
Abstract
Recent decades have seen the rapid progression of minimally invasive surgery in urology with continuing developments in robotic technology paving ways into a new era. In addition to these technological innovations, interests from urologists in developing and embracing new techniques have become a forefront in the ongoing evolution of the field allowing for improvement in intraoperative experience as well as morbidity and mortality outcomes. This article aims to provide an overview of the historical development of laparoscopic surgery in urology while also providing a brief look into its future.
Introduction
The introduction of robotic laparoscopic surgery has changed the landscape of urologic surgery. With increasing utility of robotic and laparoscopic approaches encompassing most of urologic surgeries, the scope of open urologic surgeries has reduced significantly and now only limited to certain clinical conditions. This article aims to provide a brief overview of the historical development of laparoscopy in urology (Table 1).
Summary of Some of the Important Milestones of Laparoscopic Surgery in Urology from Its First Application to the Development of Robot-Assisted Laparoscopic Techniques
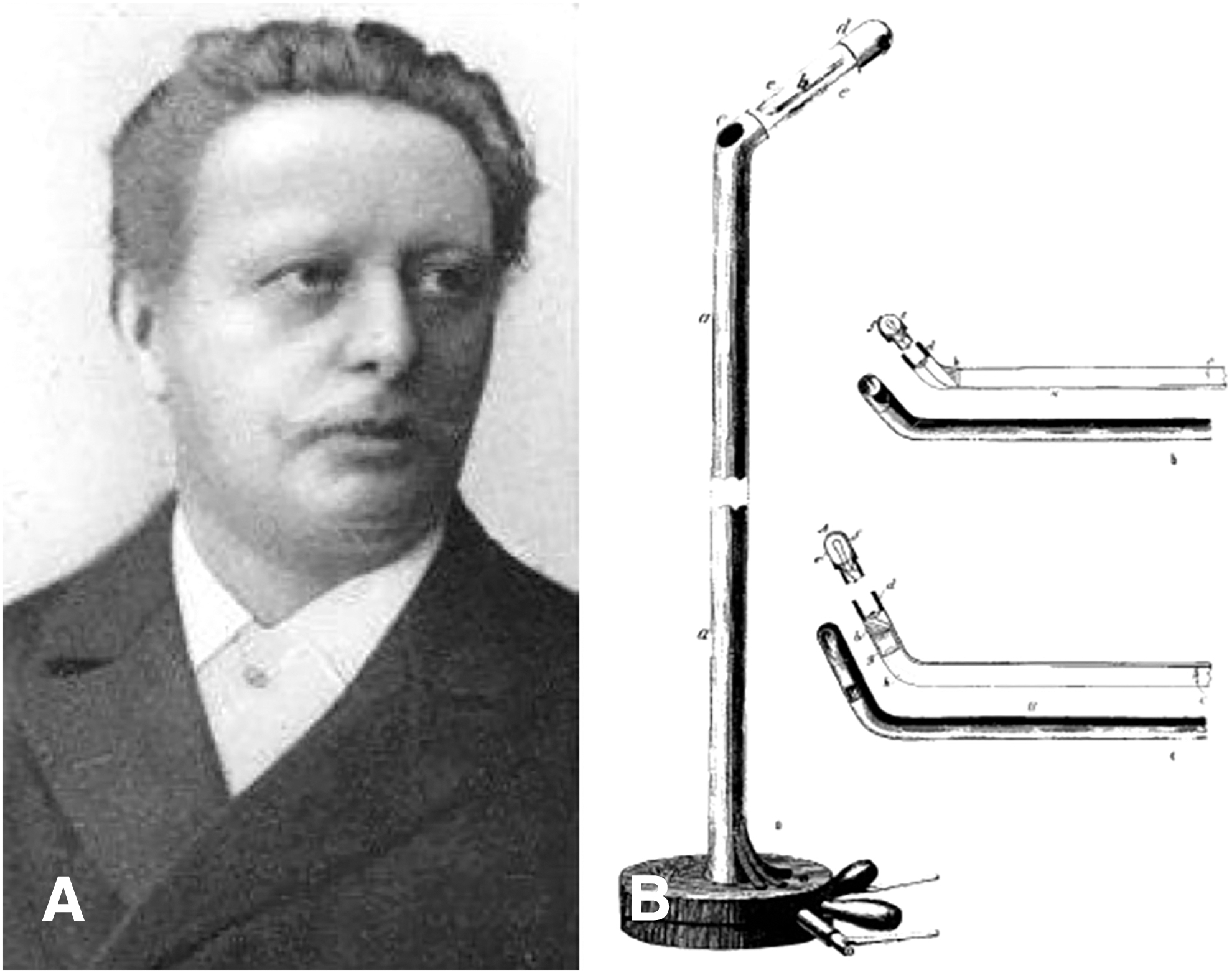
