, require a specific outcomes selection to take into consideration the ones for which environmental exposure is suspected or ascertained to have an etiologic role. SENTIERI has been dealing with the complexity of the relation between area contamination and health effects focusing on those causes identified a priori from the epidemiological evidence of their association with selected environmental exposures. This is the basic and peculiar key aspect of SENTIERI, which requires a periodical appropriate scientific literature searching, and evaluation of the strength of causal association for each cause combined with different exposures.
Sites of interest for environmental remediation show a relevant environmental contamination, and a consequent potential impact on the health of residents. In SENTIERI, the possible health impact from environmental exposures is measured in terms of mortality, morbidity, incidence of neoplastic diseases, prevalence of congenital anomalies. The last report includes also data about children, adolescents, and young adults. 11
When found appropriate, SENTIERI makes public health and scientific research recommendations.
The complexity of the project needs an extended multidisciplinary working group (epidemiologists, statisticians, toxicologists, doctors, etc.), and a national network of research institutions, as well as technical and local sanitary structures.
Since 2012, the SENTIERI Project has been providing the Italian National Statistical System (SISTAN) with its results. SISTAN is a network of public and private structures that make available official statistical information to the national and international organizations.
Up-to-date, SENTIERI has published five reports.11, 12 , 13 , 14 , 15
This study aims to assess inequalities in the distribution of environmental pressures due to contamination and health outcomes considering socioeconomic deprivation in Italian municipalities under SENTIERI monitoring.
Methods
The analysis was conducted considering the 319 municipalities included in the fifth SENTIERI report. 11 For each municipality, an ad hoc deprivation index (DI-SENTIERI) was calculated, combining four indicators derived from 2011 National Census data: percentage of residents with a primary education degree or below, percentage of the active population unemployed or searching for a first job, percentage of rented habitations, and household crowding (as dwellers/100 m 2 ). Values for these indicators were normalized (z-score) at regional level and their sum was taken as the deprivation index for each municipality. Finally, municipalities were ranked at the regional level in quintiles (Q) of deprivation index and subsequently divided into two groups: Q1 and 2 were categorized as least deprived, whereas Q4 and 5 were classified as most deprived.
The health outcomes analyzed were municipal standardized mortality ratios (SMRs), computed using regional age-specific rates by gender as reference. SMRs for both genders were calculated for general, neoplastic, and premature mortality. The last is an implementation of the UN's Sustainable Development Goals indicator SDG 3.4.1, 16 measuring deaths in ages 30–69 from preventable causes (neoplasms, cardiovascular disease, chronic respiratory disease, and diabetes). Data for general and neoplastic mortality were previously utilized for the fifth SENTIERI report, relative to the period from 2006 to 2013; data for premature mortality were extracted anew, specifying a year range of 2007–2015. Mortality data aggregated at municipality level were extracted from the National mortality database available at the Statistical Service of the Italian National Institute of Health (Istituto Superiore di Sanità).
Finally, meta-analyses with random effects were employed to generate gender-specific meta-SMRs—with 90% confidence intervals—for the groups of least deprived and most deprived municipalities. Municipalities having less than five reported observations were excluded from the analysis. Heterogeneity was assessed with Higgins' I2 statistics. Owing to the increasing variability of deprivation values within municipalities as the populace increases, 17 separate meta-SMRs were computed excluding municipalities >50,000 residents. As previously described in Pasetto et al., 18 the rationale for meta-SMRs is they are suited as summary indicators for groups that are relatively homogenous in deprivation level but very heterogeneous in size, contamination sources, and other characteristics.
In addition, meta-SMRs for general mortality were calculated for the three Italian geographical macro-areas of North, Center, South and Great Island to account for long-standing socioeconomic differences among these territories, with a marked North–South divide. 19
All analyses were performed with STATA software v. 16.
Results
Most municipalities in SENTIERI surveillance are either from the North or the South and Great Islands (Sicily and Sardinia), with Central Italy only accounting for 10%. Out of 319 municipalities, 111 (34.8%) belonged to the least deprived group and 144 (45.1%) to the most deprived group; the latter comprised 29.5% of North, 50% of Center, and 55.8% of South and Great Islands municipalities (Fig. 1).
