
Abstract
Purpose:
Laparoscopic Madigan prostatectomy have not been reported yet. We modified the Madigan prostatectomy to make it suitable for laparoscopically enucleating hyperplastic glands larger than 100 g.
Patients and Methods:
Between May 2007 and Oct 2008, extraperitoneal laparoscopic prostatectomy with maintenance of the intact urethra had been performed on 16 patients with benign prostatic hyperplasia (BPH) and glands larger than 100 mg. To make it suitable for laparoscopic use, two major modifications had been made: (1) Open the prostate capsule near the bladder neck without sutures along the opening; (2) identify the bladder neck mucosa before recognizing the urethra. All patients were evaluated preoperatively and postoperatively. Data were compared with those from open surgeries.
Results:
All laparoscopic procedures were successful with the total operative time of 111.8±28.6 minutes, which had no significant difference compared with open surgeries. Estimated blood loss of laparoscopic procedures (112.5±47.8 mL) was significantly lower than that of open surgery. The catheterization time and hospital stay time was significantly shorter than open surgery. The improvement of the International Prostate Symptom Score, maximum flow rate, and quality-of-life score were not different between the comparing groups.
Conclusions:
The laparoscopic Madigan prostatectomy is a safe and feasible approach for large glands (BPH). Furthermore, its advantages include shorter learning curve, reduced blood loss, less retroejaculation rate, shorter catheterization time, and shorter hospital stay.
Introduction
We present our modification of the Madigan prostatectomy to make it suitable for laparoscopic enucleation of the hyperplastic gland larger than 100 g.
Today, benign prostatic hyperplasia (BPH) is commonly managed with transurethral resection of the prostate (TURP). For lesions larger than 100 g, however, it remains a big challenge for most TURP surgeons. In China, some urologists would rather choose traditional open surgical procedures 2 –5 than TURP, because the open procedures offer good long-term functional results compared with those of TURP. 6 –8
The open simple prostatectomy has been successfully transferred to the laparoscopic approaches with Millin techniques as described by Rehman and associates. 9 Recent reports indicate that it offers advantages exceeding its open predecessor; in addition, both operations are comparable in improving prostate symptoms and quality of life. 10 –12 Indeed, a laparoscopic approach has brought proven benefits, including lower morbidity, limited pain, shorter hospital stay, and earlier return to normal working activities. Thus, the laparoscopic Millin prostatectomy has the potential to combine the advantages of a minimally invasive technique with the favorable results of open surgery. Our efforts with the laparoscopic Madigan prostatectomy have not been reported, however.
Patients and Methods
From May 2007 to Oct 2008, extraperitoneal laparoscopic prostatectomy with urethra preservation was performed on 16 patients. All the patients had symptomatic BPH, and the volumes of their prostates were larger than 100 cc measured by transrectal ultrasonography. All 16 patients were evaluated with the International Prostate Symptom Score (IPSS) and quality-of-life (QoL) questionnaires, maximum flow rate (Qmax) and urodynamic studies, serum prostate-specific antigen (PSA) test, and digital rectal examination preoperatively. IPSS questionnaires and Qmax were also evaluated 2 months after surgery.
Two sample t test was used for the statistical analysis, and P<0.05 was considered as the criterion of statistical significance.
Surgical technique
After the general anesthesia had been induced, the patient was prepped and draped in a supine, slight Trendelenburg position with a rolled towel under the lumbar curvature and the table slightly broken at about 15 degrees to extend the lower abdomen. A 20F Foley urethral catheter was placed with balloon inflated.
A 20-mm semicircle incision was made in the infraumbilical crease, and the anterior rectus fascia was incised vertically. The rectus muscle fibers were separated vertically, exposing the posterior rectus fascia. The space between the rectus muscle and the posterior rectus sheath was bluntly developed by finger dissection; then, a self-made balloon was inserted through the space toward the pubis. The balloon was slowly inflated with 500 mL air to develop the retropubic working space. After placement of a 10-mm trocar into the umbilical incision, the 0-degree laparoscope was put in and a 10-mm trocar was placed in each side lateral to the rectus muscle on the umbilicus plane under observation. High-flow carbon dioxide insufflation was used up to 10 to 15 mm Hg. A 5-mm trocar was placed in the iliac fossa at the level of a so-called McBurney point on either side under visual control. The areolar tissue and fat were coagulated and swept gently from the anterior surface of the bladder and prostate using bipolar forceps.
