
Abstract
Introduction and Objective:
Prolieve® transurethral thermodilatation (TUTD) is the only third-generation transurethral microwave thermotherapy (TUMT) device that incorporates balloon dilation/compression of the prostatic urethra with cooled TUMT, at ≤50 W power. We evaluated its 5-year efficacy in the treatment of symptomatic benign prostatic hyperplasia (BPH) in an open-label prospective multicenter trial.
Methods:
Eligible patients with American Urological Association symptom index score (AUASS) ≥9, peak urine flow rate (Qmax) <12 mL/s, and prostate size 20–80 g without obstructing median lobe were enrolled. Prolieve TUTD was delivered in the office setting under local anesthesia. AUASS, quality of life (QOL), BPH impact index (BPHII), Qmax, and other measures were assessed at baseline, and at least annually thereafter to year 5. Adverse events (AEs) were recorded. Treatment success over time was analyzed using the Kaplan–Meier method while changes from baseline were evaluated using paired t-tests.
Results:
Intention to treat population was 225, of whom 220 with a mean (standard deviation) age of 65 (5.9) completed treatment. 187/220 (85%) did not require urethral catheterization. AUAS, QOL, and BPHII scores significantly improved from baseline in ≤3 months, with sustained improvements to year 5. Qmax also significantly improved from baseline at each annual follow-up evaluation. Cumulative 5-year surgical retreatment rate was 14.2% (95% confidence interval 9.5–20.8). Transient urinary urgency and dysuria were the most reported AEs.
Conclusions:
Prolieve TUTD is a safe and effective treatment option for BPH, with durable long-term improvements in voiding symptoms and urinary flow rates. It has a low catheterization rate and sexual side effects are rare.
Clinical
Introduction
Benign prostatic hyperplasia (BPH) is nonmalignant proliferation of smooth muscle, fibroblasts, and glandular epithelial cells within the prostate gland resulting in its progressive enlargement particularly in the periurethral transition zone. 1,2 BPH progression leads to the development of lower urinary tract symptoms (LUTS) in up to 20% of American men between the ages of 30–79 years, with a prevalence that increases with age. 3,4 Moderate-to-severe LUTS, defined by American Urological Association (AUA) Symptom Index score (AUASS) of ≥8 also increases in prevalence with age, in one study rising to ∼50% by the eighth decade. 5
Surgical therapy in men with LUTS secondary to BPH (LUTS/BPH) is indicated for those unresponsive or unwilling to use medical therapies, or those with BPH-related complications such as refractory urinary retention, renal insufficiency, bladder stones, recurrent urinary tract infections, and recurrent hematuria. 6 Historically, available surgical options for LUTS/BPH were open prostatectomy, with transurethral resection of the prostate (TURP) subsequently introduced in 1926. 7 Despite their efficacy, associated morbidity and mortality were a driving factor behind the development of minimally invasive surgical therapies (MISTs), which provide an alternative to both medical therapy and the more invasive surgical therapies. MISTs can be generally performed in the office setting under local anesthesia and are associated with fewer complications. 8
Transurethral microwave thermotherapy (TUMT) is one of the MISTs for BPH that may be offered to symptomatic patients according to AUA guidelines. 6 It was originally developed in the 1980s, and uses radiant heat energy delivered from a microwave antenna to ablate prostate tissue. Early generation devices delivered heat energy to the prostate transrectally and had limited efficacy as temperatures required for effective ablation of BPH tissue (>45°C) could not effectively be achieved beyond the peripheral zone. Later generation devices incorporate higher power outputs with transurethral energy delivery capable of generating higher intraprostatic temperatures, with or without urethral cooling. 9 Advantages of TUMT include capability to be performed under local anesthesia alone, decreased risks of incontinence, retrograde ejaculation, strictures requiring treatment, and hemorrhage requiring transfusions. 10
Prolieve® transurethral thermodilatation (TUTD) is the only third-generation TUMT system that incorporates delivery of temperature-regulated microwave energy, balloon dilation/compression of the prostatic urethra and urethral cooling, enabling effective prostate tissue ablation at lower power (≤50 W) than for the second-generation (high-energy, nondilating) TUMT systems. 9 Prolieve TUTD was found to be more effective than finasteride in a randomized multicenter trial, 11 and was superior to a second-generation TUMT (cooled thermotherapy) in a head-to-head comparison. 12 Long-term efficacy data for TUTD have not previously been reported. We assessed Prolieve TUTD 5-year outcomes in an open-label, postmarketing prospective multicenter trial.