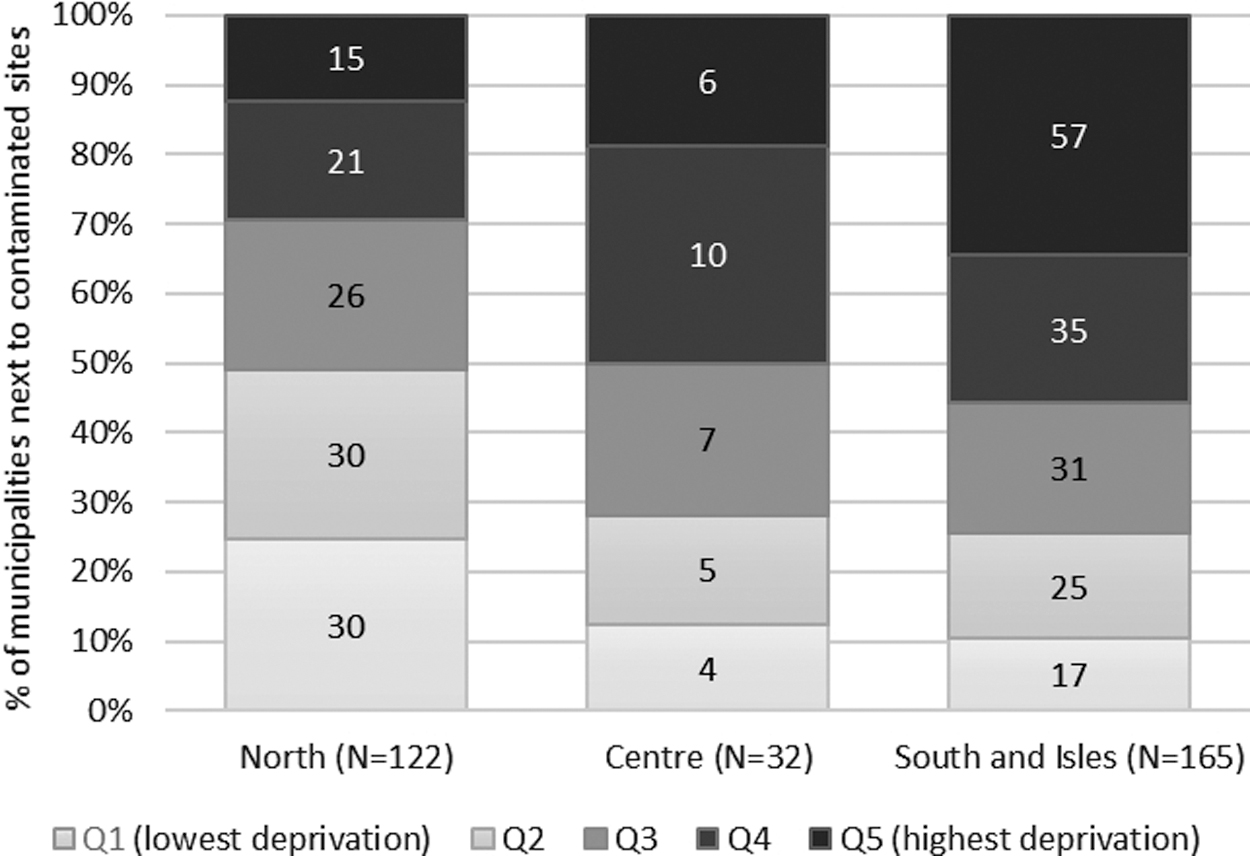
Number of SENTIERI municipalities by macro-area and quintile of deprivation (DI-SENTIERI from 2011 Census data).
National meta-analysis results are resumed in Table 1. Meta-SMRs in the most deprived group in men show a significant excess of cases relative to regional references for all three outcomes. General mortality for women is also significantly in excess in both groups, whereas female neoplastic mortality is significantly below the expected in the most deprived group.
Gender-Specific Meta-Standardized Mortality Ratios with 90% Confidence Interval by Deprivation Group
Observation periods were 2006–2013 for general and neoplastic mortality, and 2007–2015 for premature mortality.
Number of municipalities reporting five or more cases in the observation period.
Estimates with I2 < 50%.
Mortality rate between 30 and 69 years of age due to cardiovascular disease, cancer, diabetes, or chronic respiratory disease.
Municipalities with a population below 50,000 residents.
CI, confidence interval; meta-SMR, meta-analytic standardized mortality ratio; SDG, sustainable development goals.
General mortality is significantly higher in the most deprived group than in the least deprived group in both genders. A significant difference between groups is also highlighted for neoplastic mortality in men, whereas in women the estimate is higher in the least deprived group (although not statistically significant). Premature men mortality is higher for the most deprived municipalities (not statistically significant), whereas female estimates are juxtaposed.
Women have higher meta-SMRs than men for all outcomes in the least deprived group and for general mortality in the most deprived group. Higgins' I2 was >50% for most values, suggesting high variability of municipal SMRs within groups. Similar results were observed when limiting the analysis to municipalities with <50,000 residents.
Geographic stratification for general mortality (Table 2) confirms a pattern of higher meta-SMRs for the most deprived municipalities, both as significant excess from the expected and in comparison with the least deprived group, except for women in the North; however, the risk appears as significantly different only in women from South and Great Islands. Also, southern women in both groups show a significant excess from regional reference and higher estimates than men. I2 is >50% for most estimates.
Meta-Standardized Mortality Ratios with 90% Confidence Intervals for General Mortality by Macro-Area
Number of municipalities reporting five or more cases in the observation period.
Estimates with I2 < 50%.
G.I, Great Islands.
