
Abstract
Objective:
To compare the efficacy and safety of robot-assisted laparoscopic radical prostatectomy (RARP) performed using the KangDuo surgical robot system to the da Vinci Si robotic system in clinically localized prostate cancer (KD-RARP vs DV-RARP).
Methods:
A total of 16 patients underwent extraperitoneal KD-RARP performed by a single experienced surgeon using the KangDuo surgical robot system between May 2021 and August 2021. The data were prospectively collected. The most recent 16 cases of extraperitoneal DV-RARP performed in 2021 by the same surgeon were selected from a prospectively maintained database for comparison to prevent operator variability. Preoperative, perioperative, and postoperative data were collected and compared between the two groups.
Results:
No significant difference was noted between the two groups in terms of basic clinical characteristics. All operations were performed successfully without open or traditional laparoscopic conversion. KD-RARP had a significantly longer operation time compared with DV-RARP (127 [107–159] vs 70.5 [54–90] minutes, p < 0.001). No significant differences between the two groups were observed in neurovascular bundle sparing, estimated blood loss, postoperative hospital stay duration, complications, positive surgical margins, biochemical recurrence, and continence recovery 3 months after catheter removal.
Conclusions:
RARP using the KangDuo surgical robot system achieved similar short-term oncological and functional outcomes with a disadvantage in operation time compared with the da Vinci Si robotic system. A multicenter randomized clinical trial with a larger sample size is needed for more experience.
Introduction
Prostate cancer is the second most common cancer in men worldwide. 1 Early diagnosis became possible with the increased use of prostate-specific antigen (PSA) screening, which made the management of clinically localized prostate cancer common.
In general, radical prostatectomy is one of the standard treatments for prostate cancer. 2 With the development of medical equipment, radical prostatectomy evolved from open radical prostatectomy to laparoscopic radical prostatectomy (LRP) and then robot-assisted laparoscopic radical prostatectomy (RARP). 3 –5
Open surgery is accompanied by a high incidence of complications. Therefore, a minimally invasive alternative was expected to improve perioperative outcomes. The first LRP was performed by Schuessler et al. 4 At the time, minimally invasive laparoscopic surgery was widely performed due to better perioperative outcomes. 6 Laparoscopic suturing was technically challenging due to limited dexterity compared with open surgery, and poor hand–eye coordination in laparoscopic surgery resulted in unsatisfactory ergonomics. All these restrictions contribute to the long learning curve associated with anastomosis in LRP. 7 Even for skilled laparoscopic surgeons, urethrovesical anastomosis is still demanding.
Robot-assisted laparoscopic surgery is considered a major leap in minimally invasive surgery, which combines the dexterity of open surgery and the microinvasive technique of laparoscopic surgery. RARP was first reported by Binder and Kramer. 5 Since then, the technique has been in fast development and has become an established modality for clinically localized prostate cancer. 8 The most critical disadvantage of the da Vinci® system is its cost. 9
Various robotic platforms have been developed in other countries, such as the Revo-i system and Senhance robotic platform. The eye tracking system of Senhance robotic platform allows the camera to be controlled by viewing various parts of the operative field, and the handles for manipulating the instruments have haptic feedback, which is helpful for suturing and dissection. 10 The Revo-i system is a master slave system similar to the da Vinci system, with more reusable times of instruments, and it also incorporates haptic feedback, but the range of motion of the needle driver is less than that in the da Vinci system. 11 In China, the developed KangDuo surgical robot system demonstrated excellent performance in partial nephrectomy, pyeloplasty, and radical prostatectomy. 12 –16 To the best of our knowledge, this is the first comparison of RARP performed using the KangDuo surgical robot system (KD-RARP) to RARP performed using the da Vinci Si robotic system (DV-RARP) in the treatment of clinically localized prostate cancer.
Materials and Methods
A total of 16 patients underwent KD-RARP performed by a single experienced surgeon using the first generation of the KangDuo surgical robot system (KD-SR-01) between May 2021 and August 2021 in Peking University First Hospital. The data were prospectively collected. The most recent 16 cases of DV-RARP performed in 2021 by the same surgeon were selected from a prospectively maintained database for comparison to prevent operator variability. All operations were performed through the extraperitoneal route by the same expert surgeon (Prof. Cheng Shen) with experience of more than 400 RARP cases (Fig. 1). Preoperative, perioperative, and postoperative data were collected and compared between the two groups. The study protocols were approved by the Institutional Review Board of Peking University First Hospital (Beijing, China).