Patients and Methods
Patients
Patients were recruited from 33 community Urology practice sites nationwide between January 2006 and September 2011. Independent Ethics Committee/Institutional Review Board approvals were obtained at each site. Patients were counseled on all available treatment options for LUTS/BPH and informed consent was obtained from each study participant. Inclusion criteria were men with symptomatic BPH with AUASS ≥9, peak urine flow (Qmax) rates <12 mL/s, and prostate size 20–80 g. Patients who previously failed medical therapy, or who were on concomitant medical therapy were included provided they were on a stable dose for at least 1 week before trial enrollment. Exclusion criteria were subjects with prostate-specific antigen (PSA) levels >10 ng/mL, obstructing (ball-valve type) median lobes, confirmed or suspected malignancy of the prostate, previous pelvic irradiation or pelvic surgery, history of previous prostate surgery and/or nonmetallic urogenital implants, active urinary tract infection, urethral stricture and/or bladder stones, neurogenic bladder and/or sphincter abnormalities due to neurologic disease, diabetes or other disorders, residual bladder volumes >250 mL, urinary retention, bleeding disorders, serum creatinine levels ≥1.8 mg/dL, or prostatic urethral lengths <1.2 or >5.5 cm. Patients who were started on alpha blockers or bladder antispasmodics within 1 week of treatment, as well as those on 5-alpha reductase inhibitor or gonadotropin releasing hormonal analog therapy were also excluded. Patients were enrolled between April 2005 and April 2012 and followed for a minimum of 5 years.
Study procedures
Each patient underwent a baseline assessment, including complete history and physical prostate volume measurement by ultrasound, uroflowmetry, postvoid residual measurement, and cystoscopy, to evaluate for a median lobe, assess urethral length, and rule out urethral strictures or bladder pathology. Serum creatinine and PSA levels were obtained and urine samples for urinalysis and culture were collected. Patients completed AUASS, BPH impact index (BPHII), pain, sexual function, and quality of life (QOL) questionnaires. A special QOL questionnaire was used, consisting of six questions related to the subject's feelings about his urinary condition, perception of urinary difficulties, sexual functions, activities of daily living, general well-being, and social activities. Each item was scored on a seven-point scale, ranging from “delighted” to “terrible” (total score range: 6–42), with higher scores indicating worse QOL.
All treatments were completed under local anesthesia with or without mild sedation alone. The Prolieve TUTD treatment device is displayed in Figure 1. The catheter is anchored in the bladder by an anchoring balloon, positioning the 46F dilating balloon across the length of the prostatic urethra, and a 1.2 cm microwave antenna at the base of the prostate. A specially designed three-sensor rectal temperature monitor was inserted in the rectum and positioned such that the three sensors were at the anterior rectal wall against the prostate to monitor the rectal temperature. The thermodilatation balloon was then inflated to dilate the prostatic urethra and compress the prostate tissue, thereby reducing intraprostatic blood flow to limit heat sink effects within the prostate. Sterile water at 26°C–35°C was continuously circulated through the dilating balloon to maintain urethral cooling. The microwave antenna was then activated to initiate the 45-minute treatment cycle. Continuous rectal temperature monitoring was maintained throughout treatment, maintaining the rectal temperature at 41°C for the duration of treatment (as monitored by the maximum of the three rectal temperature sensors).
