
Abstract
Purpose:
This article presents the extracorporeal ligation of inguinal hernia defects using an epidural needle and preperitoneal hydrodissection.
Patients and Methods:
Thirteen children underwent laparoscopic extracorporeal ligation of their hernia defect using an epidural needle and preperitoneal hydrodissection. A 5-mm trocar for an operative laparoscope was placed through an infraumbilical incision, a Veress needle for forceps was inserted halfway between the umbilicus and the anterior superior iliac spine on the contralateral side of the hernia, and a 17-gauge epidural needle was inserted at the point of the internal inguinal ring. The hernia defect was closed extracorporeally by a nonabsorbable suture, which was introduced into the abdomen through the epidural needle on the lower half of the hernia defect and withdrawn on the opposite side by a wire-loop through the epidural needle going along the upper half side of the hernia defect in a series of movements. When a contralateral hernia defect is present, laparoscopic-assisted extracorporeal ligation of the contralateral hernia defect is performed during the same operation.
Results:
All patients were discharged uneventfully from the hospital within 24 hours postoperatively. The mean follow-up period is 6.1 months (range 2–12 mos), and no recurrence has been observed to date.
Conclusions:
This article describes a unique technique of extracorporeal circuit suturing of inguinal hernia defects using a minimally invasive technique as afforded by an epidural needle.
Introduction
Recently, it has been described that laparoscopic hernia repair with extracorporeal ligation, as compared with intracorporeal suturing, resulted in a marked reduction in operative time, low comparative recurrence rates, and excellent cosmetic results. 2 This article presents a unique technique of extracorporeal ligation of inguinal hernia in a series of movements performed using a percutaneous epidural needle and preperitoneal hydrodissection with minimal injury to the subcutaneous tissues, nerves, and muscles.
Patients and Methods
From October 2010 to September 2011, 13 children, 7 boys and 6 girls, aged 1.4 years to 9 years (mean 4.2 y), underwent laparoscopic extracorporeal ligation of their hernia defect using an epidural needle and preperitoneal hydrodissection. The surgical technique is as follows: A 5-mm trocar for an operative laparoscope is placed through an infraumbilical incision via the standard open approach. Halfway between the umbilicus and the anterior superior iliac spine, on the contralateral side of the hernia, a Veress needle (Endopath pneumoneedle, Ethicon Endo-Surgery, Inc.) into which forceps can be inserted is introduced. Under laparoscopic guidance, a 17-gauge epidural needle (Terumo Corporation, Tokyo, Japan; out-diameter, 1.40 mm; length, 80 mm) is inserted and advanced along the lower half of the internal inguinal ring. The needle is then advanced extraperitoneally over the testicular vessels/spermatic duct or under the round ligament by performing hydrodissection within the preperitoneal space and grasping the peritoneum with forceps by countertraction through the Veress needle.
Hydrodissection is performed via infusion of isotonic saline through the epidural needle into the preperitoneal space. After this dissection, the epidural needle penetrates the peritoneum on the opposite side, and a small opening is made in the peritoneum. A 2-0 nonabsorbable suture is threaded through the sheath of the epidural needle with the end of the suture remaining in the abdominal cavity and the other end remaining above the skin (Figs. 1a, 1b, 2a, 2b).
