
Abstract
Introduction:
The evidence for prostatic urethral lift (PUL), in treating lower urinary tract symptoms/benign prostatic hyperplasia (BPH) in men with obstructive median lobes (OMLs), has grown. In this study, we present the first detailed comparison of outcomes between OML patients treated with PUL in controlled and real-world settings to relevant comparators (subjects treated with transurethral resection of the prostate [TURP] and sham in randomized controlled trials [RCTs]) to demonstrate similar symptom, safety, and patient experience outcomes.
Materials and Methods:
Symptom and safety outcomes and patient satisfaction were compared through 12 months among controlled PUL studies: BPH6 RCT (35 men randomized to TURP); L.I.F.T. pivotal RCT in subjects with lateral lobe obstruction (66 subjects randomized to sham) and MedLift, an U.S. Food and Drug Administration-approved Investigational Device Exemption (IDE) extension of the L.I.F.T. trial (45 men with OML). Symptom improvement, catheterization, and adverse event rates were compared between MedLift subjects and OML patients (n = 187) from the large real-world retrospective (RWR) study of PUL filtered on baseline characteristics to approximate the MedLift population.
Results:
Posttreatment, International Prostate Symptoms Score (IPSS) improvement for MedLift subjects was 170% greater compared with sham at 3 months with significantly better quality of life (QoL), Qmax, and benign prostatic hyperplasia impact index (BPHII). Compared with TURP, MedLift IPSS and QoL improved significantly better at 1 and 3 months and with superior ejaculatory function scores at all time points after PUL. IPSS, QoL, postvoid residual (PVR), and Qmax outcomes were equivalent between MedLift and RWR OML groups at 3, 6, and 12 months. RWR OML patients did not experience higher rates of overall adverse events compared with MedLift.
Conclusion:
Controlled and real-world outcomes confirm PUL is a safe and effective treatment for BPH patients with and without OML.
Introduction
Since its approval by the U.S. Food and Drug Administration (FDA) in 2013, prostatic urethral lift (PUL) for the treatment of bothersome lower urinary tract symptoms attributed to benign prostatic hyperplasia (BPH) has experienced a growth in adoption. 1,2 Today hundreds of thousands of men have been treated with PUL and it is considered a standard of care in the United States and abroad, with gland morphology and size assessment an important component of the initial evaluation. 3 –6 The procedure relieves urinary flow obstruction and provides patients with rapid, durable relief. 7,8 The rise of PUL has once again positioned minimally invasive surgical therapy (MIST) as an attractive option for patients unsuccessfully treated by medical therapy or with poor compliance, yet hesitant to undergo traditional surgery, a sentiment acknowledged by the European Association of Urology (EAU) and the American Urological Association (AUA). 6,9
The FDA indicates PUL for the treatment of BPH, including lateral and median lobe hyperplasia, in men with prostates no greater than 100 cc. This indication is based on review of randomized controlled trial (RCT), controlled clinical trial (CCT), and single-arm trial studies. Society guidelines, however, often provide recommendations that are narrowed, due to their more limited evaluation of published evidence. For instance, the AUA BPH guidelines state that only RCT and CCT studies are considered when crafting evidence-based updates, and thus limit PUL recommendation to only lateral lobe (LL) disease with a maximum prostate volume of 80 cc. The EAU BPH guidelines give a strong recommendation for PUL but limit the maximum volume to 70 cc and also exclude middle lobe.
Because the regulatory/legal indication for PUL is broader than the current academic guidelines, there has been extensive use of PUL to treat men with prostates outside of the guideline volume limit and with obstructive median lobe (OML). The MedLift study, an FDA-approved IDE extension of the L.I.F.T. pivotal trial, was the first study to compare PUL outcomes for OML to those for LL and concluded that PUL OML treatment was not inferior to LL treatment. 10 MedLift enrolled subjects with the same criteria as the L.I.F.T. trial (which randomized LL patients to either PUL or sham treatment), however patients presented with an ultrasound-defined OML. Utilizing the sham subjects from L.I.F.T. as controls for PUL OML treatment thus positions MedLift as a CCT. Within this study, we compare outcomes of OML patients treated with PUL in controlled and real-world settings to relevant comparator groups (i.e., subjects treated with transurethral resection of the prostate [TURP] and sham in RCT) to demonstrate similar symptom, safety, and patient experience outcomes.