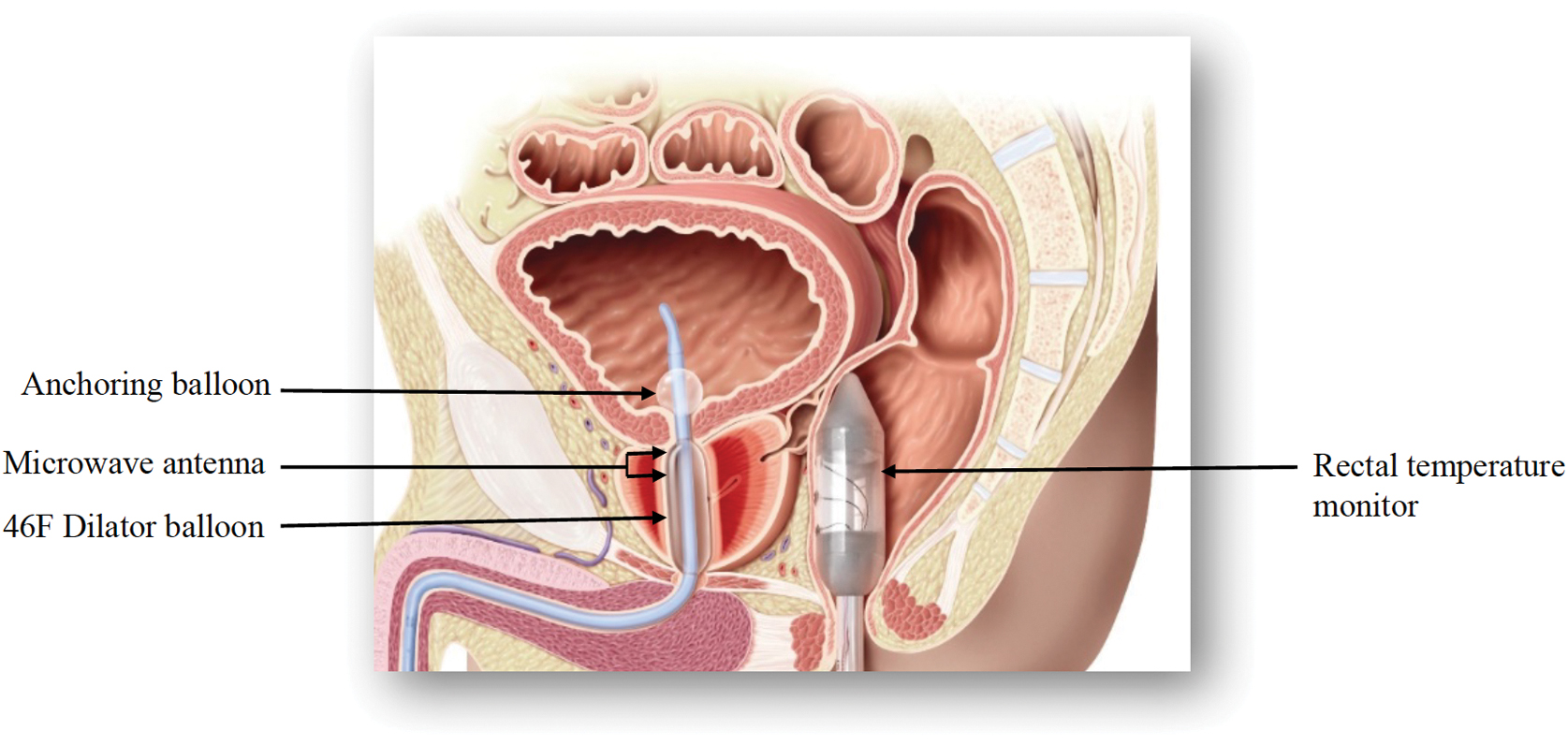
Prolieve® TUTD device. TUTD = transurethral thermodilatation. Color images are available online.
Posttreatment evaluations were completed at 2 weeks, 3 months, 6 months, 1 year, and annually thereafter to year 5, or immediately before retreatment (if applicable) or early termination. The questionnaires and PSA were completed at each follow-up visit, while prostate size (measured by ultrasound) and uroflowmetry were recorded at annual visits only.
The number of retreated patients (i.e., resuming drug therapy or undergoing secondary procedures) and time to retreatment was recorded. Retreatment was offered to patients with a <30% decrease from baseline in AUASS and AUASS ≥13 at least 3 months after the initial treatment. Occurrence and severity of adverse events (AEs) were also recorded, and incidence rate of AEs per 100 person-years of observation was reported.