The superficial veins over the prostate were carefully coagulated. The junction of the bladder and the prostate is clearly identified by moving the catheter. The most important of our improvements is to make a transversal incision near the prostatic-vesical junction (Fig. 1) as long as crossing the base of the prostate. The capsular incision is deepened by monopolar (or bipolar) coagulation until the exposure of the plane between the prostatic surgical capsule and the adenomatous tissue. The incision near the bladder neck allowed good blood control and a possibility of managing the enlarged middle lobe. Capsular sutures along both sides of the incision as described previously 9 were not necessary.
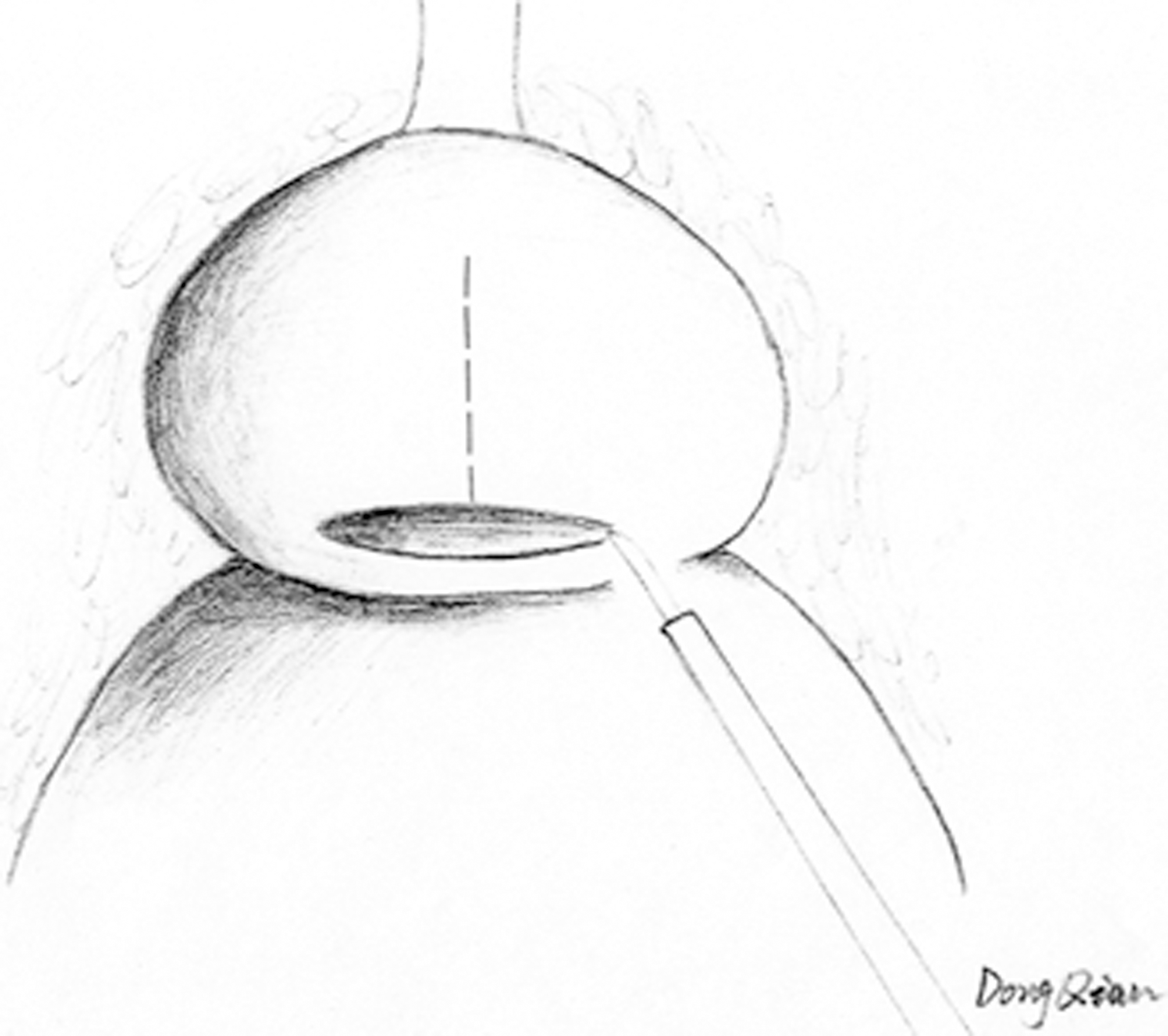
Transversal incision near the prostatovesical junction crossing the base of the prostate.