Materials and Methods
Study protocol
Details of the four PUL studies used in this analysis have been published and are summarized in Table 1. The study protocols were in accordance with all applicable U.S. Federal and state laws and regulations, including 45 CFR 46 and the HIPAA Privacy Rule.
Design Details of Prostatic Urethral Lift Clinical Studies and Subjects Used for the Comparative Analysis
BPH = benign prostatic hyperplasia; BPHII = benign prostatic hyperplasia impact index; CCT = Controlled Clinical Trial; EJD = ejaculatory dysfunction; IPSS = International Prostate Symptoms Score; LL = lateral lobe; MSHQ = Male Sexual Health Questionnaire; OML = obstructive median lobe; PUL = prostatic urethral lift; PVR = postvoid residual; QoL = quality of life; RCT = randomized controlled trial; RWR = real-world retrospective; SHIM = Sexual Health Inventory for Men; TURP = transurethral resection of the prostate.
Study procedures
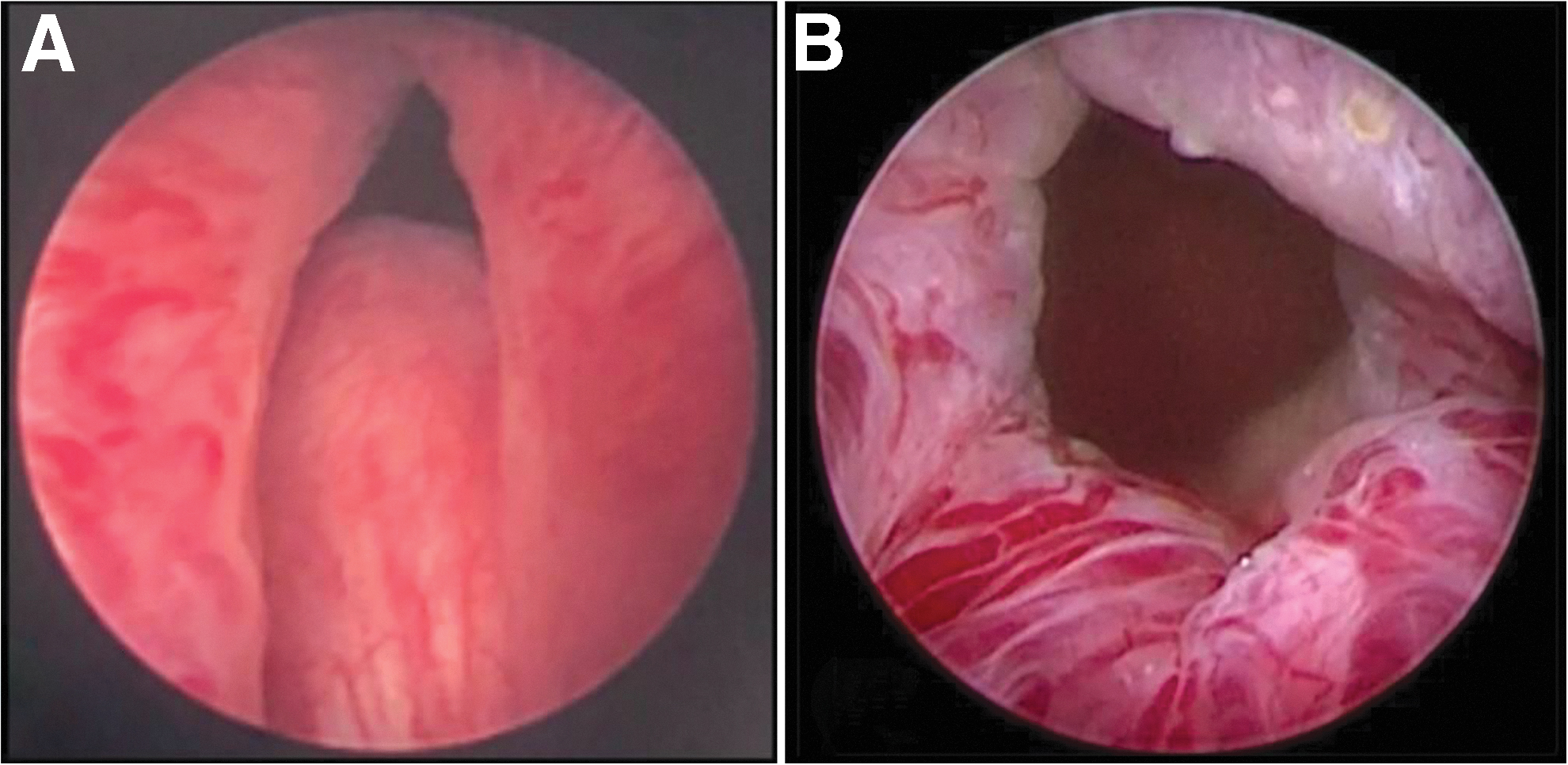
During the PUL procedure, small, transprostatic implants (UroLift System; NeoTract, Inc./Teleflex, Pleasanton, CA) are deployed under cystoscopic guidance, mechanically retracting obstructive prostatic lobes, and creating an anterior channel through the prostatic fossa (Fig. 1). In patients with OMLs, the base of the tissue protruding intravesicularly is retracted distally into the prostatic fossa and secured to either side of the urethra using the implant, thereby extending the channel to the bladder neck through displacement of the middle lobe as described in the MedLift CCT.
Cystoscopic evaluation of median lobe obstruction
In the pivotal L.I.F.T. study, a sham control procedure was conducted to mimic the PUL experience as closely as possible: a surgical drape was used as a visual partition and a rigid cystoscopy performed, with the surgeon calling for devices that were opened but not deployed. A disposable biopsy device was deployed to simulate device sounds. TURP control procedures in the BPH6 RCT were conducted by experienced urologists in accordance with their standard operating procedure.
For the Real-World Retrospective (RWR) Study of PUL, retrospective chart review of PUL procedures was conducted across 22 sites in the United States, Australia, and the United Kingdom between July 2017 and March 2020. Consecutive PUL cases following market clearance were included in the database totaling a number of 3226 patients. The presence of an obstructing median lobe was based on physician cystoscopic assessment during the procedure.