Statistical methods
The primary effectiveness outcome was time to retreatment. Secondary outcomes were Qmax, prostate size, PSA, and scores on AUASS, QOL, BPHII, pain, and sexual function surveys. Time to retreatment was analyzed using the Kaplan–Meier method, with patients lost to follow counted as retreated with Prolieve. Mean changes from baseline in Qmax, PSA, AUASS, BPHII, and QOL scores were analyzed using paired t-tests. At each follow-up evaluation, proportions of patients who had worse, no change (1%–29% of baseline), or improved (≥30% of baseline) AUASS scores were determined. Similarly, proportions of patients with worse, no change (1%–19% of baseline), or improved (≥20% of baseline) Qmax scores were determined.
Analysis was done using SAS v9.1 Software (Cary, NC, USA).
Results
Two hundred twenty-five subjects were enrolled in the intention to treat (ITT) population out of 375 screened. Of these, five subjects completed only the preparatory steps, but did not subsequently undergo TUTD treatment, resulting in a treated population of 220 men (Fig. 2). Ninety-eight completed follow-up to year 5. Clinicodemographic characteristics of the treated cohort are shown in Table 1. At baseline, mean (±standard deviation) age was 65 (±8.8) years, prostate size 41.4 (±14.5) g, AUASS 20.1 (±5.9), QOL 22.0 (±4.5), and Qmax 8.6 (±2.6). Mean TUTD treatment duration was 47 (±3.4) minutes, with peak rectal temperature 40.9 (±1.2)°C. Of all, 34/220 (15.5%) required catheterization after treatment, with a median (range) catheter duration of 4 (0–10) days. Many catheterizations were done for urinary retention (28/34; 85%).

CONSORT diagram of subject disposition. CONSORT = Consolidated Standards of Reporting Trials.
Patient Characteristics
AUASS = AUA symptom score; BPHII = BPH impact index; PSA = prostate-specific antigen; Qmax = maximal flow rate; QOL = quality of life; SD = standard deviation.
Statistically significant improvements from baseline in AUASS, QOL, and Qmax were observed by month 3 and maintained through year 5 (Figs. 3–5). Mean BPHII also significantly improved from baseline by month 3 through year 5. Mean prostate weight in grams did not significantly differ from baseline levels throughout the study period. At year 5, 54/98 (55.1%) subjects reported a ≥ 30% improvement in AUASS from baseline, while 58/98 (59.2%) reported a ≥ 20% improvement in Qmax from baseline.

AUASS scores over 5 years.

QOL scores over 5 years.

Qmax values over 5 years.
The cumulative 5-year surgical retreatment rate was 14.2% (95% confidence interval [CI] 9.5–20.8) (Fig. 6), while the 5-year medical retreatment rate was 29.3% (95% CI 23.1–36.6). Types of retreatment are outlined in Table 2. Treatment-related AEs with the highest overall incidence rates per 100 person-years in the ITT population were transient urinary urgency (19.4), dysuria (16.3), and urinary retention (11.9) (Table 3). There were no reported urinary fistulas or sphincteric/rectal injuries.