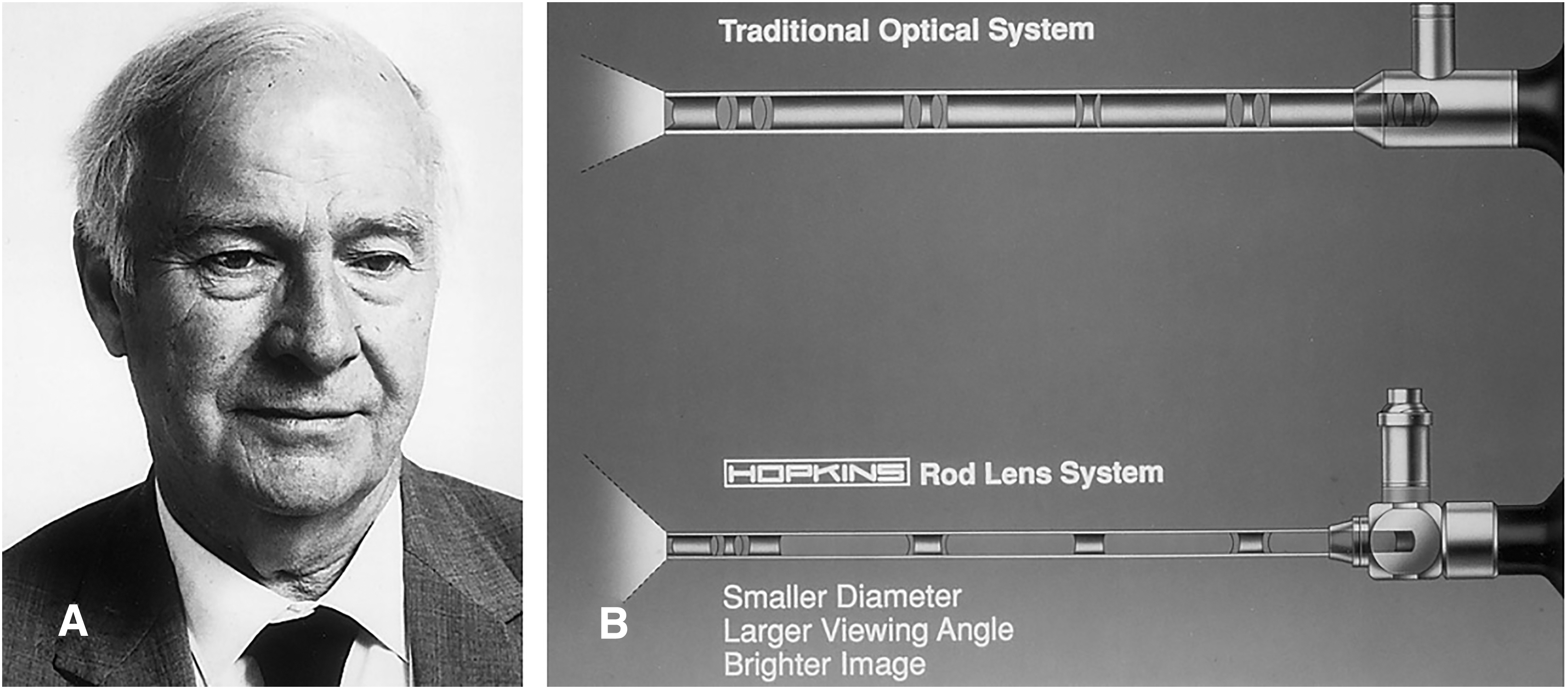
The beginning of laparoscopy can be traced back to early 19th century when Philip Bozzini, an obstetrician, used the first candle-lit endoscope to perform inspections of the urethra, bladder, and rectum. The device was later adapted by Antonin Desormeaux in 1853 with the addition of a concave mirror and turpentine and alcohol-based lamp to improve observation. The light source was further improved by Julius Bruck in 1867 who applied the first electrical light source using heated platinum wire, which was applied to the first rigid cystoscope used by German Urologist Maximilian Nitze in 1879 (Fig. 1) and later became the foundation of Harold Hopkins's rod-lens system developed by Storz (Fig. 2). 1 –3
Nitze's cystoscope subsequently became the critical instrument in George Kelling's laparoscopic examination of an insufflated abdomen in 1901. The same year also saw Hans Christian Jacobaeous publishing the first case series of abdominal diagnostic laparoscopy, mostly involving patients with ascites and without use of pneumoperitoneum. The first therapeutic application of laparoscopy was introduced by Karl Fervers in 1933, who performed laparoscopic liver biopsies and adhesiolysis.