Comparative study assessments
MedLift CCT PUL outcomes vs RCT controls
The following MedLift CCT (n = 45) outcomes were compared with those of RCT control procedures (sham: n = 66; TURP: n = 35) at 1, 3, 6, 12, and 24 months: International Prostate Symptoms Score (IPSS), quality of life (QoL), Qmax, postvoid residual (PVR), patient satisfaction (rating postprocedural condition as very much better, much better, a little better, no change, a little worse, much worse, or very much worse), catheterization, surgical retreatment, adverse events (including serious adverse events), and sexual function (Benign Prostatic Hyperplasia Impact Index, Sexual Health Inventory for Men, Men's Sexual Health Questionnaire Ejaculatory Dysfunction/Bother). Mean change and percent change from baseline were compared using t-tests and 95% confidence intervals (CI); unpaired t-tests were used to compare absolute symptom scores and Fisher's exact test was performed to assess adverse event and catheterization rates. It should be noted that the sham and TURP arm patients did not have median lobes, however. Standard deviations between MedLift and BPH6 were reviewed and determined to provide statistical weight in pairwise comparison to permit appropriate statistical comparisons.
MedLift CCT outcomes vs RWR study
MedLift results were compared with those of two subgroups in the RWR study: RWR OML and RWR LL patients. After filtering for baseline IPSS, Qmax, PVR, prostate volume, and no previous BPH procedures to mirror MedLift and L.I.F.T. enrollment criteria, 180 of 244 OML and 1279 of 1834 LL total RWR subjects were used in the comparative assessments, respectively. Effectiveness was evaluated by comparing IPSS, QoL, Qmax, and PVR at baseline and at 1-, 3-, 6-, 12-, and 24-month post-PUL. Mean change and percentage change from baseline were compared using paired t-tests and 95% CIs. Absolute symptom scores were compared between groups using unpaired t-test; adverse event and catheterization rates were analyzed using chi-squared and Fisher's exact test when appropriate. Analyzed cohorts were statistically powered to allow for comparative analysis.
