
Abstract
There is extensive evidence that when people have parks, gardens, and greenery near their homes, they gain mental and physical health benefits. As a result, there are a number of health care initiatives to motivate people to spend time in local green spaces. This article proposes a network of access and engagement with nature to support health and well-being: Equitable access to nearby nature spaces; nature prescriptions to encourage people to integrate time in nature into their lives; and nature programming that involves people in organized activities in nature to address health challenges. This article defines nature prescribing and nature programming and provides examples of each, with an emphasis on initiatives that support mental health. It compares these approaches according to four criteria: Participant engagement, program leadership and community partnerships, the role of health care providers, and financial sustainability. Considering nature prescribing and programming in this ordered way can help identify strategies to increase time in nature, which are compatible with health system resources and participant needs. The article closes by considering implications for practice and research.
Introduction
Alarge body of evidence documents the physical and mental health benefits of time spent in nature (see recent reviews by Li et al., 2023; Silva, Matos, & Gonçalves, 2023; White et al., 2023). These benefits include better immune system functioning (Andersen, Corazon, & Stigsdottir, 2021; Kuo, 2015), less self-perceived stress (Corazon, Sidenius, Poulsen, Gramkow, & Stigsdotter, 2019; Litt, Alaimo, et al., 2023), emotional well-being (Bratman et al., 2019; Litt, Alaimo, et al., 2023; Tillmann, Tobin, Avison, & Gilliland, 2018; Zhang, Mavoa, Zhao, Raphael, & Smith., 2020), social connection (Goldy & Piff, 2020), and reduced loneliness (Astell-Burt et al., 2022; Hammoud et al., 2021). Although contact with nature benefits physical as well as mental health (White et al., 2023), this article emphasizes programs that reduce stress and loneliness, increase social-emotional well-being, and treat mental illnesses like anxiety, depression, and suicidality.
Across the world, conditions of contemporary life are failing to support people's social-emotional health and well-being. As the Centers for Disease Control and Prevention (2023a) defines it, “Mental health includes our emotional, psychological, and social well-being.” Socially, people do well when they have positive connections with family, friends, and community members; but in the United States, about half of adults report feeling lonely at least some of the time (Office of the Surgeon General, 2023), and rates of loneliness rise steeply between ages 10–18 years (Shovestul, Han, Germine, & Dodell-Feder, 2020). Loneliness has serious adverse consequences for health and well-being overall (Hawkley & Cacioppo, 2010).
According to other indicators of worsening mental health, since 2015, self-reported anxiety, depression, hopelessness, and suicidal ideation increased sharply among adolescents 12–18 years of age in the United States (Centers for Disease Control and Prevention, 2023b; Panchal, Rudowitz, & Cox, 2022); and in recent surveys, one in three adults and half of young adults 18–24 years of age reported symptoms of anxiety and depression (Panchal, Saunder, Rudowitz, & Cox, 2023). Similar increases in loneliness and declines in mental health have been reported globally (Buecker & Horstmann, 2021; World Health Organization, 2021a).
Traditional responses to mental health treatment, from hospitalization for acute crises to individual and group therapy in clinics and private counselors' offices, cannot adequately address these high levels of need. The United States, European countries, and countries globally face workforce shortages in health care and particularly in mental health care, with access to mental health care most limited in middle- and low-income countries (Office of the U. S. Surgeon General, 2022; World Health Organization, 2021b). Therefore, it is necessary to broaden mental health care beyond hospital wards, clinics, and therapy offices by integrating care into settings across communities.
This article examines initiatives to extend care into natural areas like parks, gardens, farms, and wild spaces, given their healing potential. As we use the term “nature” in this study, it can involve different “spatial scales and degrees of human influence, from a potted plant or a small urban creek or park to expansive, “pristine” wilderness” (Bratman et al., 2019, p. 2). Initiatives to increase the time people spend in nature are commonly grouped together under the term “nature prescribing”: However, this article argues that this general use conceals significant differences between “nature prescribing” and “nature programming.”
It makes the case that it is useful to distinguish nature prescribing and nature programming, based on the levels of resources that they require and people's levels of need, to identify which approach best serves people's needs in different contexts. It is then possible to envision how the two approaches can be applied together in a coordinated network of support for health and well-being.
