
Abstract
Purpose:
Encrusted and knotted stents may cause serious urologic complications. This study aimed to develop a novel and minimally invasive technique to manage encrusted or knotted retained ureteral stents.
Materials and Methods:
This technique was used in nine patients with retained stents. Through rigid cystoscopy, the stents were pulled out of the urinary meatus. The access sheath was modified by cutting the distal end of its obturator. The modified access sheath was advanced over the retained stents in a telescopic manner to remove the encrusted and/or knotted stents.
Results:
Six patients had encrustations, two had knot formation, and one had both encrustation and knot formation. The encrustations were peeled off in the process. The knots were either undone or pulled through the lumen of the access sheath. The retained stents were removed intact from all patients without any complications.
Conclusion:
The access sheath method described in this article provides a simple alternative for the removal of encrusted or knotted retained stents. However, this technique requires further validation to establish its safety and efficacy.
Introduction
Ureteral stents, also known as double-J-stents, have been widely used in urology practice since their first description in 1967. 1 They are commonly used to relieve obstruction of the upper urinary tract. They are also used as an adjunct for various urologic procedures. However, ureteral stents may be associated with complications such as pain, hematuria, infection, encrustation, and, rarely, knot formation in the upper curl within the renal pelvis. 2,3
Encrustations can occur in up to 13% of cases, especially if stents are left for longer periods or forgotten. 4 There are no formal guidelines for the maximum safe indwelling time for ureteral stents with a minimal risk for developing encrustations. The mechanism of encrustations is complex and multifactorial; it includes dwell time, stent composition, patient-specific factors, biofilm formation, and mineral deposition. 5 –9 Encrusted retained ureteral stents are a critical problem if they cannot be removed by a simple cystoscopic procedure.
Depending upon the site and degree of encrustation, these cases may require additional procedures. 10 –18 Similarly, the management of retained knotted stents is a clinical dilemma and may require further endoscopic or percutaneous procedures. 3,19 –26 These additional procedures to remove the retained stents may lead to high morbidity in patients. Up to 16% of endourology lawsuits in the United States are related to retained stents. 27 Thus, there is a requirement for simpler and noninvasive techniques that could remove the retained stents without causing any complications. This article aims to describe a simple and minimally invasive method, using a modified access sheath, to remove the encrusted and/or knotted retained stents.