Results
PUL for OML in controlled trials
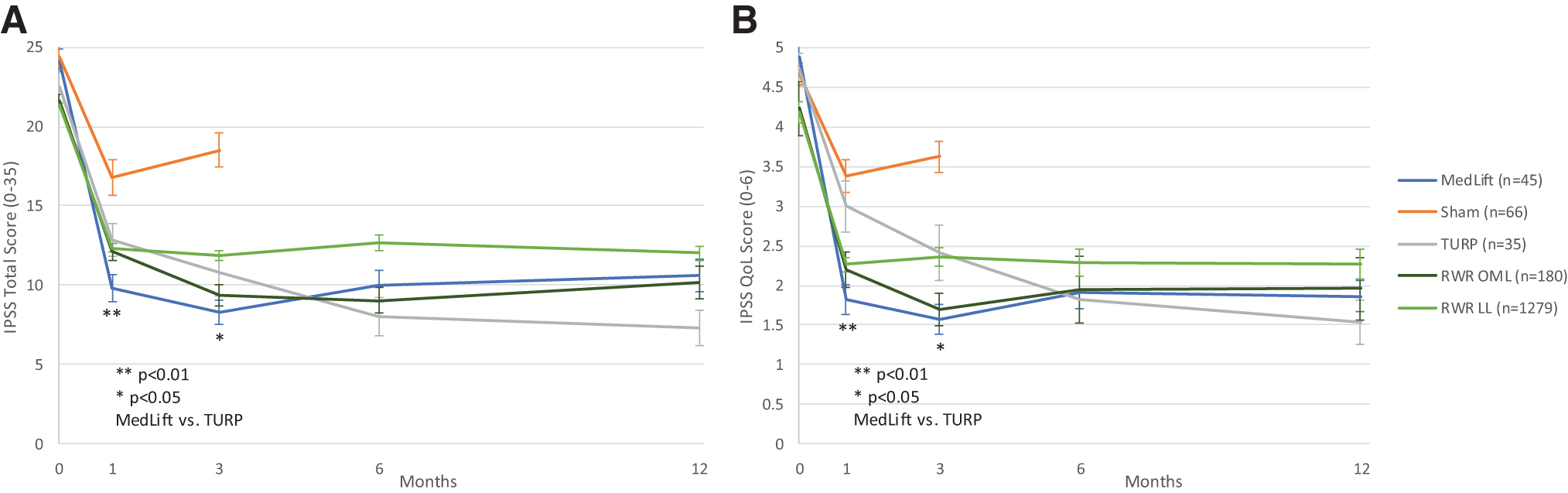
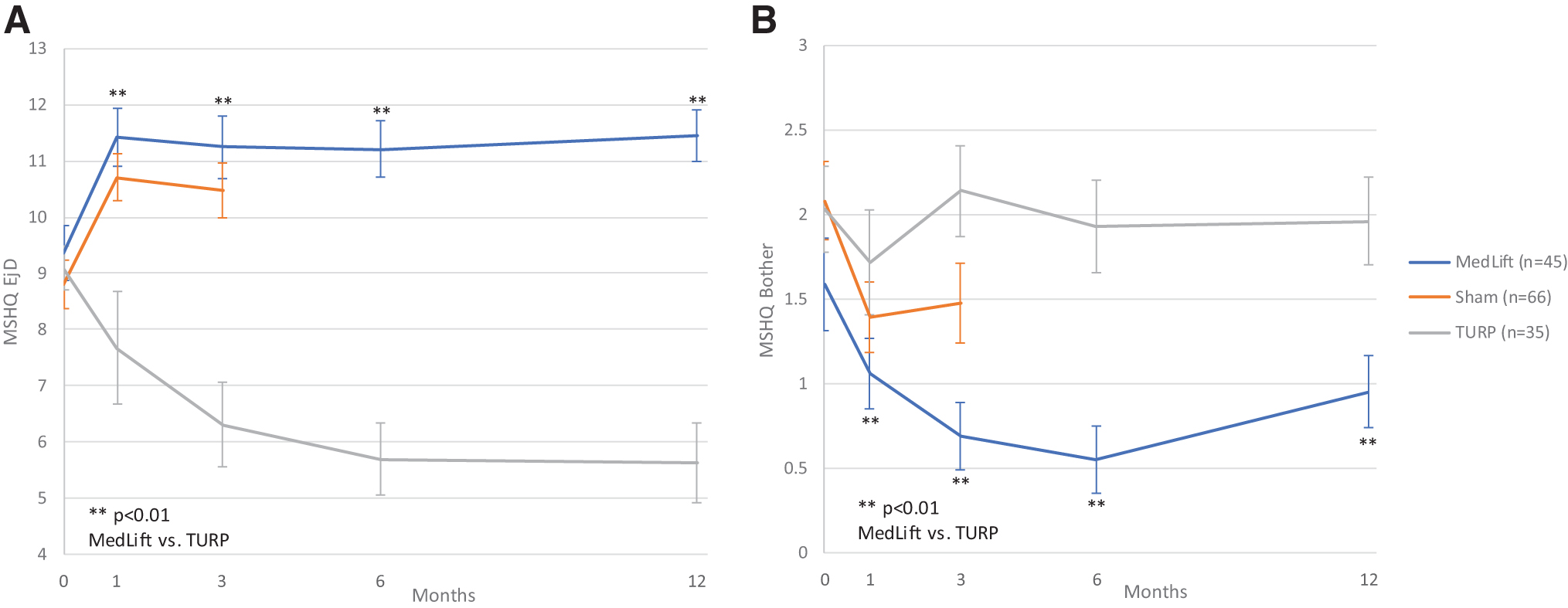
Baseline demographics were similar in all compared groups (Table 2). Statistical difference was only seen for baseline Qmax in TURP control and MedLift subjects (Table 2). At 3 months, MedLift subjects experienced 170% greater IPSS improvement than sham control subjects and significantly better QoL, Qmax, and benign prostatic hyperplasia impact index (BPHII) outcomes (Table 3 and Fig. 2A,B). MedLift IPSS and QoL were significantly improved compared with TURP controls at 1 and 3 months postprocedure and were equivalent at 6 and 12 months. There were no differences in percent change in Qmax and BPHII and change in PVR and Sexual Health Inventory for Men (SHIM) scores between MedLift and TURP at 12 months posttreatment (Tables 3 and 5). MedLift ejaculatory function scores were significantly better than TURP at all time points after PUL (Table 5 and Fig. 3A,B). A significantly higher percentage of MedLift patients described their postprocedural condition as ‘better than baseline’ vs TURP after 1 and 3 months, which was then similar at 6 and 12 months postprocedure (Fig. 4).