Since then, increasing popularity of laparoscopy can be credited to critical innovations in the likes of oblique-viewing telescopes and additional operating ports by Heinz Kalk in 1929, insufflation needle by Janos Veres in 1938, and large variety of laparoscopic instruments and techniques, such as extracorporeal and intracorporeal suturing, the first laparoscopic appendicectomy as well as the first laparoscopic cholecystectomy by Kurt Semm. 2,4
History of Laparoscopic Urology Surgeries
Beginning of laparoscopy in urology
The first laparoscopic application in urology was reported by Nicola Cortesi in 1976 for the localization of bilateral abdominal cryptorchidism in an 18-year-old patient. 5 Transition to therapeutic application for management of undescended testes was initiated by David Bloom who performed the first laparoscopic orchiopexy in 1991 based on a two-step Fowler–Stephen approach with initial ligation of spermatic vessels. 6 The technique was further modified by Gerald Jordan and Boyd Winslow in 1994 who truncated the aforementioned procedure into a single stage laparoscopic orchiopexy. 7
Further use was introduced by Tage Hald and Finn Rasmussen in 1980 and later by William Scheussler in 1991 who performed endoscopic lymph node biopsies for better staging of urologic malignancies through extraperitoneal and transperitoneal approach, respectively. 8,9
Laparoscopic nephrectomy and nephroureterectomy
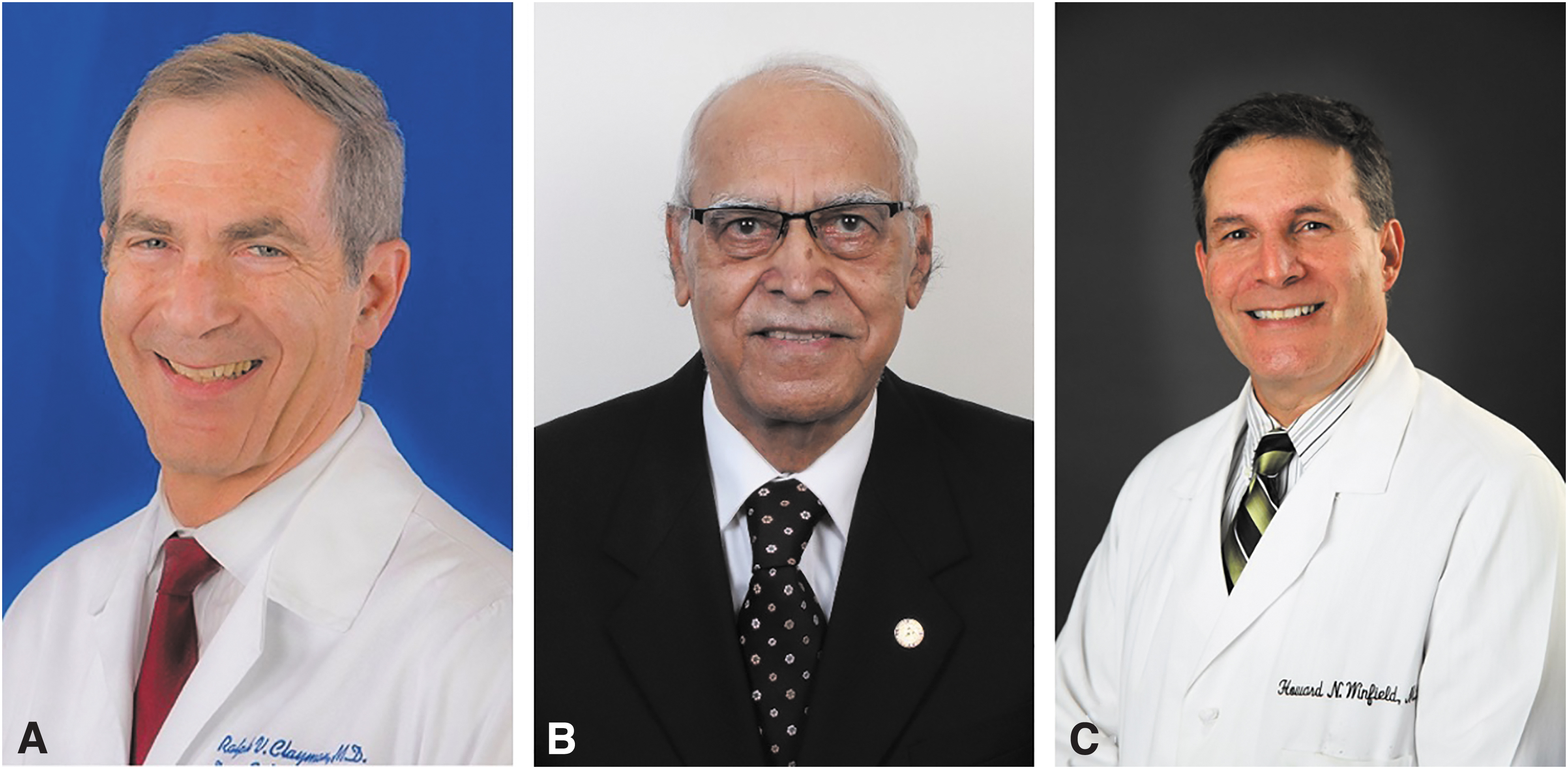
The year 1991 also saw the first laparoscopic renal surgery with radical nephrectomy performed by Ralph Clayman (Fig. 3) on an 85-year-old woman with incidentally found 3 cm right midpole renal mass, later reported as grade I oncocytoma. Clayman adopted a transperitoneal approach for his dissection with the patient placed in a lateral decubitus position and with renal artery embolization and ureteral catheter insertion performed prior. 10 Similar approach was replicated later in the year by Clayman as he proceeded for laparoscopic nephroureterectomy for an 82-year-old man with low-grade transitional cell carcinoma of the renal pelvis. 11