Materials and Methods
This project received approval from the Royal Melbourne Hospital Human Research Ethics Committee.
Initial preparation
The telescopic access sheath method was used in nine patients with encrusted (Fig. 1) and/or knotted retained stents (Fig. 2). Rigid cystoscopy was performed in the lithotomy position under general anesthesia. The lower curl of the ureteral stent was observed and the distal end of the ureteral stent was grasped and gently pulled out of the urinary meatus. The end of the stent was secured to avoid retraction into the urethra.
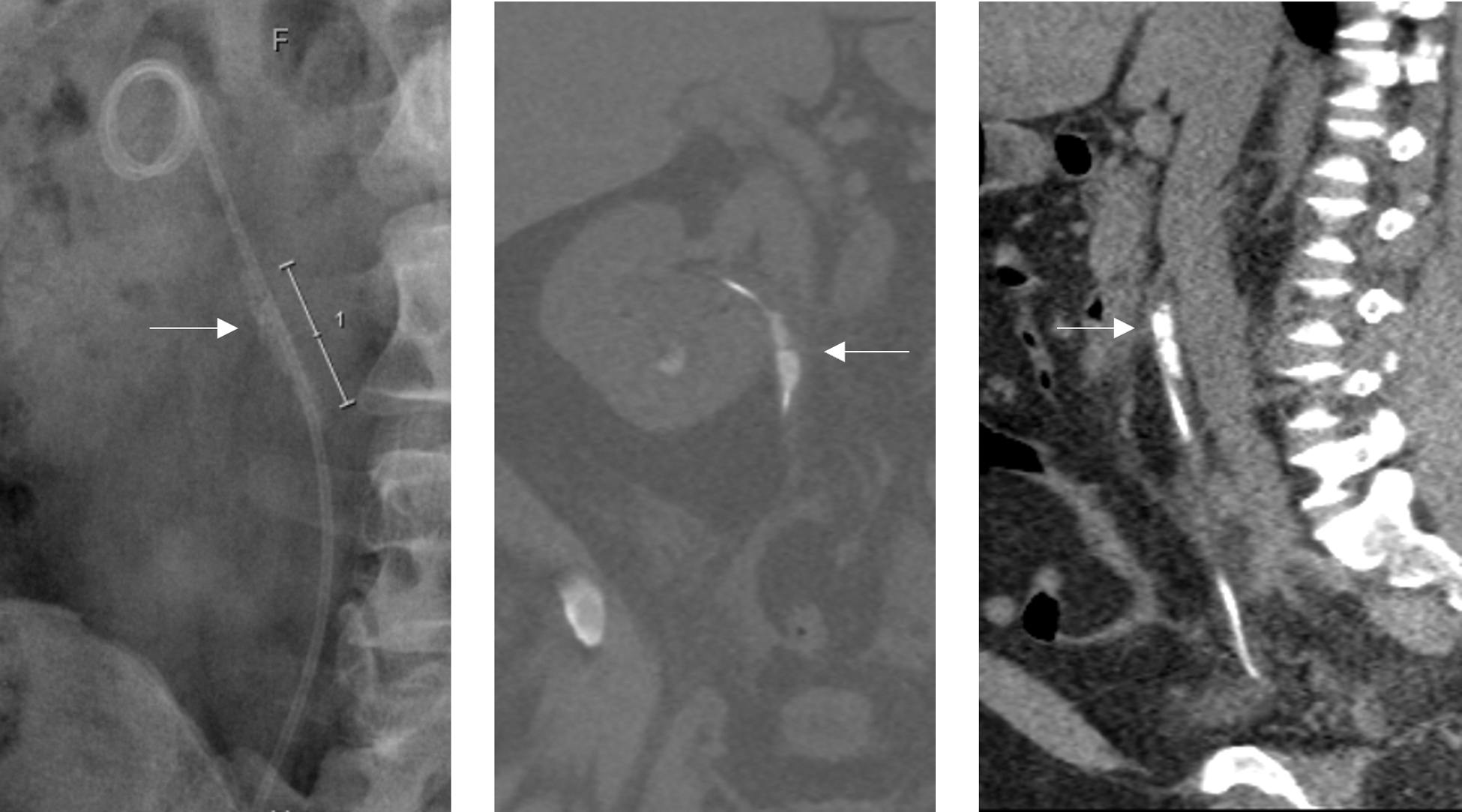
KUB radiograph and CT KUB imaging showing encrustations (indicated by arrow) in the upper part of the ureteral stent. KUB, kidney, ureter, and bladder.
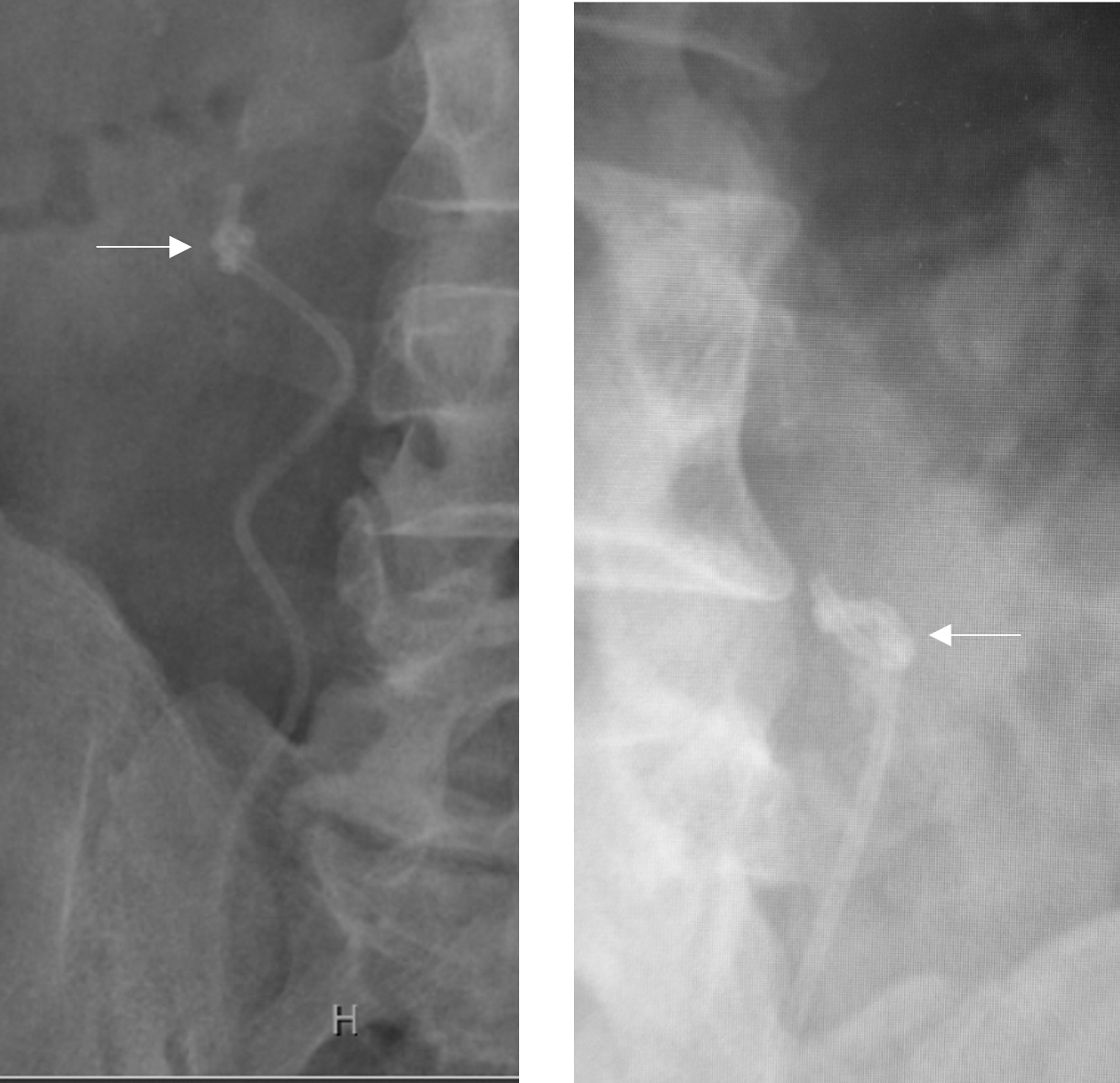
KUB X-ray showing a knot (indicated by arrow) in the upper curl of the ureteral stent.
We used ureteral access sheaths from Applied Medical, US (12F/14F); Boston Scientific, US (13F/15F); and Cook Medical, US (14F/16F). Ureteral access sheaths are commonly used to facilitate the passage of flexible ureteroscopes into the ureter and the upper collecting system. They have two components: an inner tapered obturator and an outer sheath. The lumen of the obturator is not uniform. It is wider proximally and tapered at the tip to accommodate a 0.038 inch (0.97 mm) diameter guidewire. The proximal lumens of the obturators of Applied Medical's (12F/14F), Cook Medical's (14F/16F), and Boston Scientific's (13F/15F) sheaths can accommodate 6F, 7F, and 8F ureteral catheters, respectively.