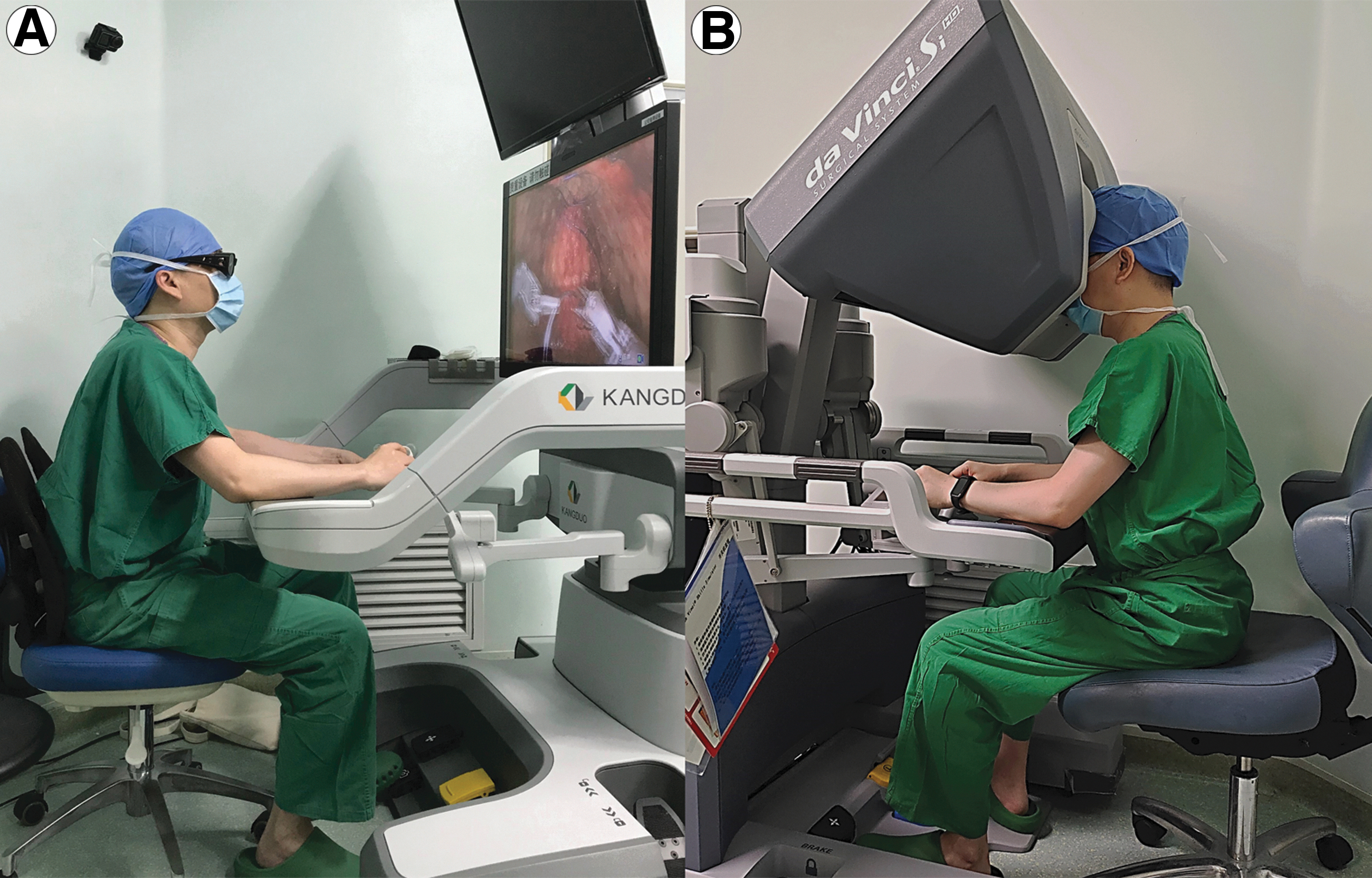
Relative location of the surgeon to the console.