Discussion
Results of the study show that communities sited next to contaminated sites in the Italian South are disproportionally characterized by higher socioeconomic deprivation, confirming observations of a similar study carried out with the DI-SENTIERI computed with 2001 National Census data. 10 Sixty-four percent of municipalities in the most deprived group are located in the South and Great Islands. Furthermore, the South carries a socioeconomic disadvantage compared with the rest of Italy: since DI-SENTIERI is normalized and ranked at the regional level, the most deprived municipalities in the South are bound to fare worse than their northern and central counterparts in the same quintiles. Thus, unequal distribution of contaminated sites on these populations could represent an environmental injustice at both the local and national level. The wealth gradient from North to South of Italy has complex historical reasons that predate industrialization 20 ; however, the gap was widened in the postwar period when southern regions were “colonized” with massive heavy industrial complexes that had no connection with the pre-existing economy and failed to bring the expected development for local communities. 21
SMRs for general mortality from the fifth SENTIERI report show an excess risk in 8 years of 4% (+5,267 observed cases) in men and 5% (+6,725 observed cases) in women. 11 Meta-SMRs in this study provide similar risk estimates for the most deprived municipalities, indicating that these populations contribute the most to the mortality excesses in SENTIERI. Also, general mortality in these communities exceeds the risk versus the reference populations in the least deprived municipalities by about 4% in men and 3% in women.
Neoplastic and premature mortality in the most deprived group is also significantly in excess for men. A similar association between DI-SENTIERI and male cancer mortality at the municipality level was previously observed in three Italian regions. 17
In the least deprived population, women have higher estimates than men for all three outcomes, especially in the North; the risks for men in the same municipalities are comparable with the regional standard. Such difference may indicate that, when socioeconomic gaps are removed, the net effect of environmental hazards is stronger on women or that the indicator of deprivation used is more representative of deprivation for men than for women, as discussed by Minichilli et al. 17
A North–South gradient is observed in female general mortality within the most deprived group: women from southern municipalities with greater disadvantage are the subgroup with the highest SMR and the only ones in the most deprived population whose estimate exceeds that of their male counterparts.
Results are influenced by the limitations of the indicator of deprivation, which express the deprivation for the whole population using only a few, although relevant, variables. Furthermore, it is not possible to identify which had been conditions of deprivation when the industrial complexes had been established and opened. Existing knowledge makes it impossible to establish whether conditions deteriorated after industrialization and subsequent contamination. What is clear is that most communities close to contaminated sites in southern Italy belong to the most deprived groups and have a higher risk of mortality in both genders.
A second limitation of the study comes from the aggregated nature of SENTIERI and National Census data sets: ecological evidence of inequalities in environmental pressures and health is not enough to make claims about the social causes of injustice 22 or even to assert that there is “injustice” at all 23 —although it can be argued that a significant disparity toward a community is always unjust. 24 Nonetheless, a similar association between social deprivation, disproportionate environmental burden, and health inequalities was already observed in assessments from other European countries (e.g., Refs.8, 25 , 26 , 27 , 28 ), suggesting that a causal relationship could exist. In the Italian context, the evolution of the Network of Longitudinal Metropolitan Studies, which includes detailed socioeconomic data at the individual level among the available information to assess health inequalities, 29 is a promising effort that paved the way for to the assessment of environmental health inequalities at the local level (at least in some areas of the country) using socioeconomic data at the submunicipal area and individual levels. Upcoming local epidemiological monitoring systems should include socioeconomic data at individual and census tract levels (e.g., from record linkage or sampling) to better analyze disproportions in the distribution of contaminants and health outcomes. 30 Nevertheless, a preliminary assessment with such information has been carried out in only one of the Italian heavily contaminated sites. 31
Finally, this study is conditioned from the use of administrative units as a proxy for the population potentially exposed to noxious factors from contaminated sites—that is, a unit-hazard coincidence approach1, 32 : such approximations preclude any strong inference on the results, consistently with the exploratory purpose of the study.
Nevertheless, in contaminated sites the weight of evidence from ecological-area studies increases with the overall knowledge on environmental and health issues available in each site (e.g., environmental data, collected for administrative or research purpose, local ad hoc studies on environmental and/or health issues). This is a key aspect of SENTIERI approach. 33
Conclusions
An assessment at a national level is helpful to understand geographical patterns of environmental injustice associated with the distribution of environmental hazards and health risk by deprivation at the community level. Nevertheless, it does not help in explaining the complexity of the relationship between the evolution of each industrial complex and their surrounding communities in terms of their social profiles and health. Every site and every community have their own history, which cannot be described by a national monitoring system. 3 Therefore, national assessments on distributive justice should be integrated with the reinforcement of local environmental and epidemiological monitoring programs oriented to assess exposure and health inequalities within local communities. 10
The combination of national and local approaches can give complementary information for policies at different administrative levels. The present country assessment within SENTIERI should be integrated with local assessments as soon as small-area and individual data became available.
Footnotes
Authors' Contributions
R.P. contributed to the conceptualization, methodology, formal analysis, writing of the original draft preparation, and reviewing and editing of the final article. D.D.F. contributed to the conceptualization, writing of the original draft preparation, and in reviewing and editing of the final article. M.D.S. contributed to the formal analysis. R.P. contributed to the methodology and the formal analysis. A.Z. contributed to the writing of the original draft preparation and in reviewing and editing the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Italian Ministry of Health “SENTIERI Project: implementation of the permanent epidemiological surveillance system of the populations residing in the contaminated sites of interest for reclamation”. Chap. 4100/39 funding 2018.