The tapered end of the obturator was cut with a surgical blade to expose its dilated lumen and to accommodate the distal end of the ureteral stent. This obturator was used with the outer sheath to remove the retained stent. In one patient with an encrusted stent, the obturator was used alone. The technique for removing the retained stents is described in the following sections.
Technique for removing the encrusted stents
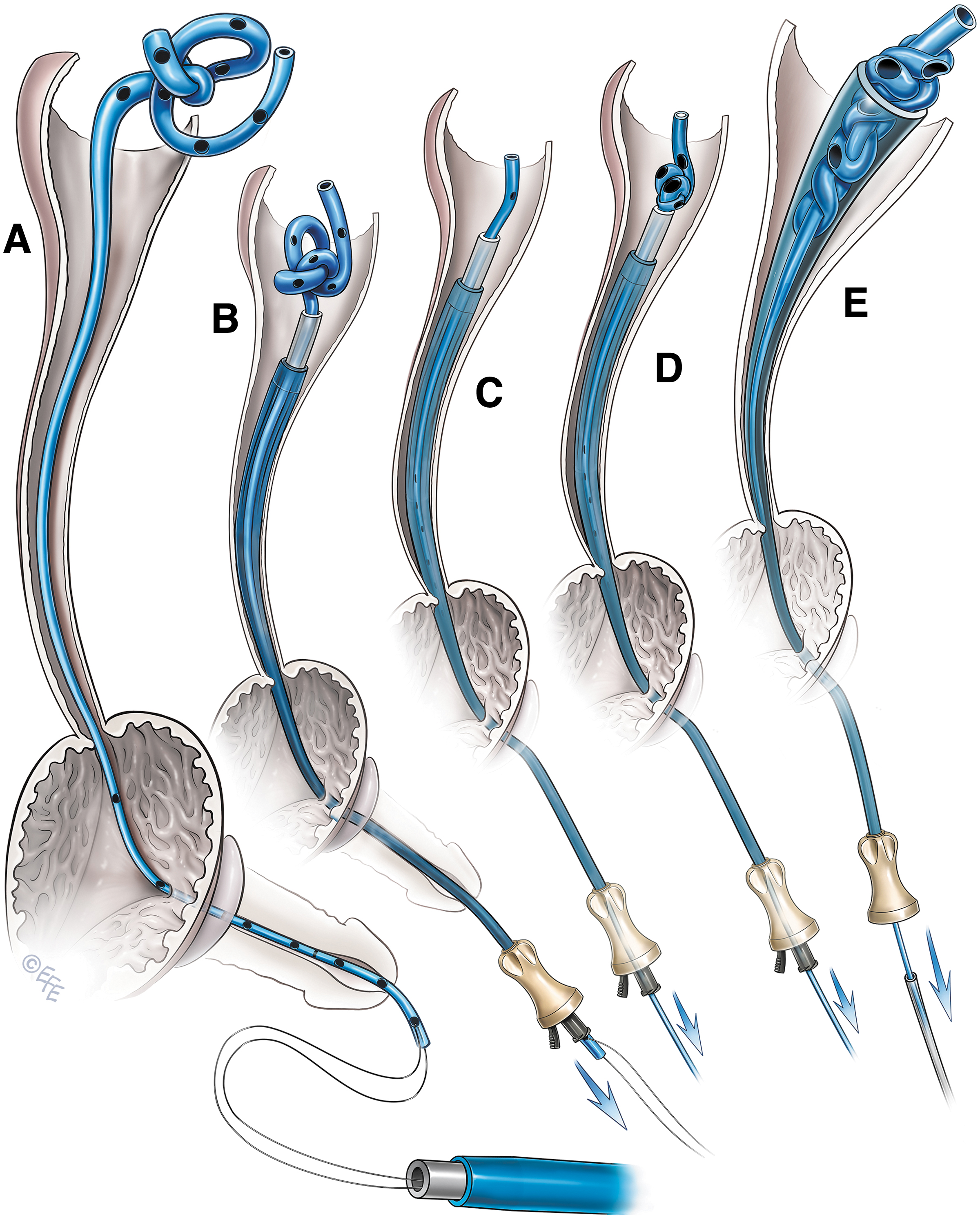
The technique used to remove the encrusted stent is shown in Figure 3. The lower end of the ureteral stent was secured with a 2–0 Prolene suture (SH, 26 mm ½ circle taper needle; Ethicon 8533, US) by passing it through the lowest side hole and the luminal end. This suture was double-armed and 122 cm long with one needle cut before use. After securing the lower end of the stent, another needle was cut. Both the free ends of the suture were fed into the lumen of the obturator of the access sheath and retrieved from the proximal end (Fig. 3A).
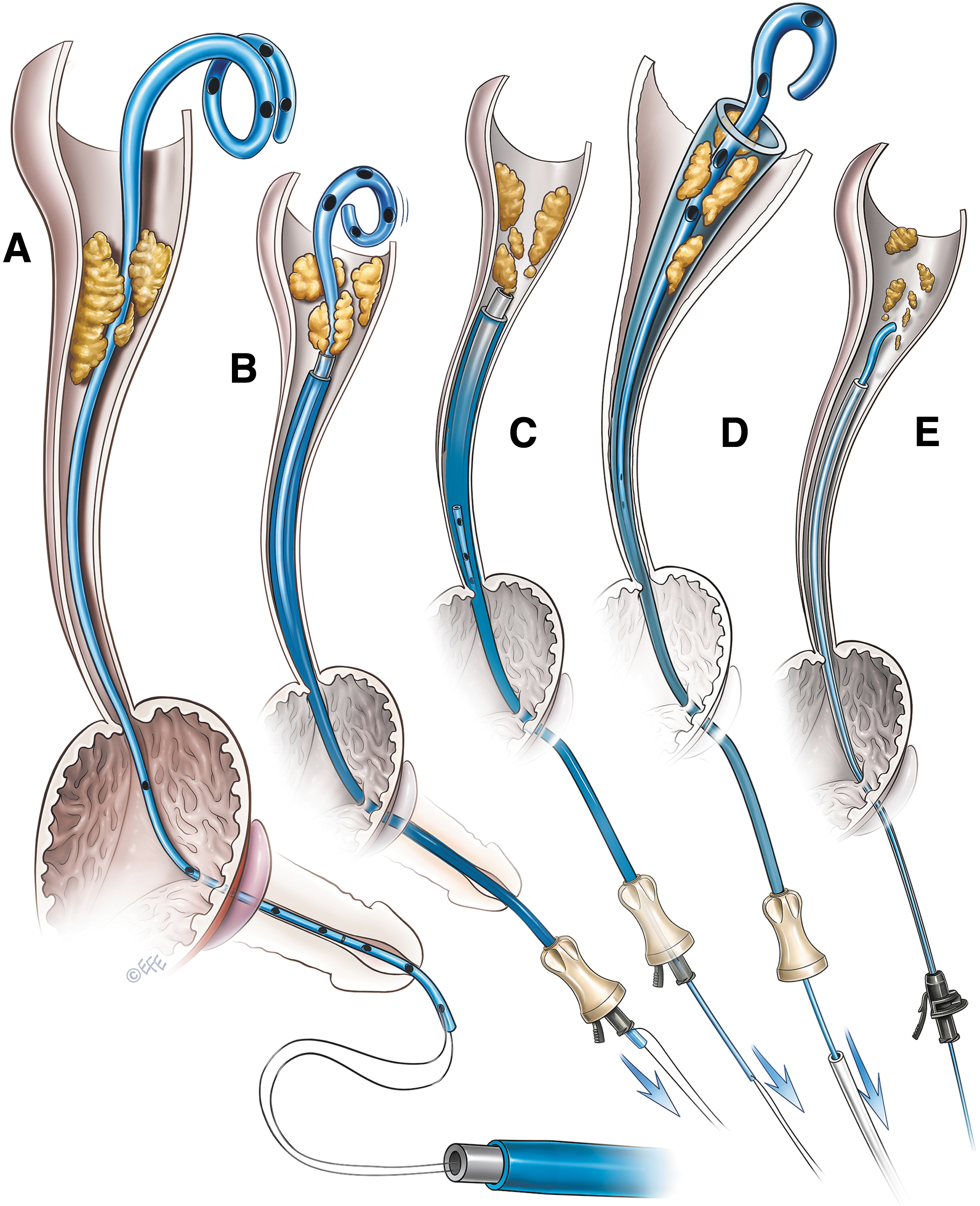
Telescopic access sheath method of removing an encrusted ureteral stent.
The suture was long enough to be retrieved from the proximal end of the access sheaths of varying lengths. The obturator along with the outer sheath was then gently advanced into the ureter over the ureteral stent up to the site of encrustations. The process was done in a telescopic manner under fluoroscopic guidance. During the process, the Prolene suture was held tight with mild tension (Fig. 3B). As the access sheath progressively advanced, the lower end of the stent was retrieved from the proximal end of the sheath when encrustations involved the upper end of the stent.
To peel off the encrustations from the stent, gentle pressure was applied repeatedly with the access sheath assembly by holding the Prolene suture or the lower end of the stent under mild tension (Fig. 3C). Patience is required during this stage of the procedure, as it may take a few minutes to clear the encrustations from the stent. Excessive pressure should be avoided, as it may break the stent. In one patient with mild encrustations at the upper end of the ureteral stent, the encrusted stent was gently pulled inside the access sheath after removing the obturator, and the stent was removed (Fig. 3D). In another patient, we used a refashioned obturator without an outer access sheath to peel off the encrustations and remove the ureteral stent (Fig. 3E). Ureteroscopy was performed to treat the residual stone fragments (Fig. 4). A new ureteral stent was placed, at the end of the procedure, in all the patients. This stent was removed after 1–2 weeks.