After incision, the surgical capsular plane was developed distally, and the isthmus was cut open toward the apex by harmonic scalpel, so that the prostate is divided into two separate lobes (Fig. 2). The urethra can easily be identified near the border of the prostate and bladder neck between the right and left lobes. The urethra was carefully divided from the prostate by sharp dissection, and the urethra was fully preserved (Fig. 3). Then the surgical capsular plane was sequentially developed laterally to the posterior plane and cranially to the bladder neck. Finally, the right and left lobes were divided by posterior excision of the prostate until the whole hyperplastic nodules were freed. After the specimens were taken out of their positions, the capsular incision was closed by running suture (2/0 polyglactin on a tapered needle) (Fig. 4). An EndoBag was introduced. and the specimens were taken out through the umbilical port. A drain was placed via the right 5-mm port.
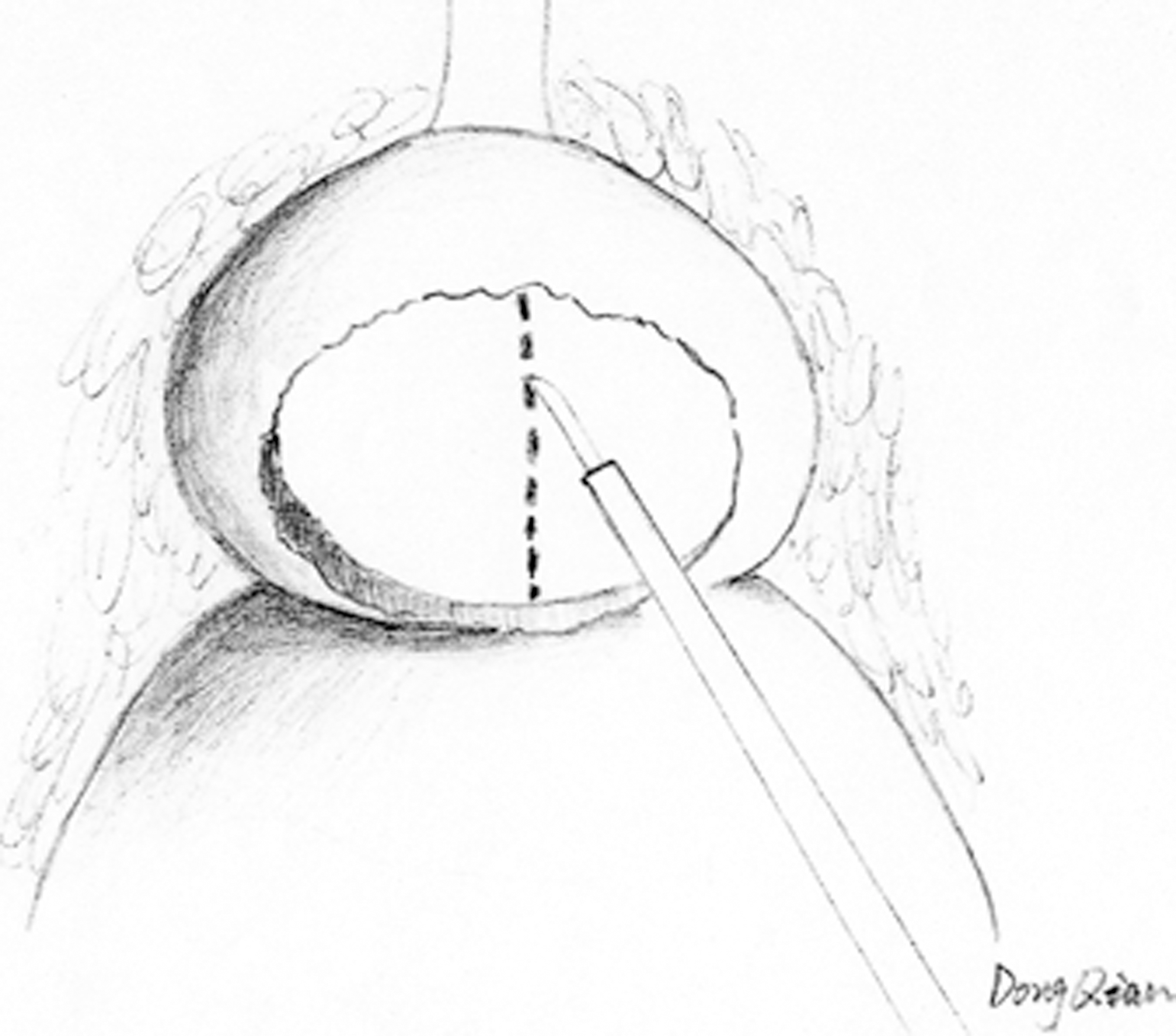
The isthmus was cut open toward the apex by harmonic scalpel.