In a later publication, Clayman's group highlighted their experience with laparoscopic nephrectomy over 9 years, and comparing with the conventional open approach, they highlighted significant reduction in operating time and intraoperative blood loss, while maintaining satisfactory oncologic outcomes and proving the benefits of laparoscopic technique in improving convalescence, reducing postoperative analgesia requirements, and duration of inpatient stay. 12 Subsequent larger studies comparing laparoscopic and open nephroureterectomies for upper tract urothelial carcinoma also demonstrated comparable results with similar operating time, reduced intraoperative blood loss, and comparable cancer-free survival. 13,14
Considering the retroperitoneal location of the kidney and building on earlier studies by John Wickham, D.D. Gaur (Fig. 3) conceptualized a different approach for laparoscopic nephrectomy through retroperitoneal dissection. 15 Appreciating previous concerns surrounding fibrofatty retroperitoneal tissues and potentially limited working space, Gaur's 1991 report included the novel retroperitoneal dissecting balloon inserted through a 2 cm midaxillary line incision above the iliac crest, which was initially developed from a step-wise insufflation of a surgeon's glove. 16
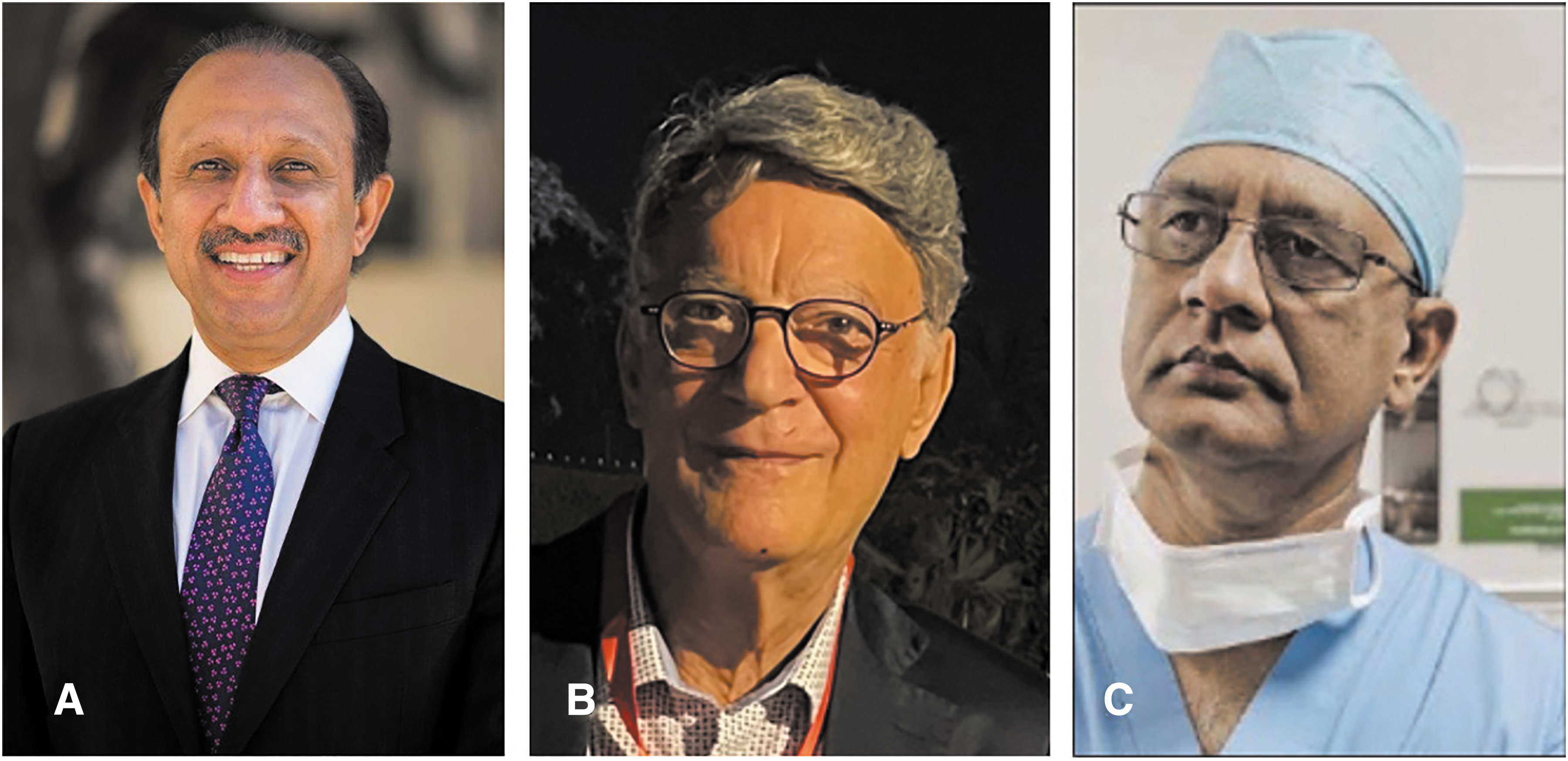
A later study by Inderbir Gill (Fig. 4) in 1994 involving larger cohort of patients confirmed the feasibility and benefits of the technique, allowing for a more direct entry, quicker dissection, yet without much compromise on working space and dimension of excised specimen. 17