Both the KD-RARP and DV-RARP were performed using essentially the same technique. The patient was placed in the supine position first. After insertion of a Foley catheter, the patient was placed in the Trendelenburg position. The port distribution is shown in Figure 2. The surgical technique has been previously described in detail. 14 Two instrument arms and one camera arm were used in both groups. The main technique consisted of suturing/ligation of the dorsal venous plexus, bladder neck dissection, dissection of the Denonvilliers' fascia, prostatic pedicles, urethra, posterior reconstruction, and vesicourethral anastomosis. Neurovascular bundle (NVB) sparing procedure was performed according to preoperative risk stratification.
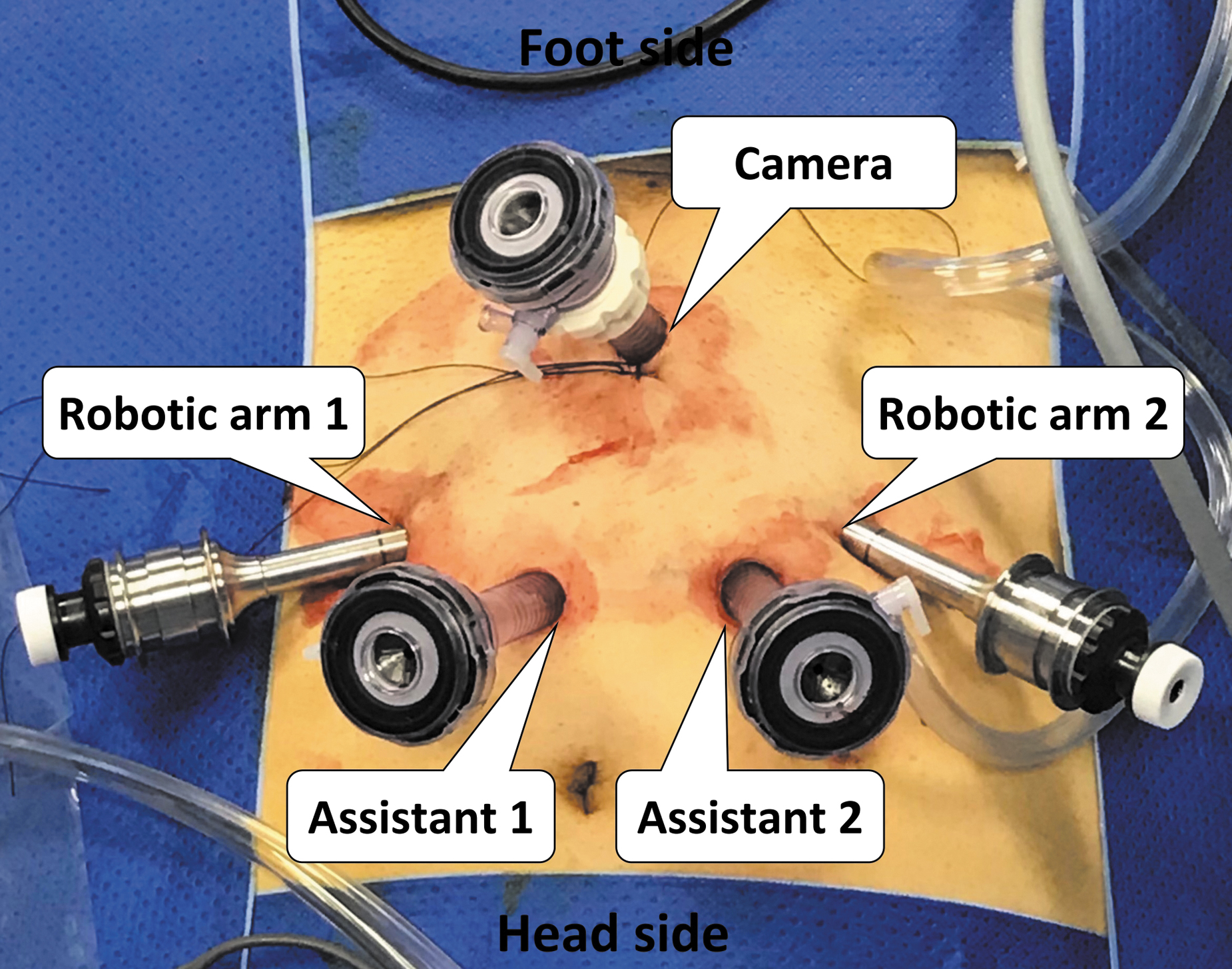
The port distribution of extraperitoneal robot-assisted laparoscopic radical prostatectomy. The port distribution of extraperitoneal robot-assisted laparoscopic radical prostatectomy performed using the KD-SR-01 and da Vinci Si was the same. A 2 cm skin incision about 3 to 4 cm above the pubic symphysis was made for initial access into the retropubic space and subsequently as a camera port. A balloon was inserted and insufflated to establish, expand, and maintain the retropubic space. Next, two extraperitoneal ports were placed about 8 cm from the camera port along the exterior margin of the rectus abdomen under direct vision with the left trocar (robotic arm 1) for a bipolar Maryland grasper and the right trocar (robotic arm 2) for a monopolar scissor or large needle driver. Additional ports for assistant were placed at the midpoints of the line joining the robotic arm 1/2 and the umbilicus (assistant 1/2) for retraction, suction, and clip placement.