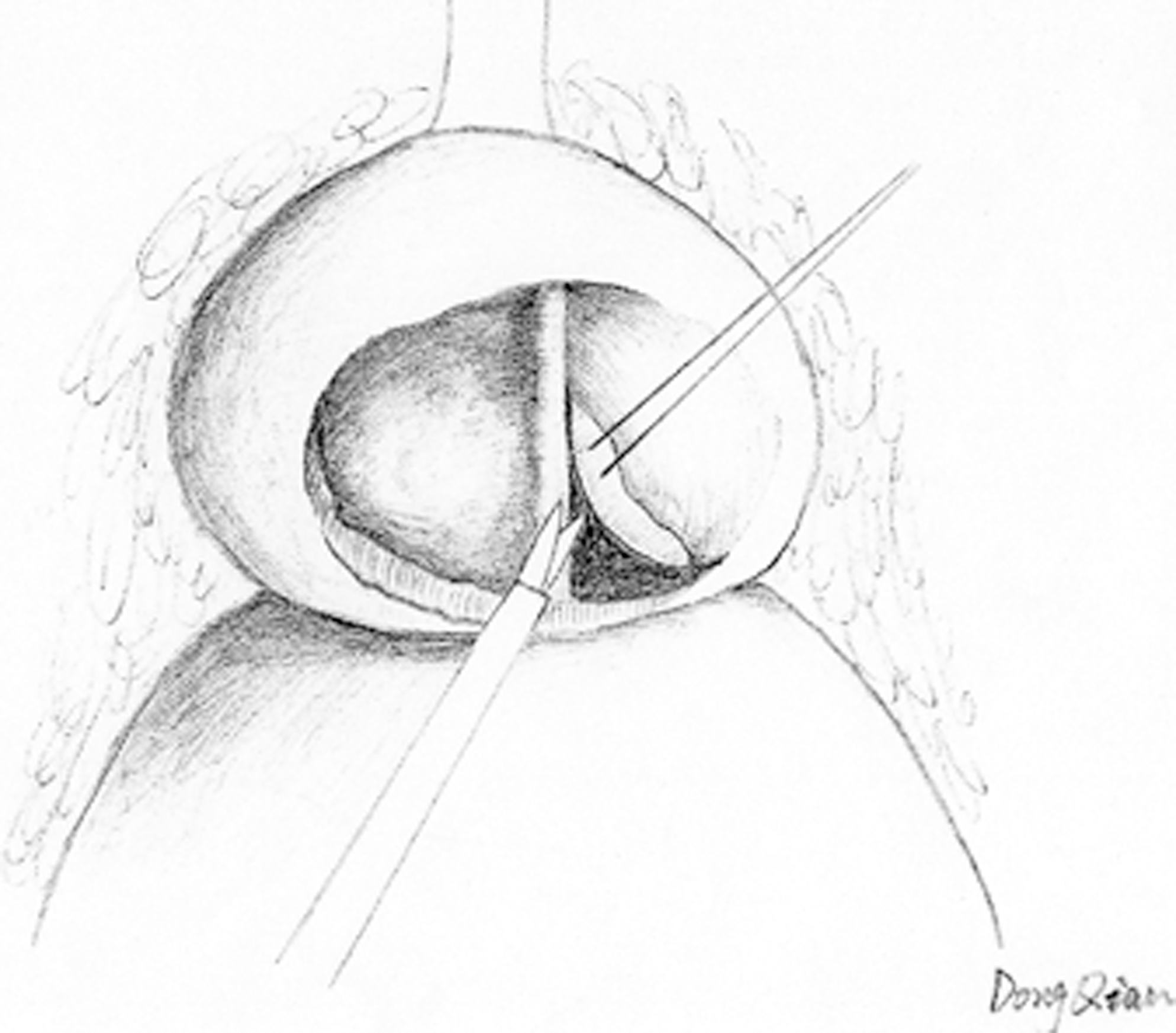
The urethra was carefully divided from the prostate by sharp dissection.