Further technical innovation was proposed by Stephen Nakada in 1997 who conducted the first hand-assisted laparoscopic transperitoneal radical nephrectomy on a 60-year-old woman with recurrent pyelonephritis secondary to recurrent calculous disease of the right kidney. Nakada took advantage of the recently developed PneumoSleeve® device by Bannenberg et al. applied through a vertical supraumbilical incision, which allowed surgeon's hand to be inserted into the intraperitoneal working space through an airlock without compromising the established pneumoperitoneum. The benefits of this technique relied on the tactile and flexibility of the hand itself, allowing for better organ retractions and manipulations, as well as assisting working laparoscopic instruments. 18
A different application of laparoscopic nephrectomy was introduced by Lloyd Ratner and Louis Kavoussi in 1995 who performed the first live donor nephrectomy from a 40-year-old man to his sister. With the patient in lateral decubitus position, transperitoneal dissection was performed to free the donor kidney attachments and ureter to the level of iliac bifurcation. With renal artery and veins transected and ligated with surgical clips, donor kidney was then removed and flushed with iced solution. Total warm ischemia time was limited to <5 minutes. 19
Laparoscopic partial nephrectomy
One year after Clayman's laparoscopic nephrectomy, the first laparoscopic partial nephrectomy was attempted by Howard Winfield (Fig. 3) on a 35-year-old woman with recurrent urinary tract infections secondary to a refractory lower pole renal calculus situated in a caliceal diverticulum. Transperitoneal dissection was opted after ureteral catheter insertion and patient positioning in a reverse Trendelenburg position. Specially designed adjustable renal torniquet was then applied on the lower half of kidney, which was followed by resection using electrosurgical blade and argon beam coagulator. 20 After their earlier study on laparoscopic retroperitoneal nephrectomies, Inderbir Gill (Fig. 4) attempted the first laparoscopic retroperitoneal partial nephrectomy in 1994.