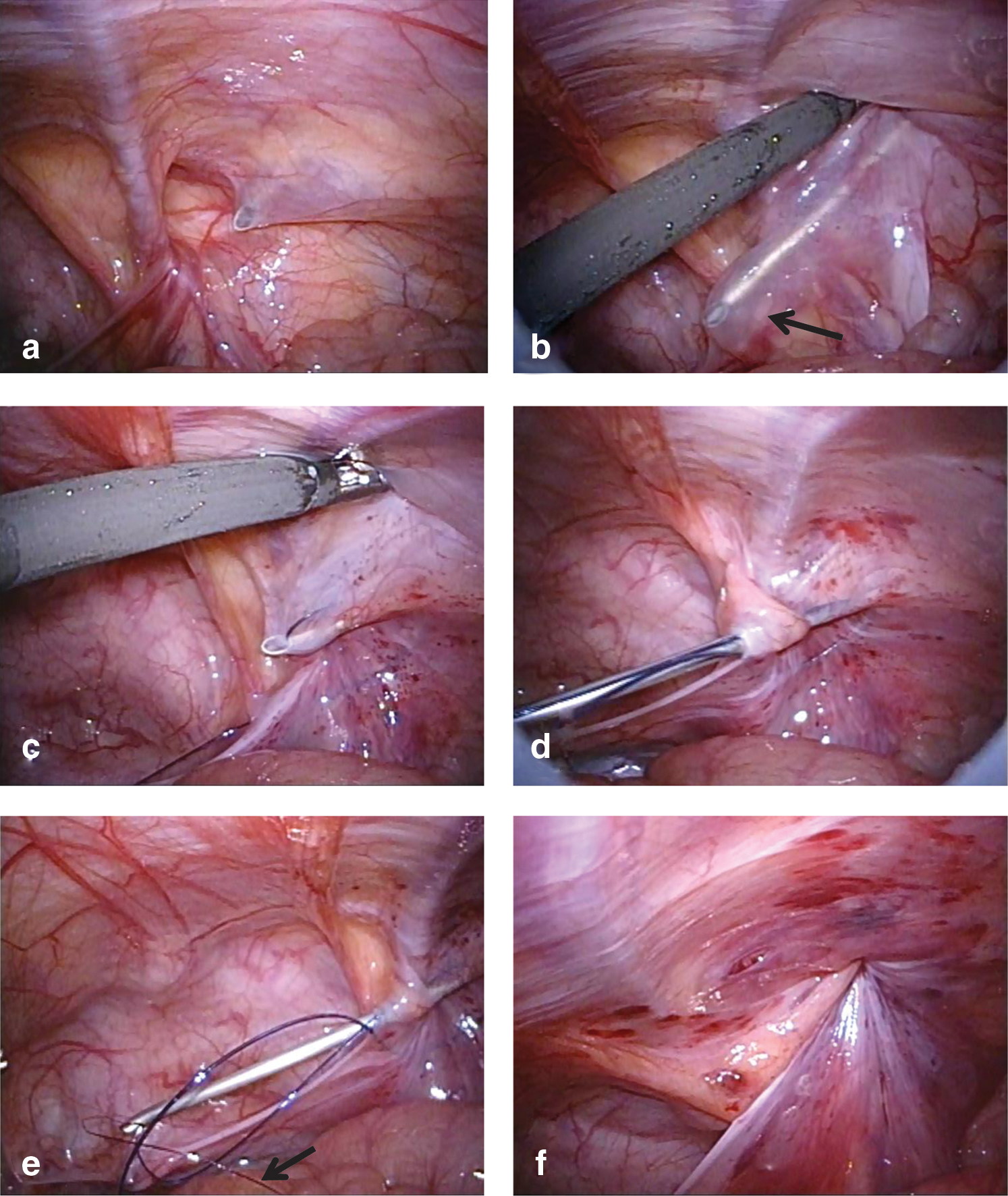
Intraoperative findings in a male patient.