Encouraging time in nature is one example of the wider practice of “social prescribing,” which involves a staff member in a primary care practice, general practitioner's office, hospital, or clinic, who counsels patients about community-based services in their local area, which offer social support and promote healthy activities (Leavell et al., 2019). Given the need to extend health care across community settings, social prescribing has been adopted by health systems in a number of countries, with interest growing in the United States (Khan & Giurca, 2023). In United Kingdom, the National Health Service has funded specialized “link workers” to staff general practitioners' offices and connect patients with community opportunities (Kiely et al., 2022). Some countries call staff who serve this function “navigators” (Alliance for Healthier Communities, 2020).
Social prescribing has become a popular approach to enable people to take advantage of community resources that address social determinants of health: The political, economic, and social systems, social norms, community institutions, and physical conditions in which people live (Blass & Kurup, 2010). Only about 10% of the variation in life expectancy within a population is due to people's access to quality health care (Kaplan & Milstein, 2019). More important are the physical and social environment, socioeconomic conditions, and public policies that shape individuals, families, and communities more generally. One environmental determinant is access to nature.
The term “nature prescribing” has been applied broadly to any effort by health care professionals or other service providers to encourage people to spend more time in nature—from counseling about the benefits of contact with nature to writing down specific directions about how much time to spend in local nature spaces, to programming activities with participants in nature. In practice, “counseling,” in the sense of advice about the benefits of time in nature and how to integrate nature into daily life, overlaps with “prescribing,” in the sense of writing down specific directions for a patient to follow (South, Kondo, & Razani, 2020). Both share the common feature that health care professionals or link workers recommend what patients should do on their own, such as visiting local parks for a specified amount of time each week or engaging in particular activities in nature.
Because the term “nature prescribing” has been used more widely than “nature counseling,” this article applies it to cover both general advising, as well as written prescribing. Nature prescribing tends to follow a medical model that treats nature like a medication to be administered to “passive patients,” who experience positive physiological effects just by being in nature (Chawla, 2022). Consistent with this perspective, there has been active research to determine the “dose” of time in nature required to deliver health gains (White et al., 2019).
In contrast, “programming” involves people in planned wellness activities at nature sites. It treats people as “active agents,” who take advantage of opportunities that nature affords to extend their capabilities, feel autonomy and competence, and experience positive emotions (Chawla, 2022; Sachs, Tharry, et al., 2022). Because these activities typically involve groups, they can build social relations (Chawla, 2021; Hartig, 2021; Sachs, Tharry, et al., 2022; Teig et al., 2009). A recent review of social prescribing practices (Litt, Coll-Planas, et al., 2023) identified different models that practices take. One, a “holistic group-based model,” involves facilitators who work in collaboration with primary and other care organizations, engaging participants in group processes. They pass information about participants' activities and experiences back to their organizational partners, to enable cycles of continuous improvement. This model corresponds to the definition of “programming” used in this study.
Because both prescribing and programming involve a variety of community partners, this article uses the general terms “care professionals” or “care providers” for the people who facilitate time in nature to support health. In addition to doctors and other medical staff, they may include staff in public health offices or other social service agencies, in addition to partners in community nature spaces. As examples in this article show, community partners may include park rangers, naturalists, farmers, educators, and community garden leaders. The term “health care professionals” is used when it only refers to medical staff and allied health professionals.
A Network of Access and Engagement with Nature
To support different levels of need for resources in nature for physical and mental well-being, this article proposes a coordinated network of nature-based health practices (Fig. 1). It includes equitable access to high-quality, nearby nature spaces; nature prescriptions to spend more time in nearby nature; and nature programs that offer treatment for the needs of specific populations. Each practice in this network requires resources, including care professionals who need training to deliver services, as well as funding for operations.