The surgery was performed on a 24-year-old woman with right lower pole calculus not amendable to extracorporeal shock wave lithotripsy. Different to Winfield's, Gill adopted a retroperitoneal approach based on earlier studies on retroperitoneal nephrectomy and a double loop sling was used in place of the aforementioned torniquet. The sling possessed a superior loop to stabilize and an inferior loop to facilitate hemostasis. Incision of renal parenchyma was done caudal to the lower loop using electrosurgical scissors and argon beam coagulator. 17
Despite initial success of partial nephrectomies, as further popularized by Inderbir Gill et al., 21 earlier procedures were often plagued with prolonged operating and ischemia time mostly associated with challenges in hemostasis and parenchymal closure using surgical knots. A technical improvement was proposed by Agarwal et al. in 2007 with the use of sliding-clip fixation approach using Hemolok clips, allowing for faster closure of renal parenchymal defect without laceration and obviating the need for time-consuming conventional knot tying, and thus reducing warm ischemia time. The safety and efficacy of this technique have now been demonstrated in other series, with it now used in various clinical settings across many surgical centers worldwide. 22 –24
Laparoscopic renal pelvis and ureter surgery
The first planned laparoscopic surgery involving the ureter was performed later in 1993 in the form of laparoscopic vesicoureteroplasty by Richard Ehrlich, Alex Gershman, and Gerhard Fuchs. The procedures were performed on two pediatric patients—2-year-old boy with Grade IV left vesicoureteral reflux and a 5-year-old girl with Grade III left vesicoureteral reflux. Ureterovesical anastomoses were constructed following the Lich–Gregoir technique. 25
With increasing interests for laparoscopic surgery in urology, 1993 saw the addition of laparoscopic pyeloplasty for ureteropelvic junction obstruction to the growing list of therapeutic indications. Introduced by Louis Kavoussi and Craig Peters, the procedure was performed on a 24-year-old woman with evident right ureteropelvic junction obstruction secondary to crossing vessel on intravenous pyelogram. With patient placed in left lateral decubitus position, dissections were performed to expose the right renal pelvis, which was kinked between the lower pole renal artery anteriorly and vein posteriorly.
Following the steps of Anderson–Hynes dismembered pyeloplasty, ureter was transected just distal to the ureteropelvic junction and brought anterior to both vessels. Ureteral anastomosis was formed using intracorporeal interrupted sutures over the stent. Ureteral stent was removed 2 weeks after the procedure after ensuring absence of urine leak and patent anastomosis. 26 Appreciating the varying techniques of pyeloplasty, later study by Thomas Jarrett and colleagues in 2002 highlighted the feasibility of adopting laparoscopic technique across the different repair techniques, including Anderson–Hynes, Y-V plasty, Heineke–Mirhulicz, and Davis intubated ureterotomy. 27
Laparoscopic prostate surgery
William Schuessler performed the first laparoscopic radical prostatectomy (LRP) in 1991. The procedure was performed through transperitoneal approach. Foley catheter was used to assist in both dissections and to create the vesicourethral anastomosis. The latter was formed by first creating a transverse incision through the bladder dome and reconstructing the bladder neck over Foley catheter with interrupted intracorporeal suture knots. 28 Despite the initial success with good oncologic and functional outcomes as reported in his case series, Schuessler argued against the adoption of laparoscopic prostatectomy because of its complexity, especially surrounding vesicourethral anastomosis, yet without additional benefits when compared with the conventional open procedure in terms of acute recovery period, oncologic and functional outcomes. 29
Appreciating the potential benefits and with rising popularity of laparoscopic techniques, Bertrand Guillonneau and Guy Vallancien adopted and modified the technique a few years later. In their 1999 publication of the so-called Montsouris Technique, two critical changes were reported—the “parachute” technique with interrupted sutures for vesicourethral anastomosis without need for transverse incision of the bladder and the introduction of Béniqué metal catheter to improve tactile perception during dissections. 30
Although transperitoneal LRP was initially opted as it conceptually allows for larger working space and better access for subsequent dissections, the technique deviated from the conventional open retropubic prostatectomy as first proposed by Terence Millin in 1946 and then popularized by Patrick Walsh in 1980s. 31 The first LRP adaptation with this retropubic retroperitoneal approach was then attempted by Adley Raboy in 1997. Blunt dissections were first performed to open the extraperitoneal space with placements of five ports—umbilical port, two other midline ports between pubic symphysis and umbilicus, and two lateral ports on each side at two-thirds distance from midline to the iliac spines, in the order.