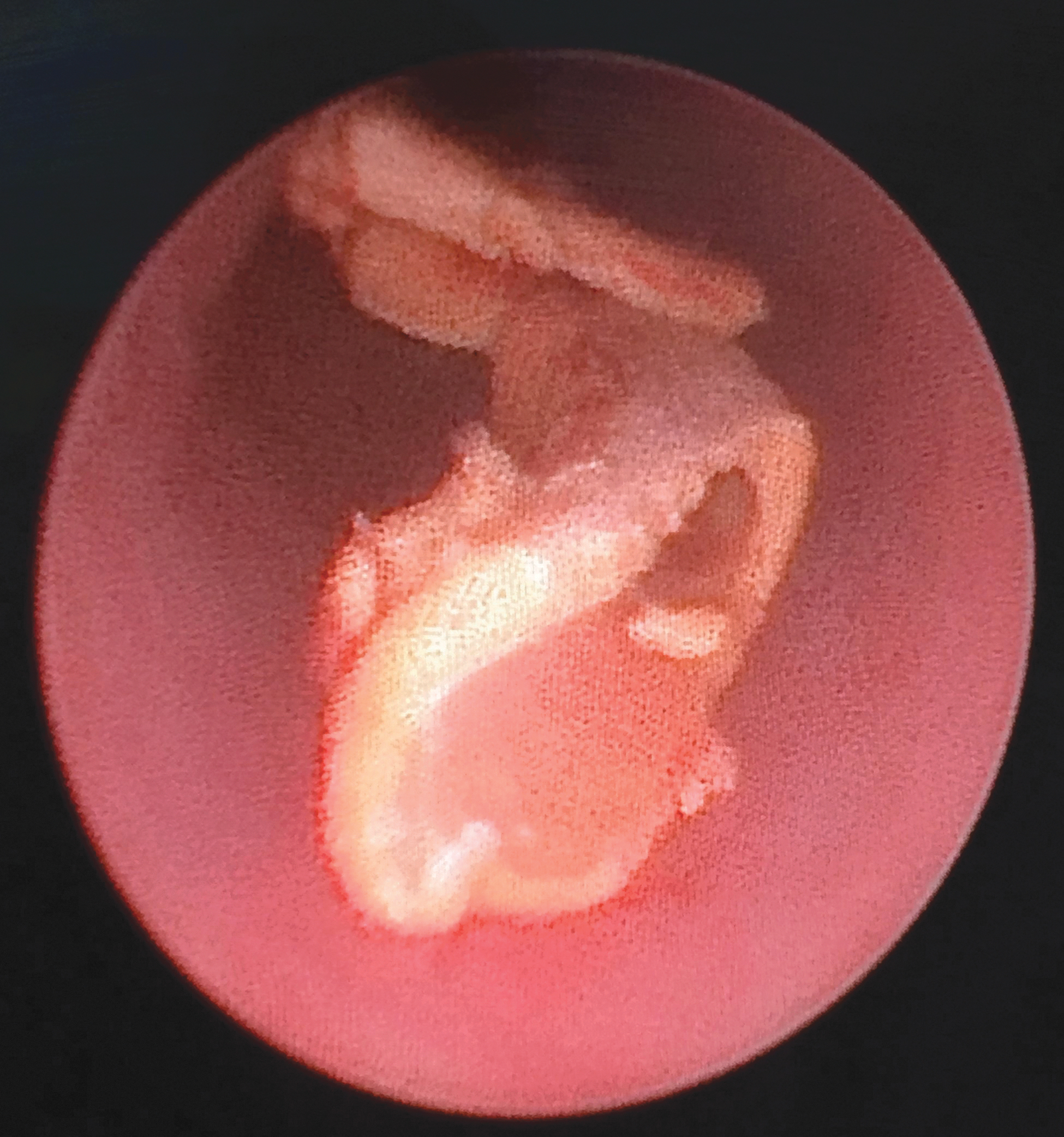
Ureteroscopic view of a peeled off stone fragment.
Technique for removing the knotted stents
In patients with knotted stents, we tried to undo the knot using a stiff guidewire, but this maneuver failed in all cases.
Details of the technical steps for removing the knotted stent are shown in Figure 5. In two patients with a knot in the stent, the obturator along with the outer sheath assembly was used. The lower end of the ureteral stent was passed through the lumen of the access sheath assembly as described earlier (Fig. 5A). Under fluoroscopic guidance, the access sheath assembly was gently advanced over the ureteral stent in a telescopic manner up to the knot (Figs. 5B and 6). At this stage, the lower end of the stent emerged from the lower end of the access sheath.
Telescopic access sheath method of removing a knotted ureteral stent.