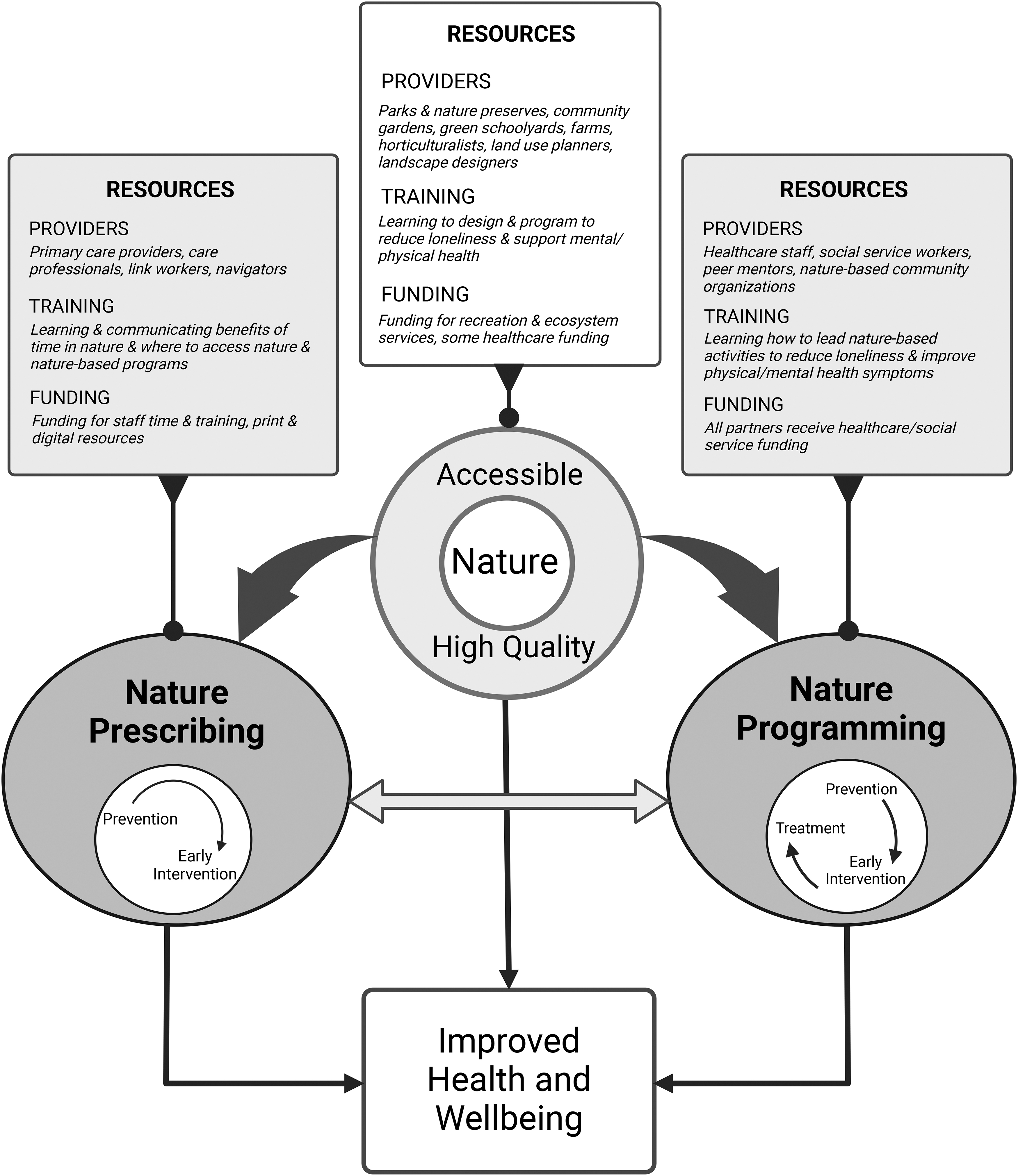
A coordinated network of access and engagement with nature for improved health and well-being. (This figure was created with BioRender.com.)
This article focuses on clarifying and comparing different health care approaches to increasing time in nature, but it is important to begin by acknowledging that none of them is possible without public access to nature. They rely on the work of “nature providers” such as land use planners, green infrastructure planners, landscape designers, park departments, and community garden associations that create, conserve, and restore natural habitats at every scale. Public parks began in the 19th century with the intent of supporting health (Collins, 2020), and their provision is a precondition for the interventions to increase time in nature, which this article describes.