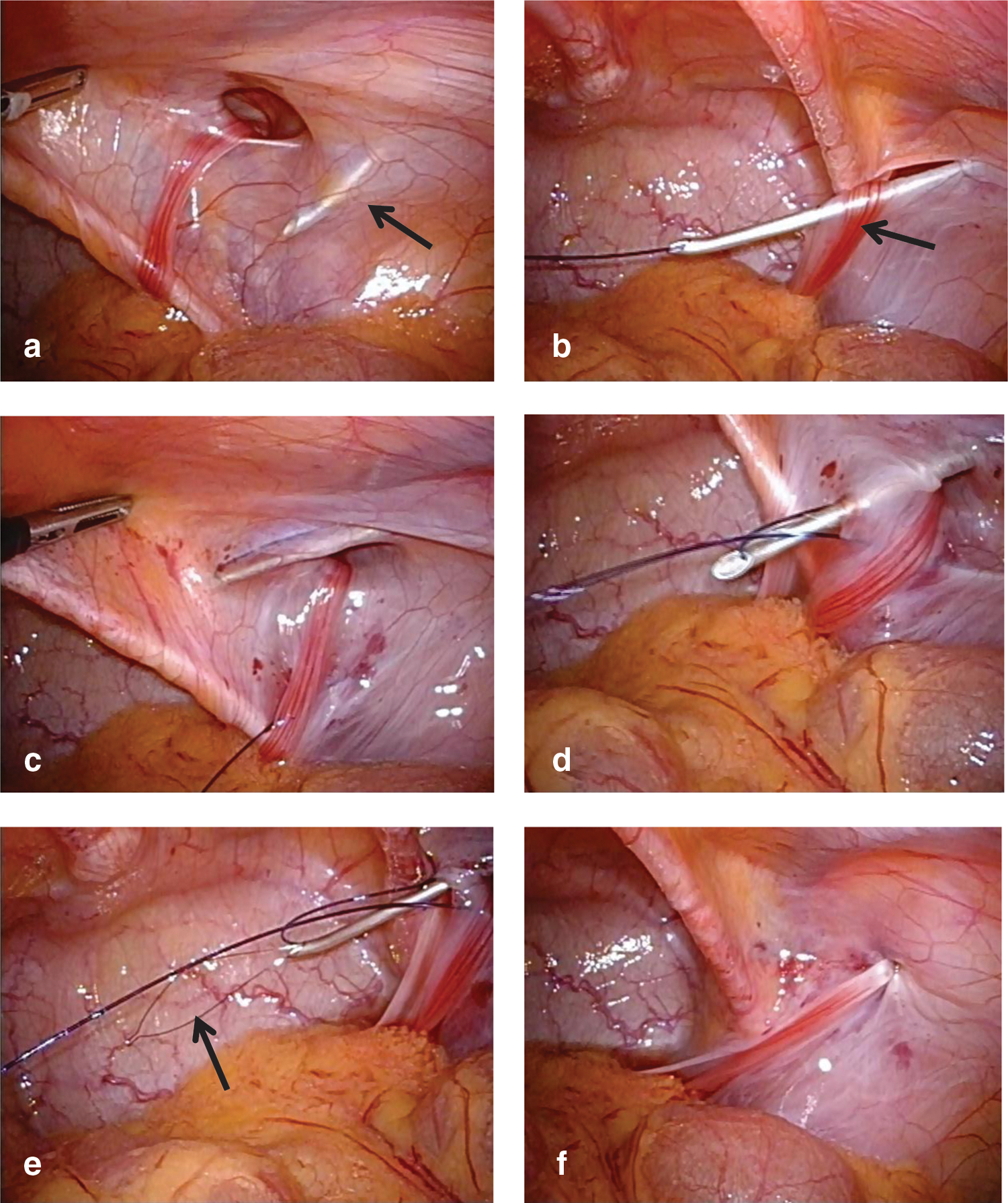
Intraoperative findings in a female patient.
Aided by the previous hydrodissection of the preperitoneal space, the epidural needle easily reaches the upper half of the internal inguinal ring extraperitoneally without removing the epidural needle completely, and the epidural needle is advanced on the same opening of the peritoneum. The nonabsorbable suture is withdrawn by a loop wire through the sheath of the epidural needle (Figs. 1c-–1e, 2c–2e). The epidural needle is then removed from the abdomen together with the suture material.
The hernia defect is closed and the circuit suturing is tied extracorporeally (Figs. 1f, 2f). This approach places the knot above the fascia. These procedures are performed in a series of movement through one needle puncture. When a contralateral hernia defect is present, laparoscopic-assisted extracorporeal ligation of the contralateral hernia defect is performed during the same operation.