Ejaculatory function
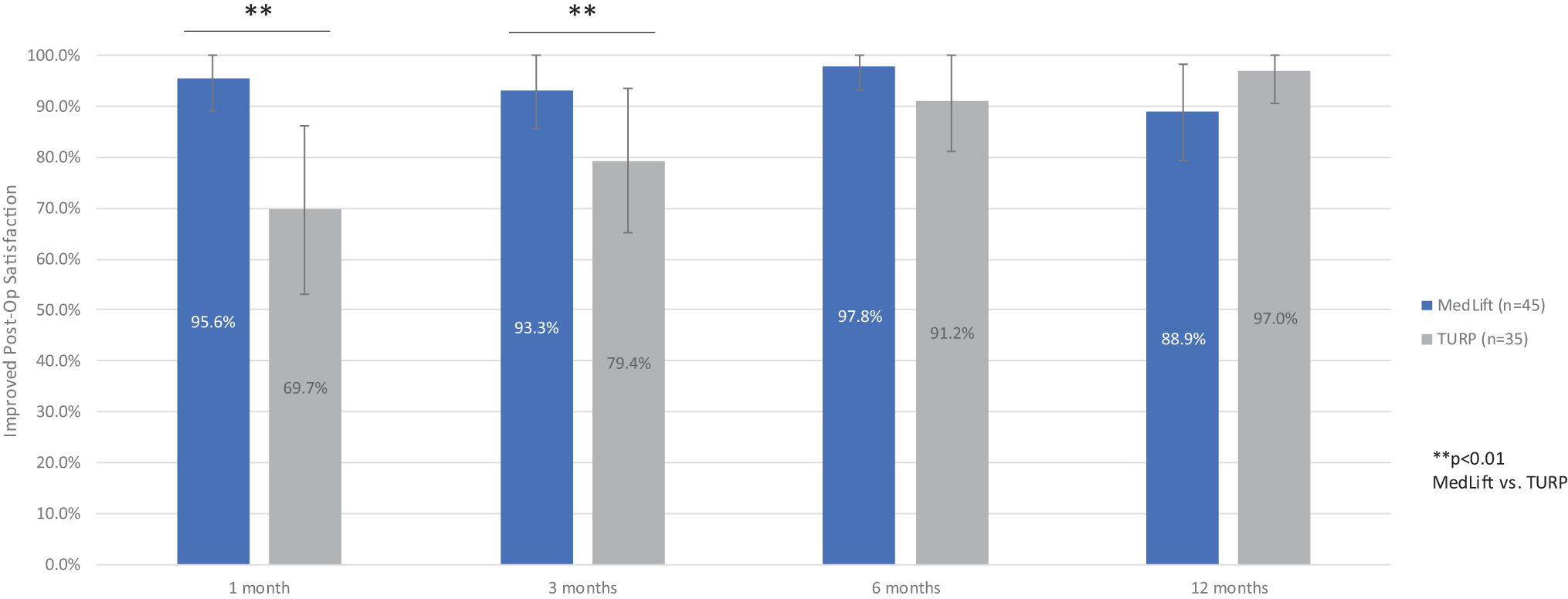
Postprocedural satisfaction scores following treatment with PUL or TURP in controlled studies of PUL.
Baseline Demographics of Patients Used for the Comparative Analysis
RCT and CCT Outcomes over 12 Months After Treatment with Prostatic Urethral Lift, Sham, and Transurethral Resection of the Prostate
RCT = randomized controlled trial; CCT = controlled clinical trial.
Real-World Outcomes over 12 Months Following Treatment with Prostatic Urethral Lift
Sexual Function and Satisfaction Outcomes over 12 Months Following Treatment with Prostatic Urethral Lift
Expectedly, MedLift patients experienced more adverse events (30.3% vs 88.9%, p < 0.01) and higher rates of postprocedural catheterization (for subjects who failed voiding trials: 15.6% vs 3.0%, p < 0.01) compared with sham subjects. As previously published, perioperative adverse events were typically mild to moderate and transient and mean catheter duration was 1.2 days averaged over the total cohort. 10 Compared with patients who underwent TURP, MedLift subjects experienced no high-severity adverse events (AEs) (0.0% vs 14.3%, p < 0.01), whereas five TURP patients reported serious AEs (blood clot in urine, urge incontinence, urethral stricture, bladder tamponade, and weak urinary stream); MedLift patients also experienced shorter catheter durations in comparison to TURP (1.24 days vs 2.2 days, p = 0.01). Retreatment rates were similar between MedLift and TURP patients (2.2% vs 5.7%, p = 0.4155).
PUL for OML in large-scale retrospective study confirms control trials
PUL outcomes for treating OML were equivalent to those for treating LL in the RWR study. At baseline, RWR OML and LL groups were equivalent in terms of IPSS, QoL, Qmax, and age. Postprocedure IPSS, QoL, Qmax, and PVR were similar at 1, 6, and 12 months (Table 4). Overall AEs and nonstandard of care catheterization rates were also similar between RWR OML and LL groups.