Preoperative, perioperative, and postoperative data were collected and compared prospectively. Preoperative data included age, body mass index (BMI), preoperative PSA, and biopsy Gleason score. Perioperative data included estimated blood loss (EBL), transfusion rate, operation time, and postoperative length of stay. The operation time was defined as the period from the incision of the skin to the end of the skin suture. Postoperative data included surgical margin, biochemical recurrence, and continence rate. Complications were evaluated according to the Clavien–Dindo system. 17 A positive surgical margin (PSM) occurred when the tumor was found on the inked surface of the prostate specimen. Biochemical recurrence was identified when the postoperative level of total serum prostate-specific antigen (tPSA) was more than 0.2 ng/mL. Continence was defined as the use of no more than one pad daily or urine leakage of <20 g as determined by a 24-hour pad weight test.
All of the data were analyzed using SPSS 26.0 (IBM SPSS, Armonk, NY). The numeric parameters were expressed as a median (range) and compared using Student's t-test or Mann–Whitney test. The nominal data were expressed as a percentage and compared using the chi-square test or Fisher's exact test. The result was considered statistically significant when the p-value was <0.05.
Results
The baseline characteristics of the two groups are shown in Table 1. The two groups were statistically similar in terms of age, BMI, and the ratio of neo-adjuvant hormonal therapy. A total of seven patients received neoadjuvant hormonal therapy at other hospitals before they underwent surgery in our center. The preoperative oncological characteristics, such as preoperative PSA, prostate volume, biopsy Gleason score, and clinical tumor stage, were also statistically similar between the two groups (Table 1).
Demographic and Preoperative Characteristics of the Patients
Mann–Whitney U test.
Fisher's exact test.
BMI = body mass index; DV-RARP = robot-assisted laparoscopic radical prostatectomy performed using the da Vinci Si robotic system; KD-RARP = robot-assisted laparoscopic radical prostatectomy performed using the KangDuo surgical robot system; PSA = prostate-specific antigen.
The intraoperative and perioperative information is presented in Table 2. All surgeries were completed successfully without laparoscopic or open conversion. A bilateral and unilateral NVB sparing procedures were performed in 1 (6.3%) and 8 (25.0%) cases, respectively, in the KD-RARP group vs 2 (12.5%) and 3 (18.8%) cases, respectively, in the DV-RARP group (p = 0.867). No pelvic lymph node dissection was performed in any patient in both groups. KD-RARP had a significantly longer operation time compared with DV-RARP (127 [107–159] vs 70.5 [54–90] minutes, p < 0.001). There was no statistically significant difference in the EBL and postoperative hospital stay duration between the two groups. The postoperative hospital stay duration in the KD-RARP and DV-RARP groups was 5 (range 4–10) and 6.5 (range 5–10) days, respectively (p = 0.254).
Intraoperative and Perioperative Variables
Mann–Whitney U test.
EBL = estimated blood loss; NVB = neurovascular bundle; PLND = pelvic lymph node dissection.