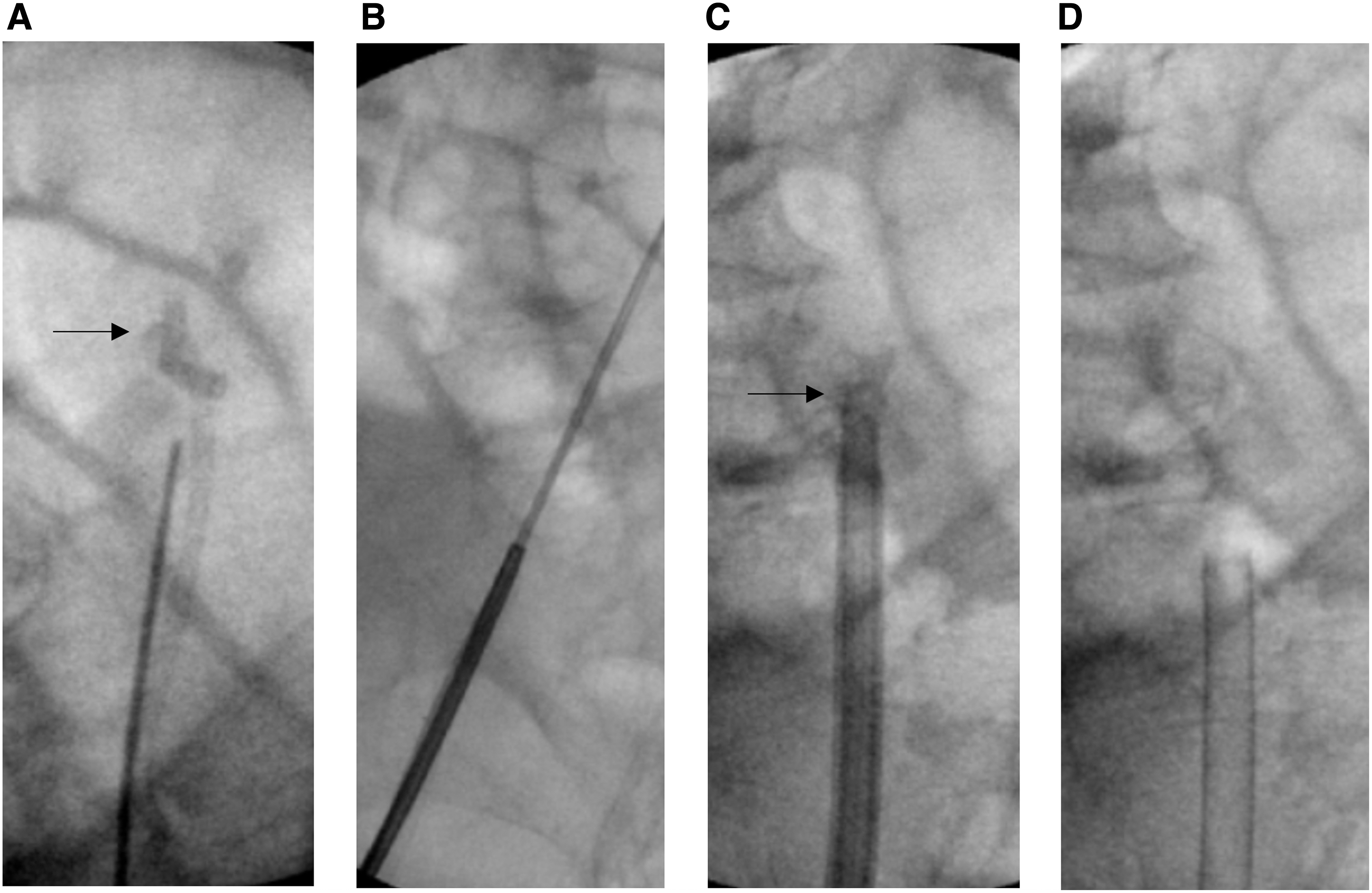
Fluoroscopic images of knotted stent removal.
Gentle pressure was applied by pulling down the lower end of the stent. The knot was easily undone in one patient and the stent was removed (Fig. 5C). In another patient, the knot could not be undone. Hence, we attempted to tighten the knot and decrease its size by gently pulling the lower end of the stent (Fig. 5D). Excessive pulling pressure was avoided to prevent inadvertent stent breakage. At this stage, we removed the obturator of the access sheath, pulled the knot inside the access sheath, and pulled the stent out (Figs. 5E and 6).
In a patient with both encrustation and a knot in the stent, we also used the obturator and an outer sheath assembly. The access sheath assembly was advanced over the ureteral stent, as described earlier, up to the site of encrustation. Encrustations were cleared by gentle and repetitive pushing of the access sheath over the stent under fluoroscopic guidance, as described earlier. Once the encrustations were cleared, the access sheath assembly was gently advanced to the site of the knot. The knot was tightened to reduce its size. Then, the obturator was removed and the knotted stent was pulled out through the access sheath.
Results
The demographics of the nine patients with retained stents in this study are outlined in Table 1. Among them, seven patients were men and two were women. Their ages ranged from 36 to 77 years. In all patients, stents were placed after ureteroscopy for stone management. These stents could not be removed using a flexible cystoscope under local anesthesia. Plain kidney, ureter, and bladder (KUB) radiography and/or plain CT KUB showed encrustations of the ureteral stent in six patients, knots in the upper curl of the ureteral stent in two patients, and both knots and encrustations in one patient. All ureteral stents were either from Boston Scientific or Cook Medical and were ≤5F in size.