Compared with the filtered RWR OML subjects, MedLift patients were younger and more symptomatic at baseline while baseline body mass index and prostate specific antigen (PSA) were equivalent (Table 2). Although the filtered RWR OML group retained significant baseline differences in comparison to MedLift, the cohorts were as closely matched as possible to include patients at 6- and 12-month time points from which to make meaningful comparisons.
Post-PUL, percent change IPSS, QoL, PVR, and Qmax were equivalent between MedLift and the filtered RWR OML group at 3, 6, and 12 months (Table 3 and Fig. 2A,B). Collectively, MedLift, RWR OML, and RWR LL subjects had similar catheter-free rates (20% vs 33.9% and 62.1%, p = 0.07) and RWR cohorts did not experience higher rates of overall AEs (66.7% vs 29.4% and 31.3%).
Discussion
Median lobe obstruction has been estimated to occur in up to 20% of men diagnosed with BPH, although in the L.I.F.T. RCT only 5.3% subjects were excluded due to median lobe obstruction. 10 –13 Although this type of obstruction may not affect most BPH patients, population-based studies have shown that an OML can pose an increased risk for progression of clinical BPH and bladder outlet obstruction, prompting the inclusion of diagnostic morphology assessments in AUA guidelines. 6,14,15 In general, watchful waiting and most BPH medical therapies are less effective at treating patients with OML, often necessitating surgical intervention. 17 –20 As such, the access to minimally invasive surgical options for this patient population is particularly pertinent.
The utility of PUL in treating OML was first demonstrated in the MedLift CCT, where median lobe patients were enrolled using the L.I.F.T. trial criteria to approximate LL patients in the L.I.F.T. RCT. In the MedLift CCT, no significant difference was seen at 1 year between OML and LL outcomes. Notably, PUL efficacy in patients with OML was independent of intravesical prostatic protrusion (IPP) severity at baseline (p = 0.7). 10,16 This independence is likely due to median lobe displacement during PUL, changing the angle of bladder neck obstruction and preventing the median lobe from acting as a “ball valve” into the prostatic fossa. Durability is likely associated with displacement and the resulting ischemia, atrophy, and scarring that occurs postimplantation. 5,21
In the current analysis, we find that PUL for OML indeed outperforms matched sham controls without OML in terms of symptom relief, QoL, and flow rate, while showing no relative negative change in sexual function. As one would expect, there was a higher postoperative catheterization rate for OML PUL, but as with LL patients the typical catheter duration was ∼1 day. At the 3-month comparator endpoint PUL for OML was more effective than sham and somewhat more effective in symptom relief and flow improvement than with LL. This is likely due to the dramatic effect displacement, regardless of IPP, can have on outcomes. Although the MedLift and BPH6 studies utilized different criteria scales to assess adverse events (CTCAE and Clavien–Dindo, respectively) a strength of PUL was that no patient experienced a high-severity AE compared with TURP (i.e., CTCAE grade 3 vs Clavien–Dindo 3b). Furthermore, as expected, the adverse event rate in MedLift was higher than sham, lower than TURP, and commensurate with other MISTs. 22 –24
Comparing PUL for OML with TURP provides interesting insights. TURP, being a full cavitation of the prostatic fossa, generates higher flow rates, but it is interesting that the high flow did not translate into greater QoL. The trajectory of symptom improvement and patient satisfaction over the first year is particularly meaningful. PUL for OML patients improve and indeed are largely satisfied by 1 month, while TURP patients only catch up to the PUL patients by 6 to 12 months, showing no difference thereafter. Erectile function was maintained in both groups. While not surprising for PUL, the lack of degradation that was seen following TURP was perhaps due to rigorous baseline sexual function screening, TURP technique, or insufficient sample size to detect a low-level occurrence. Ejaculatory function is maintained for PUL patients, which is a marked difference to TURP. While TURP efficacy remains a gold standard for BPH, the considerably more rapid improvement, easier postoperative recovery, and preservation of ejaculatory function are likely important factors in OML men choosing PUL as a therapeutic choice.