Research shows that people at higher socioeconomic levels are more likely to have greenery in their surroundings and parks with more amenities (Rigolon, Browning, & Jennings, 2018; Rigolon, Browning, Lee, & Shin, 2018; Han, He, Liu, Zhao, & Huang, 2023). Racial and ethnic minorities tend to be most disadvantaged in terms of high-quality natural spaces (Rigolon, Browning, & Jennings, 2018). Creating equitable access to nature is a critical foundation for all nature-based approaches to support health.
Beyond equitable access to nature for everyone, the next part of this network to increase time in nature is nature prescribing, when staff in a health care or social service setting encourage people to integrate more time in nature into their daily lives. The third component of the network is nature programming, which involves people in organized interventions in nature, such as group activities, to reduce loneliness, increase physical activity, or teach mental health coping skills.
While programs in nature can serve people at every level of need, they are uniquely suited for people who require interventions that treat diagnosed medical and mental health conditions. Nature prescribing and nature programming can be mutually reinforcing by sharing resources, such as staff, training, and locations, and by providing cross-referrals. Participants in nature prescribing can be assessed for a higher level of care based on their needs and referred to a nature programming group when appropriate. Likewise, when participants complete a nature programming group, they can “step down” into a nature-prescribing intervention.
Individuals who take advantage of opportunities to stay healthy by spending time in nearby nature are practicing a form of preventive care (Klompmaker et al., 2022). People achieve the benefit of preventing certain chronic illnesses, whether they find accessible nature on their own, receive counseling and a prescription from a health care professional, or participate in an organized nature program. Individuals with physical or mental health symptoms may benefit from spending time in nature as a form of early intervention to halt the progression and mitigate the impact of their symptoms. Once people have been diagnosed with a physical or mental illness, they require evidence-based treatment, which can alleviate their symptoms and restore them to healthy functioning. When treatment involves activities in nature, it needs to be directed by health care professionals, who may work with community partners, whom they have trained.
This article argues that it is helpful to think about the role of each part of this network systematically, as well as how all of its parts can be intentionally connected. The following two sections offer definitions and examples of nature prescribing and nature programming, each in turn. These two approaches are then compared, based on levels of participant engagement, program leadership and community partnerships, the roles of health care providers, and financial sustainability. The article concludes with reflections about how all three nature-based health practices can complement each other in a coordinated network of community initiatives, and how research can help identify effective collaborations.
Nature Prescribing
As we use the term in this study, nature prescribing involves any form of counseling to “review the health benefits of nature and assess current levels of outdoor use, patient perceptions of nature, and potential barriers to increase nature contact” and to “talk with patients about where to spend time in nature” (South et al., 2020, p. 607). It includes interventions that involve a physician, or other care providers, giving patients written recommendations to spend time outside (Kondo et al., 2020). Given direct physiological, emotional, and cognitive benefits that people derive just from being in nature, it emphasizes increasing the dose of time that people spend outdoors in nature spaces. The two examples below illustrate general advising and written prescribing.
Stress Buster strategies
“Stress Busters” (ACES Aware, n.d.) is a service developed by the California Surgeon General to provide educational tools and resources that focus on ways to manage stress, or prevent it whenever possible, so that individuals can avoid the negative health impacts of “toxic” stress (Shonkoff et al., 2012). One of the seven Stress Buster strategies is “experiencing nature.” The web-based toolkit includes the resource, “Did You Know? Being in Nature Can Help Prevent and Manage Stress,” which recommends everyday practices in nature, as well as how to find nature-based community resources when someone needs extra support. Providers can access these resources when they counsel patients to increase time outdoors and prescribe visits to local natural areas.
Park Rx
In 2009, the National Environmental Education Foundation held several workshops that brought together providers who were giving nature prescriptions to their patients. Further organizing efforts by the Institute at the Golden Gate in 2013 helped spread the word about what was happening in California. This led to the creation of more park prescription programs across the United States. Park Rx programs are locally organized and reflect the varieties of nature experiences that are available in diverse communities.
These programs “include some type of ‘push’ from a health care or social service provider and ‘pull’ from a park system that connects participating individuals with local outdoor activities” (Institute at the Golden Gate, n.d.). Park Rx America (n.d.), a national nonprofit, helps with coordination and organization for programs across the country. Currently, there are estimated to be more than 100 local Park Rx programs in the United States (Institute at the Golden Gate, 2020). With the mission of decreasing chronic disease, increasing health and well-being, and fostering environmental stewardship, they educate primary care and social service providers about the health benefits of time in nature and how to help patients find parks near their homes.