Table 3 shows the follow-up data for the two groups. No difference was observed in PSM rate, pathological Gleason score, pathological tumor stage, 3-month postoperative tPSA, and urinary continence recovery 3 months after catheter removal. The PSM rate was 25% (4/16) and 12.5% (2/16) in the KD-RARP and DV-RARP groups, respectively (p = 0.654). The postoperative serum tPSA was comparable between the two groups and no biochemical recurrence was noted. The urinary continence rate was 93.8% (15/16) in the KD-RARP group vs 87.5% (14/16) in the DV-RARP group 3 months after catheter removal (p = 0.780). No severe intraoperative or postoperative complications (Clavien–Dindo grade >Ш) were noted in either group. Only one patient developed postoperative absorption fever (Clavien–Dindo grade І) in the KD-RARP group.
Follow-Up Data
Fisher's exact test.
Mann–Whitney U test.
PSM = positive surgical margin.
Discussion
In 1997, Raboy and colleagues reported the first case of extraperitoneal LRP. 18 Six years later in 2003, RARP through the extraperitoneal approach was performed using the da Vinci robotic system. 19 The extraperitoneal approach allows for direct access to the retropubic space, which shortens the surgery duration. 20 This approach has also been associated with faster recovery after surgery and lower risks of intra-abdominal complications as compared with the transperitoneal technique, especially in patients who previously underwent abdominal surgery. 21 Therefore, the radical prostatectomy (RP) through the extraperitoneal approach was selected to assess the clinical performance of the KD-SR-01 system in lower urinary tract surgery.
In terms of effectiveness, all surgeries were completed without open or laparoscopic conversion. No significant difference in PSM rate was noted between the two groups, while the PSM rate was slightly higher in the KD-RARP group. No biochemical recurrence occurred in either of the groups. All of the above results demonstrated the effectiveness of RARP using the KD-SR-01 system.
There are several possible reasons for the relatively higher PSM rate. According to the pathological stage, 3 (75%) patients with PSM had pT3 disease and PSM peaked in 3 (75%) patients. The high pathological staging and PSM site (unclear visualization of the apex) may help explain the relatively higher rate of PSM, 22 which might also be related to the relatively small cohort in the present study. Furthermore, it should be mentioned that all cases were part of the surgeon's learning curve for the KD-SR-01 system. Hence, the results are expected to improve with additional experience. Focal positive margins after RP do not significantly affect biochemical recurrence-free survival in patients with prostate cancer. 23 In this study, no biochemical recurrence occurred 3 months after surgery.
As for safety, no significant difference was noted between the two groups, and no severe intraoperative or postoperative complications (Clavien–Dindo grade >Ш) were reported. The urinary continence rate was comparable 3 months after catheter removal. These results demonstrate the safety of RARP using the KD-SR-01 system.
Continence is directly related to the quality of life for patients after radical prostatectomy, in which the structure for maintaining continence is disrupted. The recovery of continence mainly depends on both the vesicourethral anastomosis and dissection process, which influence the preservation of the related structure, including NVB, bladder neck, and urethral length. 24 The quality of vesicourethral anastomosis and dissection during RARP is strongly associated with both the operative experience of the surgeon and the performance of the robotic platform. The surgeries in the two groups were performed by the same surgeon in the same period, so that the quality of vesicourethral anastomosis and dissection was similar between the two robotic platforms.
To reach the same level of performance in RARP with the da Vinci Si system, the surgeon required a longer operation time using the new robotic platform. Although the surgeon had experience with more than 400 cases of RARP using the da Vinci Si system, there was still a new learning curve for RARP using the KD-SR-01 system. 14 Thus, the outcomes were encouraging.
Various robotic platforms have been developed in other countries, such as the Revo-i system and Senhance robotic platform. Their performance in RARP has been previously reported. 10,11 Between August 2016 and February 2017, a total of 17 patients underwent RARP using the Revo-i robotic system with a median console time of 92 minutes. 11 From November 2018 until October 2020, 127 RARP procedures have been performed using the Senhance robotic system with a median operation time of 180 minutes. 10 The median console time and operation time of KD-RARP were 87 and 127 minutes, respectively, which were not inferior to the Revo-i and Senhance robotic systems.