The RWR study of PUL outcomes is the largest, most comprehensive investigation of a MIST for BPH. This comparative analysis expands on previously published clinical trial results demonstrating PUL's safety and efficacy in BPH subjects with OMLs. In this study, OML patients constituted 11.7% (244/2078). Patients treated with PUL outside of controlled trials appear to be modestly less symptomatic than in the typical controlled trial, which sets a minimum baseline IPSS at 13. 7,22,25 Although published analyses of the RWR database have found the patients to be less symptomatic at baseline, 25 when the database was filtered using MedLift enrollment criteria, a MedLift-like cohort emerged with mostly consistent baseline variables on which to build comparisons, strengthening the analytical approach. Despite the IPP measurement not widely available for extraction as part of the retrospective real-world database, it is encouraging that symptom improvement in the real-world largely reflected results from the controlled MedLift study. One can deduce that with over 200 real-world OML patients in the database, IPP and OML anatomical variability existed, however additional investigation in this arena will further aid patient selection.
Outcomes for PUL treating OML were largely equivalent in CCT and real-world studies, with similar percent improvement in IPSS, QoL, and Qmax scores through 12 months. Catheterization rates and duration were also comparable. Mild-to-moderate adverse events are more prevalent in the CCT, which could be a result of closer scrutiny of a controlled study follow-up or a reflection of refined technique with more experience. While large-scale real-world clinical data are not considered by many academic guidelines, it nonetheless presents an important test as to whether a treatment performs in the real world as well as it performed in highly controlled clinical studies. The data from over 3000 patients across myriad sites indeed indicate that PUL is as effective in treating OML and LL disease in the ambulatory setting as it was shown to be in controlled studies.
Although this study draws conclusions from patient populations across nonconcomitant studies, the trials pooled for this comparative analysis encompass PUL treatment spanning 2011 through 2019. A critical foundation of this analysis was that baseline demographics were similar for RCT and CCT groups, except for baseline Qmax, which was higher for TURP controls vs MedLift subjects. To date, PUL is the most well-studied MIST for BPH. The ability to evaluate results across multiple clinical controlled studies (including two RCTs) and compare results to a large real-world study is a key strength of the technology.
Conclusion
In this first detailed analysis of patients with OML treated with PUL in CCT and real-world settings compared with subjects treated with TURP or sham in RCTs not selecting for men with OML, we show that PUL is superior to TURP within the first 3 months following treatment, with better symptom improvement and patient experience and no serious adverse events. Outcomes from the large RWR study of PUL further support the effectiveness of the procedure, demonstrating similar symptom improvement and catheter-free rates with no elevation in overall adverse event rates in the real-world setting.
The clinical value of this study is achieved through total access to a large database of outcomes from industry-sponsored studies. By comparing results from randomized, clinical controlled, and large real-world studies, we were able to achieve a robust view of the safety and effectiveness of PUL in treating OML and LL obstruction. While academic guidelines often limit their analyses to early randomized studies for regulatory approval, we believe there is important information to be gleaned from comparing these results to present-day results in our clinics. This analysis supports the use of the PUL for treatment of BPH in prostates with or without OMLs.
Footnotes
Authors' Contributions
All authors were investigators on the PUL feasibility clinical trial (Drs. Roehrborn and Rukstalis were investigators on the pivotal L.I.F.T. study, Drs. Rukstalis and Eure were investigators on the MedLift trial, and Dr. Eure is an investigator on the Real-World Retrospective study). All authors had access to clinical data and contributed to the study concept and design, analysis, and interpretation of results, and critical review of the article for important intellectual content.
Acknowledgments
The authors would like to thank Margaret Mariella, MD; Theodore Lamson, PhD; and Jacqueline Nerney Welch, MD, PhD for their support in the preparation of this article.
Author Disclosure Statement
Drs. Eure, Roehrborn, and Rukstalis are NeoTract, Inc./Teleflex consultants.
Funding Information
The study was sponsored by NeoTract Inc./Teleflex. The sponsor played a role in the collection, management, and analysis of data, as well as in article preparation and review.