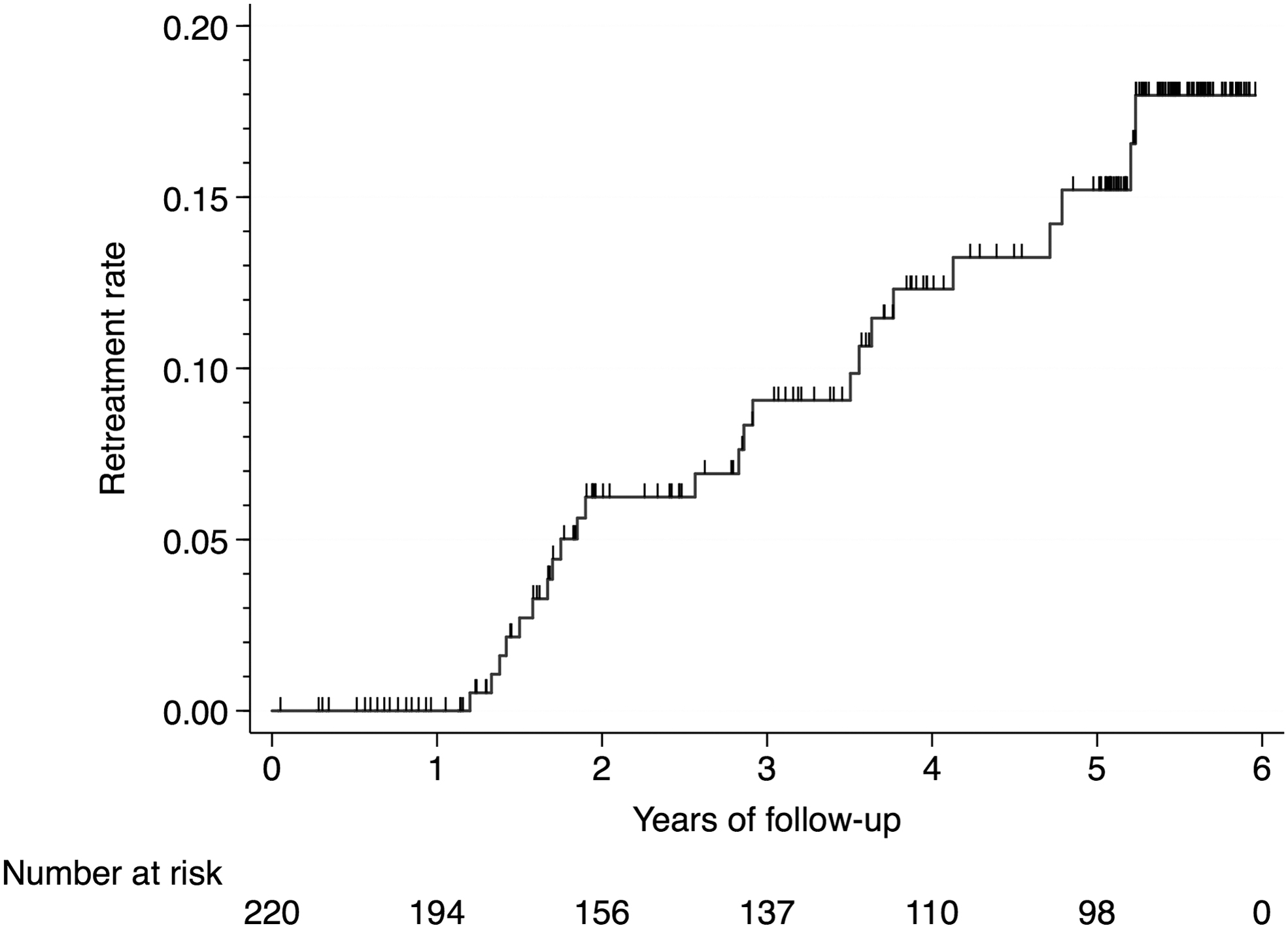
Probability of surgical retreatment over time.
Types of Retreatment
Includes 15 patients lost to follow-up counted as retreated with Prolieve®.
Surgical retreatment was at the discretion of treating physicians and patients, and specific information on the type of surgical retreatment was not collected.
Incidence Rate of Urologic Adverse Events in the Intention to Treat Population Per 100 Person-Years (≥5 Events)
AEs = adverse events; CI = confidence interval; ITT = intention to treat.
Discussion
With 5-year follow-up, Prolieve TUTD achieved statistically significant and durable improvements in urinary flow rates and subjective patient reported outcomes, including AUASS, BPHII, and QOL scores, relative to baseline values. This benefit was achieved for a significant number of patients, with 72.1% of respondents at month 3 and 55.1% at year 5, reporting an ≥30% of greater improvement in AUASS. Posttreatment catheterization rate was low at 15.5%, while surgical retreatment rate was modest at 14.2%. All subjects were able to complete treatment in the office setting under local anesthesia alone, with 189/200 (86%) reporting no or mild treatment-related discomfort.