This was followed by sequence of dissections starting from the endopelvic fascia, puboprostatic ligaments, dorsal venous complex, bladder neck, vas, seminal vesicles, then the lateral prostatic pedicles. The nearly 6-hour procedure yielded good oncologic outcome and return of complete continence but unfortunately without return of spontaneous erection. 32 The technique was later brought back to Institut Montsouris by François Rozet in 2005 who then refined it into the 11 steps known as the “Montsouris II Technique.” 33
When compared with open prostatectomies, larger series found similar oncologic and functional outcomes with multiple additional benefits including reduced intraoperative blood loss, quicker recovery, and reduced risks of early postoperative complications, including paralytic ileus after extraperitoneal LRP. The use of newer device, such as the previously outlined balloon dissector, also allows for reduced operating time and risk of intraoperative bleeding. 34,35
Laparoscopic cystectomy
The year 1992 marked the beginning of the laparoscopic cystectomy era when Mike Kozminski and Krikor Partamian performed the first laparoscopic urinary diversion with adaptation of Bricker's anastomosis on an 83-year-old man with fibrosarcoma of the prostate. Most of the procedure was able to be completed laparoscopically with intermittent adjustments to pneumoperitoneum. EndoGIA and TA-55 stapling devices were used for intracorporeal bowel anastomosis after harvest of ileal segment. Bricker anastomoses of bilateral ureters were performed with intracorporeal suturing over the respective ureteral stents. 36
In the same year, a laparoscopic simple cystectomy was performed by Raul Parra and colleagues on a 27-year-old paraplegic woman with neurogenic bladder. The procedure was performed in two stages with the first being the formation of ileocolonic reservoir with continent stoma and the cystectomy completed 4 months after.
After displacement of reservoir with pneumoperitoneum and aided by laparoscopic stapling device, dissections were performed to first open the perivesical space, followed by dissection along the plane between posterior bladder wall and uterus, ligation and transecting the lateral vascular pedicles, dividing the urethra across the vesicourethral junction, and finally detaching the bladder from the vaginal wall. 37 The technique was subsequently adopted by Eduardo Sánchez de Badajoz for the first laparoscopic radical cystectomy in 1995 for a 64-year-old woman with Grade IV transitional cell carcinoma and later refined by Xavier Cathelineau of Institut Montsouris in 2005. 38,39
Era of Robotic Laparoscopic Surgery
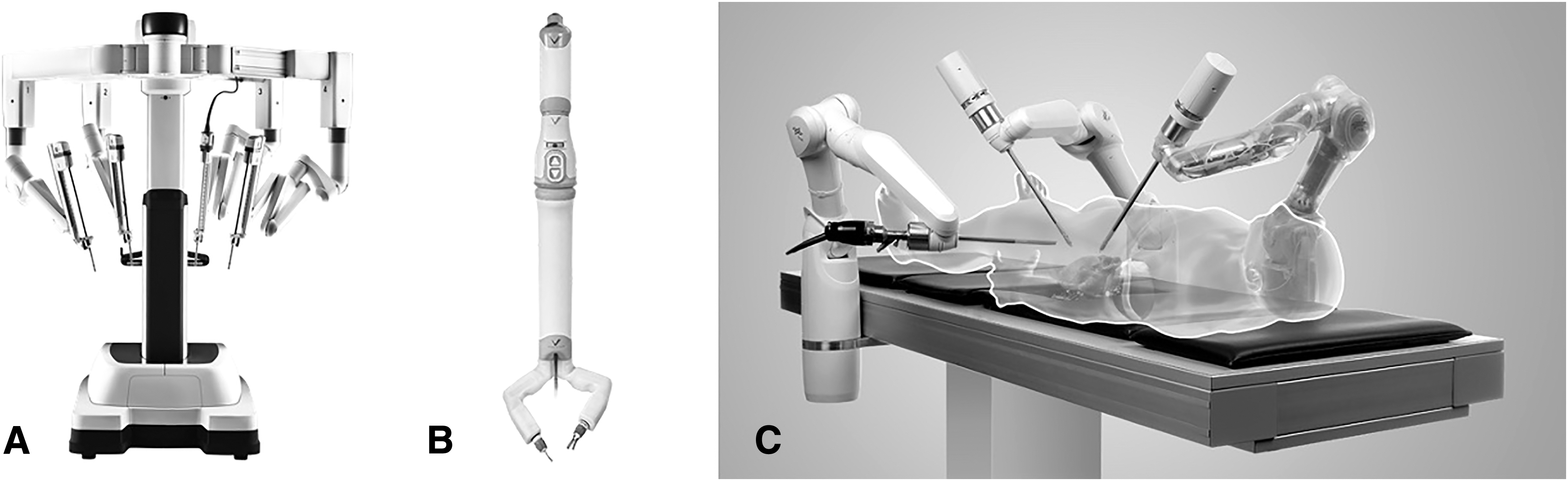
The use of robotic platform has been conceptualized since the late 20th century, allowing for three-dimensional and high-definition vision as well as 360° dexterity. The first use of robotic surgery in urology was introduced by Harris and colleagues in 1997 with the development of “Probot” to assist in transurethral resection of the prostate. However, the first robotic application in urologic laparoscopic surgery began in 2001 after introduction of the Da Vinci system (Fig. 5). 47,48 In its first application by Clément-Claude Abbou (Fig. 4), the Da Vinci system was used to assist in bilateral nerve sparing LRP on a 63-year-old patient with localized T1c prostate cancer. 41