Results
The demographic and clinical characteristics of the patients are shown in Table 1. The mean follow-up period is 6.1 months (range 2–12 mos). In 3 of the 13 patients (case 1–case 3), hernia repair using single-port laparoscopic surgery without forceps was first attempted. The single-port laparoscopic technique did not allow evaluation of the contralateral side and prolonged operative time because it was difficult to safely maneuver the epidural needle in the preperitoneal space without forceps. Thus, all remaining patients underwent laparoscopic extracorporeal ligation via a two-port approach from the beginning.
Case 1–case 3: Single-port laparoscopic surgery without forceps; case 4: Laparoscopic intracorporeal suturing of the inguinal hernia ring via two-port laparoscopy was converted to laparoscopic extracorporeal ligation; case 4–case 13: Two-port laparoscopic procedure.
In another case (case 4), laparoscopic intracorporeal suturing of the inguinal hernia ring via two-port laparoscopy was attempted, but this was converted to laparoscopic extracorporeal ligation secondary to the technical difficulty of intracorporeal suturing. In this case, a contralateral patent processus vaginalis was present and thus simultaneously closed, as was the case with a total of four cases.
All patients were discharged from the hospital without complication within 24 hours after the operation. No recurrences have been observed to date.
Discussion
In 1995, Takehara and associates 3 developed laparoscopic percutaneous extraperitoneal closure (LPEC) to manage inguinal hernias in children. This technique involved placing a 4.5-mm laparoscope through an umbilical incision, a 2-mm grasping forceps inserted through a trocar on the left side of the umbilicus, and a 19-gauge LPEC needle with suture material inserted at the midpoint of the right or left inguinal line. The opened hernia sac was closed extraperitoneally by circuit suturing around the internal inguinal ring using the LPEC needle. This approach enables surgeons to perform contralateral exploration without any additional trocars or techniques, followed by immediate and accurate closure of the hernia sac and patent processus vaginalis.
Also described is the technique of one-trocar laparoscopic-assisted extracorporeal closure for inguinal hernias. The hernia defect is enclosed by a nonabsorbable suture, which is introduced into the abdomen by a vascular access on one side of the hernia defect and withdrawn on the opposite side by a homemade hook-pin through a needle puncture wound. Extracorporeal knot tying is subsequently performed. 4
As a modification of single-port endoscopic-assisted ligation with a homemade hooked injection needle, hydrodissection of the preperitoneal space as described in this report encloses without injury of upper subcutaneous tissues and a small peritoneal gap of the suture. 5,6
In laparoscopic extracorporeal hernia repair, it is important to prevent injury to nerves and muscles as could occur by their inclusion in the circuit suturing. Also important is complete closure of the peritoneum at the lower portion of the circuit suturing scheme, thus not leaving a gap at the location of the spermatic vessels/vas deferens or the round ligament. A small peritoneal gap between sutures at the lower portion of the circuit suturing could be approximated by passing the epidural needle into the same small opening of the peritoneum while grasping the peritoneum with forceps. A small peritoneal gap between sutures at the upper portion of the circuit suturing could be approximated by directing a nonabsorbable suture within the epidural needle to the other side of the inguinal hernia ring in a series of movements. Furthermore, the fact that the suture is passed through the epidural needle without complete removal of the needle minimizes the chance of including subcutaneous tissues, nerves, and muscles in the upper portion of the circuit suturing. In addition, damage to spermatic cord structures is also prevented by performing hydrodissection of the preperitoneal space ahead of the epidural needle as it is advanced.
Overall, we have shown this procedure with its incorporation of the epidural needle in conjunction with a two-port laparoscopic scheme to be simple, safe, and effective in managing inguinal hernias in the pediatric population.
Conclusions
This article describes a unique technique of extracorporeal circuit suturing of inguinal hernia defects using a minimally invasive technique as afforded by an epidural needle.
Footnotes
Disclosure Statement
No competing financial interests exist.