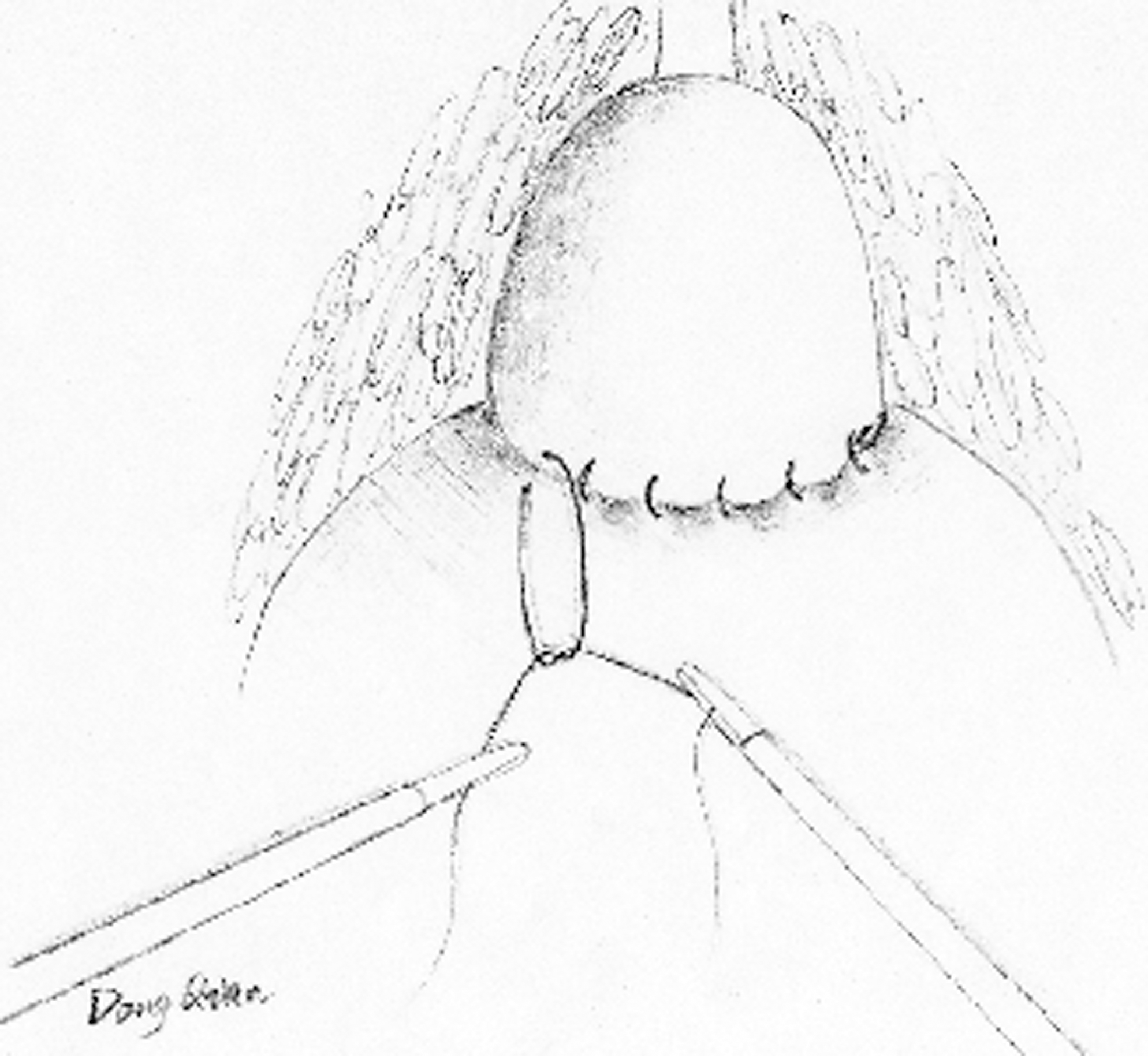
Closure of the capsular incision with polyglactin sutures.
Results
All 16 cases of extraperitoneal laparoscopic prostatectomy were successful without open conversions. Among them, roughly 20% had urethral lacerations. The total operative time was 111.8±28.6 minutes, compared with other open surgery data 12 ; there was no significant difference in operative time. Estimated blood loss was 112.5±47.8 mL; it was significantly lower than that of open surgery, and no patient needed transfusions. Drain removal was performed in 24 to 48 hours. The Foley catheter was removed when the urine was totally clear, usually in 2 days after operation. The analgesic requirement was minimal, and hospital stay was 3.5±0.8 days after operation. The catheterization time and hospital stay time were significantly shorter than those of open surgery, and there were statistical differentiations (Table 1).