Robot-assisted prostatectomy was further popularized by Mani Menon (Fig. 4) of the Vattikuti Institute and by far remains as the most common urologic procedure done robotically. Larger series have highlighted the benefits of robotic system with improved intraoperative experience and easier learning curve while having comparable intraoperative and postoperative outcomes compared with LRP. 49 The use of robotic system has since been expanded with around 6500 Da Vinci system installed worldwide and now applied for different surgeries including radical cystectomy by Mani Menon in 2003, 42 partial nephrectomy by Matthew Gettman in 2004, 43 and radical nephrectomy by Douglas Klinger in 2005. 44
Future Perspectives
The introduction of robotic technology has opened a new frontier in minimally invasive surgeries in urology. Extending from its current applications, further improvements and innovations have been instituted to enhance surgical outcomes and intraoperative experience. Some of these were inspired by the lost benefits of the conventional open approach, such as the haptic feedback system that has now been reintroduced by Senhance and Versius, which smoothens intraoperative transition and reduces risks of tissue injuries, and the development of da Vinci EndoWrist to mimic the range of motion of the human wrist in the distal effector. 50,51
Some improvements have also been attempted to improve cosmesis by reducing the number of ports. Notable examples included the development of newer technologies, such as GelPOINT advanced access platform, the da Vinci Single-Port system, and Miniature In-vivo Robotic Assistant (Fig. 5), which have since allowed for the development of robot-assisted laparoendoscopic single-site surgery, with the first application being robot-assisted laparoscopic prostatectomy as published by Jihad Kaouk in 2008. 46 Appreciating its feasibility, the technique has now been adopted across different clinical settings, including radical cystectomy with pelvic node dissection by the same group, 52 partial nephrectomy by Joon Chae Na, 53 and Retzius-sparing radical prostatectomy by Deepak Agarwal. 54
In addition to the aforementioned developments, some studies are underway to reduce the overall footprint of the robotic platform and to unlink the instruments from the main control system. Examples of these included the elimination of carts by the MiroSurge system (Fig. 5) and ongoing studies on microbots to adopt a more therapeutic purpose and enabling studies in smaller tissues, such as capillaries and interstitial space. With the original patents for pioneering robotic technologies beginning to expire, we should also expect to see increased market competition, opening further possibilities for better affordability and access, as well as new product research and developments. 55
Footnotes
Authors' Contributions
N.A.S. is the corresponding author and contributed to conceptualization, write up, and editing; B.H.D. carried out conceptualization and editing; M.V.K. was involved in editing; N.M.C. was involved in editing; and D.K.A. carried out conceptualization and editing.
Author Disclosure Statement
The authors declare no competing interest.