Demographics of the Patients
Using the telescopic modified access sheath method, the retained stents were removed in all patients, without any complications. No suture breakage occurred during the advancement of the access sheath assembly over the ureteral stents. Encrustations were peeled off and the stents were removed intact in all the patients. All stone fragments were treated by ureteropyeloscopy using a holmium laser. Similarly, all the knotted stents were removed intact. Retrograde pyelography findings were normal in all these patients with no evidence of ureteral injury. All patients were discharged on the same day.
Discussion
The management of encrusted and/or knotted retained ureteral stents poses a surgical challenge for urologists. In this study, we removed the encrusted and/or knotted stents using a novel technique. Encrustation of ureteral stents is a clinical problem because of their widespread use in various urologic procedures. The treatment of the encrusted ureteral stent may depend on the site and degree of encrustation. Several grading systems exist to define the extent of encrustations and predict the surgical complexity of stent removal. 9,28 –30 Patients in this study mostly had a low grade of encrustation involving the upper part of the stent. Patients with encrustation may require various invasive procedures such as retrograde ureteroscopic manipulation, intracorporeal lithotripsy, holmium laser stent cutting, extracorporeal lithotripsy, percutaneous nephrolithotomy, and open surgery, either alone or in combination. 10 –17 Some patients may even require multiple sessions to clear the encrustations. 18
We, for the first time, have described the telescopic access sheath method to remove the retained encrusted stents. This method is comparatively simpler and less invasive than other methods described in the literature. This procedure was effective in all patients without any complications. As none of the patients had a high grade of encrustations, this technique may be suitable for patients with a lower degree of encrustation. In one patient with encrustations, we used an obturator without an outer access sheath. However, obturators without an outer sheath have a greater tendency to buckle in the ureter, posing a potential risk for ureteral injury. Thus, the use of an obturator with an outer sheath is recommended to avoid buckling and potential ureteral injury.
Although rare, another issue with retained ureteral stents is knot formation in the upper curl. There are a few reports of knotted ureteral stents in the medical literature; however these are either mostly isolated case reports or small case series. 3,19 –26 It is speculated that knot formation may occur due to the excessive length of the coils. 25,26 A variety of techniques have been described to remove the knotted stent. Among them, gentle traction and unknotting of the stent by passing a super-stiff guidewire may represent a minimally invasive technique. 3,20 However, this technique has a potential risk for ureteral avulsion. In our study, unknotting with a super-stiff guidewire was ineffective in the patients.
Retrograde ureteroscopy and holmium laser fragmentation of the knot has also been reported to have effective outcomes. 22,24,26 However, passing the ureteroscope through the side of the retained stent is technically challenging. More invasive procedures, such as the percutaneous approach and open ureterotomy, have also been described. 19,23,25 The telescopic access sheath method described in this report may represent a novel and minimally invasive method which was effective in all three cases without any complications.
Access sheaths of various sizes and lengths are available from various manufacturers. The selection of an access sheath depends on the size and etiology of the retained stents. These procedures should be performed under fluoroscopic guidance with extreme caution to avoid ureteral injuries. If there is buckling of the access sheath or difficulty in advancing the access sheath, the procedure should be abandoned. Excessive force should be avoided while advancing the access sheath. If a gentle and controlled attempt of the telescopic access sheath method fails to remove the retained stent, an alternative procedure should be considered.
The techniques described in this article have limitations, owing to the small size of the case series. These techniques are not suitable for patients in whom the lower end of the retained stent cannot be pulled out of the external urinary meatus. This can especially occur in male patients because of the longer length of the urethra. However, we easily pulled out the lower end of the stent from the urinary meatus in all male patients in this study. This technique may not be suitable for heavily encrusted stents. The telescopic access sheath technique should be considered experimental until its efficacy and safety are proven in a larger series.
Conclusions
Encrustation and knot formation are known complications of retained ureteral stents. The management of such patients may be challenging and may require invasive procedures. The telescoping technique described in this report is a simple method that can be used before proceeding with a more invasive procedure. The small sample size described in this series is, however, a limitation of this study. A larger case series is required to establish the efficacy and safety of this procedure.
Footnotes
Author Disclosure Statement
Patent pending.
Funding Information
No funding was received for this article.
Acknowledgments
The author would like to acknowledge the contribution of Dr Levent Efe for his creation of the illustrations (Figs. 3 and ![]() ) for this article.
) for this article.