TRUS=transrectal ultrasonography.
The enucleated prostate specimen weight was 104.7±23.3 g; it was equal to 79.1% of the prostate volume estimated on preoperative transrectal ultrasonography. These data are the same as described by Porpiglia and colleagues. 12 Follow-up examination at 2 months showed that the Qmax was 22.3±1.6 mL/s; the IPSS score was 4.5±1.8, and QoL score was 0.5±0.5. Compared with preoperative data, there were visible improvements on IPSS, Qmax, and QoL scores (Table 2). The erectile function was preserved in all the patients who were potent before surgery. No urinary incontinence was reported by patients.
IPSS=International Prostate Symptom Score; Qmax=maximum flow rate; QoL=quality of life.
The overall follow-up was 19.6±4.2 months. In this period, there were no complications found, such as urinary inflammation and urethral stenosis.
Discussion
TURP represents the optional surgical treatment option for the medium-size prostate, for the prostate larger than 70 g. Although resection ratios increased, with the largest occurring in prostates of 71 to 100 g, the surgeon resects no more than 50% of the gland volume. 13 Prostates larger than 100 g have been managed traditionally with open surgical procedures. 2 –5 Open prostatectomy accounts for 14% to 32% of the total invasive procedures for BPH in Europe; in other countries, this rate is as high as 68% 6,14 –16
In recent days, a majority of urologic surgeries are performed laparoscopically. Mariano and coworkers 17 first reported a transperitoneal approach for retropubic simple prostatectomy. 10 More recently, extraperitoneal laparoscopic transcapular prostatectomy (Millin) has been proposed; minimal bleeding, a reduced transfusion rate, shorter hospitalization, and faster recovery were its additional advantages. This minimally invasive technique is a reasonable alternative to the open simple prostatectomy for large glands with reduced morbidity. 11,12,18
In our laparoscopic Madigan prostatectomy procedure, we had made several modifications on the previous operation. The first improvement is bleeding control. To our knowledge, the figure-of eight stay sutures at the prostate and bladder on either side of the prostatovesical junction is not necessary. The bleeding can be controlled easily by bipolar or monopolar coagulation. Second is the incision site. We have selected a transversal incision on the prostate capsule that is proximal to the prostatovesical junction; this is useful to handle the bleeding and enlarged middle lobe.
Third is urethra preservation. It is beneficial to the postoperative bleeding reduction, no bladder irrigation, shorter catheterization time, and shorter hospital stay, and there is no retroejaculation. It may also be beneficial to the prevention of stenosis of the membranous urethra; but longer term follow-up is needed for confirmation.
Compared with open surgery (Millin) reported by Porpiglia and associates, 12 there has been significant improvement in blood loss, catheterization time, and hospital stay (P<0.001) (Table 1) in laparoscopic surgery in the group with preservation of the urethra. There are no differences in operative time, prostate volume (transrectal ultrasonography [TRUS]), and removed gland volume (P>0.05) (Table 1). They also have compared laparoscopic surgery with open surgery; the results have shown that laparoscopic surgery is comparable to open surgery with the advantage of lower blood loss, but there is no difference in catheterization time and hospital stay, which differs from our result. This difference could be induced by urethra preservation, which is very useful for the reduction of catheterization time and hospital stay.
For the enucleated prostate specimen weight, our result was 104.7±23.3 gm; this was equal to 79.1% of the prostate volume estimated on preoperative TRUS, which is similar to previous description. 12,19 During our 19.6±4.2 months follow-up, compared with preoperative data, there were visible improvements on IPSS, Qmax. and QoL scores. Further observation is still needed for long-term outcome.
Conclusion
Laparoscopic Madigan prostatectomy with preservation of the urethra is a safe and feasible approach for large BPH. The benefits of laparoscopic Madigan prostatectomy, including a short learning curve, early removal of the catheter, the absence of postoperative lower urinary tract symptoms and hematuria, a shorter period of hospitalization, and lower incidence of retrograde ejaculation and erectile dysfunction, etc, had been characterized.
Footnotes
Disclosure Statement
No competing financial interests exist.