Prolieve TUTD is a third generation TUMT system that offers several advantages over its predecessors. First, the compression offered by its patented large-bore (46F), high-pressure (13–16 psi) dilatation balloon minimizes heat sink effects by compressing the prostatic vasculature, enabling effective thermotherapy to be delivered at a relatively low microwave energy (20–50 W), and thus contributing to improved patient comfort and safety. Thermodilatation also results in an immediate biologic stent that allows most patients to go home without an indwelling catheter. 13 In a randomized, head-to-head trial comparing Prolieve TUTD with Targis® (Urologix, Inc., Minneapolis, MN, USA), a cooled, high-energy, nondilating TUMT system, Prolieve TUTD offered a significantly higher catheter-free rate (93.7% vs 21.4%; p < 0.001) and earlier improvement in symptomatic relief. 12
Comparable MISTs for BPH that are deliverable in the office setting under local anesthesia alone include transurethral needle ablation (TUNA), prostatic urethral lift (PUL), Rezum thermotherapy, and conventional cooled high-energy TUMT. Published 5-year outcomes for many of these modalities are comparable to those for our study. For PUL, Roehrborn and colleagues reported a significant improvement in 5-year mean AUASS (14.5 ± 8.4 at 5 years) compared with 12.8 ± 6.7 in our study, from baseline values >20. However, the catheterization rate of PUL was 32%, compared with 15.5% in our study. 14 Similar improvements in Qmax were observed in each study, while both cohorts also reported preservation of sexual function. Five-year surgical retreatment rates were similar at ∼14% (<3%/year). 14 For TUNA, Hill and coworkers reported that 49%–62% of patients reported a ≥30% improvement in Qmax over 5 years of follow-up, similar to the rate observed in their study. Five-year surgical retreatment rate with TUNA was also 14%, and overall, there were fewer AEs with TUNA compared with TURP. 15 For cooled high-energy TUMT using the Targis system, Mynderse and colleagues reported improvements from baseline in AUASS and Qmax scores similar to those observed for our study, but posttreatment catheterization rate, including indwelling catheterization and CIC was 50% in their cohort. 16 For Rezum (water vapor thermotherapy), McVary and Roehrborn reported mean improvements in IPSS of 10.4 points, and in Qmax of 4.3 mL/s at 5-year follow-up, 17 compared with 6.7 points and 4.65 mL/s, respectively, for our cohort. Five-year surgical retreatment rate with Rezum in their study, however, was 4.4%, and patients with median lobe anatomy were not excluded. 17 Morbidity associated with Prolieve TUTD was low in our cohort. Incidence of erectile and ejaculatory dysfunction were low at 3.3 and 3.1 per 100 person-years, respectively, which compare favorably with untreated age-matched cohorts and other MISTs, particularly PUL and Rezum. 14,17
Progression of BPH over time in both symptomatic and asymptomatic men is well documented. 18,19 Prostate volume and PSA have been reported to strongly correlate with risk of symptomatic progression of BPH as well as future development of acute urinary retention. 20,21 In our cohort, prostate volume and PSA remained stable for 5 years after Prolieve TUTD, suggesting that Prolieve TUTD may play a role in preventing the progression of BPH in select patients. Considering this along with the added advantages of a low catheterization rate compared with other MISTs, excellent patient tolerability and safety, absent need for intravenous sedation or general anesthesia, and excellent efficacy outcomes in the short and long term, we believe that Prolieve TUTD could be considered first-line therapy for symptomatic BPH in men who may be intolerant of or averse to taking medications over the long-term, or to undergoing surgical intervention for BPH under anesthesia.
Our study is not without its limitations. First, only men with prostate sizes <80 g, and lacking an obstructive median lobe were selected for treatment and is therefore unknown how Prolieve TUTD would perform in these clinical scenarios. Second, about half of the initially enrolled patients were lost to follow-up by year 5. Although survival analysis was used to estimate 5-year retreatment rates considering this, these estimates are actuarial and could represent under or overestimate of the actual rates. Despite these limitations, we believe that our data support the use of Prolieve TUTD as a safe and effective alternative to office BPH treatment in appropriately selected men with moderate-sized prostate glands.
Conclusion
Prolieve TUTD is a safe and effective MIST for men with symptomatic BPH with prostate sizes <80 g. Long-term urinary function outcomes are comparable to those for other BPH surgical therapies, with lower posttreatment catheterization rates and well-preserved sexual function. Prolieve TUTD may also play a role in preventing BPH progression, pending further evaluation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Sponsor: Medifocus INC 10240 old Columbia RB Ste G Columbia, MD 21046.