The KD-SR-01 system provides several important features compared with the da Vinci Si system. First, the surgical KD-SR-01 system console has an open vision system. Compared with the immersive vision system in the da Vinci Si robotic system, the open vision system has several advantages. On one hand, neck stiffness likely occurs due to maintaining a flexion posture for long periods during robotic surgery with the da Vinci Si robotic system. 25 Comparatively, the open console of the KD-SR-01 system allows the surgeon to maintain a natural posture and perform slight adjustments of the neck, which can relieve neck stiffness. On the other hand, the open console ensures active communication between the primary surgeon and the assistant. Second, the arms are independent in the da Vinci Si robotic system and grouped in the KD-SR-01 system. The boom of the KD-SR-01 system is an adjustable and rotatable support that moves the grouped arms to allow for easy access to different quadrants. It enables the arms to rotate synchronously to adjust to the position of the patient without the need to reposition the entire patient care system.
Third, the vision cart in the KD-SR-01 system is compatible with conventional three-dimensional laparoscopes, which can reduce costs and promote the widespread application. Furthermore, the common hand-held three-dimensional laparoscope is thin and portable, allowing the assistant to support trocar insertion. Although the laparoscope has become lighter with a lower profile in Xi system, the proprietary laparoscope in the da Vinci Si robotic system is relatively large and heavy, thereby rendering manual maneuvers especially difficult.
Various innovations have been developed to enhance the robotic system, such as enhanced imaging using fluorescence, robot-assisted microsurgery, completely independent arms, real-time haptic feedback, single-port surgery, remote surgery, and automated robotic surgery with artificial intelligence. Enhanced imaging using fluorescence can facilitate precise removal of the prostate and lymph node and protect the NVB in RARP. 26 Robot-assisted microsurgery eliminates physiological tremors and provides visual magnification in male infertility and andrology procedures. 27 Completely independent arms and real-time haptic feedback work well in RARP. 10 Single-site robot-assisted pyeloplasty is related to excellent short-term clinical outcomes with good cosmetic results. 28 Remote surgery can eliminate geographical constraints and transatlantic tele-cholecystectomy is considered the first telesurgery in the world. 29 The first telesurgery based on 5G technology was performed using the KangDuo surgical robot system. 30 Autonomous robotic laparoscopic surgery for intestinal anastomosis was successfully performed using an enhanced autonomous strategy. 31 The development of robotic technology requires more innovation in the future.
The present study had some limitations. The da Vinci Si group data were retrospectively reviewed, although the data were collected from a prospectively maintained database. Notably, all surgeries were performed in 2021 by a single surgeon, which ensured a more accurate comparison. Second, no comparison of the erectile function outcomes was performed because the follow-up was too short to adequately address this issue. Third, the surgical cost comparison was not conducted since the price of the KangDuo surgical robot system has not yet been determined. Fourth, the follow-up period was relatively short and the oncological and functional outcomes should be evaluated further in the future. Fifth, the confounding factors might have a greater impact on the outcome due to the small sample size, which reduced the reliability of the study to some extent, so that a randomized clinical trial with a larger sample size is needed for more experience.
Conclusions
RARP using the KD-SR-01 system achieved similar short-term oncological and functional outcomes while showing a disadvantage in operation time compared with the da Vinci Si robotic system. A multicenter randomized clinical trial with a larger sample size is needed for more experience.
Footnotes
Acknowledgment
The authors are grateful to Xiang Chen who helped in the preparation of this article.
Authors' Contributions
S.F.: Conceptualization; Formal analysis; Project administration; and Writing—original draft. H.H.: Conceptualization; Formal analysis; Project administration; and Writing—original draft. S.C.: Conceptualization; Formal analysis; Project administration; and Writing—original draft. J.W.: Data curation and Investigation. X.D.: Data curation and Investigation. M.Z.: Data curation and Investigation. X.C.: Data curation and Investigation. Z.L.: Data curation and Investigation. S.X.: Data curation and Investigation. G.H.: Data curation and Investigation. J.Z.: Data curation and Investigation. Z.Z.: Resources; and Writing—review and editing. W.Y.: Resources; and Writing—review and editing. L.C.: Conceptualization; Resources; and Writing—review and editing. C.S.: Conceptualization; Resources; and Writing—review and editing. L.Z.: Conceptualization; Resources; and Writing—review and editing. X.L.: Conceptualization; Resources; and Writing—review and editing.
Author Disclosure Statement
C.L. is the cofounder and stock owner of Suzhou Kangduo Robot Co., Ltd. All other authors have nothing to declare.
Funding Information
The study was supported by the Horizontal Subject of Peking University First Hospital (5001705).