Nature Programming
Nature programming has a long history of association with environmental education, but for the purposes of this article, it is defined as programming activities in nature with the intention of supporting mental or physical health, or both. Rather than just advising people to spend more time in nature, it requires participants' active engagement in scheduled activities under the direction of trained facilitators. People usually participate in nature programs for a limited amount of time (Kondo et al., 2020), but the lessons they learn and skills they develop can become daily habits that provide continuing benefits. Because the programs involve groups, they can also build social connections. These programs can be managed by a hospital, clinic, school, or community organization, such as a community garden, as the following four examples show:
Pathways nature healing program
Pathways is a unique nature-based group therapy program for people struggling with a variety of mental health problems, including depression, anxiety, bipolar disorder, post-traumatic stress disorder, and other issues. It was initially developed at Boulder Community Health hospital in Boulder, Colorado (Boulder Community Health, n.d.). Pathways offers help for people in crisis, who require intensive care every day, but who do not need hospitalization. Participants receive treatment while living at home, and they may continue to work or attend school.
Pathways participants work with a multidisciplinary team of mental health providers, including psychiatrists, nurse practitioners, masters-level licensed therapists, and allied health professionals. Therapy takes place in a variety of outdoor settings with support from community partners such as City of Boulder Open Space and Mountain Parks (City of Boulder, n.d.) and Light Root Community Farm (Light Root Farm, n.d.). While participants are in treatment, they work on building effective coping skills and learning resilience by overcoming challenges through activities in nature. Many Pathways participants have moderate to severe mental illness, including mood disorders, psychotic disorders, and trauma-related symptoms.
Pathways' groups are co-facilitated by additional team members with experience in nature-based activities, including outdoor instructors, certified naturalist guides, and farmer educators. Pathways offers a unique training curriculum for volunteers through the City of Boulder Open Space and Mountain Parks community outreach program. In addition, Pathways offers training for program graduates to become peer mentors. Both the volunteer and peer mentor training are directed by licensed mental health professionals. Because Pathways meets criteria as both an intensive outpatient program and a partial hospitalization program, direct service costs are covered by most insurance.
Stay Healthy in Nature Every Day
The Stay Healthy in Nature Every Day (SHINE) program has been supporting at-risk pediatric populations since 2012 by providing access to nature. Operating in the University of California San Francisco (UCSF) Benioff Children's Hospital Oakland Primary Care Clinic, and serving around 50,000 well visits annually, it includes both nature counseling and nature programming. Patients are screened for access to safe green spaces to play outdoors, and those who require assistance are referred to SHINE through the Electronic Medical Record or by contacting the Family Navigation Desk (Razani, Long, Hessler, Rutherford, & Gottlieb, 2020). Staff at the UCSF Center for Nature and Health then contact the referred patients and offer behavioral counseling to tackle any barrier hindering access to nature, using motivational interviewing and the Precaution Adoption Process Model to guide their counseling (Center for Nature and Health, 2021).
Patients with the highest barriers to nature access benefit from SHINE's facilitated nature outings that are offered once a month (Razani et al., 2019). The outings are a collaboration between the hospital and the East Bay Regional Park District, primarily targeting low-income and diverse populations. Each is facilitated by both a naturalist and a physician, with a focus on using nature as a therapeutic tool for stress relief and resilience-building in children and their families. The patient's entire family attends the outings, which include developmentally appropriate and play-based methods for stress reduction, fostering family connections, and promoting overall well-being.
Meeting in Nature Together
Meeting in Nature Together (MINT) was developed as a community partnership in collaboration with the University of Colorado Boulder, the Children's Hospital of Colorado, and New Legacy Charter School—a school dedicated to the unique needs of pregnant and parenting teenagers in Aurora, Colorado (Sachs, Coringrato, et al., 2022). As a grant-supported elective course at the school, it was designed to use nature experiences to minimize loneliness, increase self-value, and promote coping skills to balance school and parenting responsibilities. Study participants received financial incentives and elective school credits for participation. During the first semester, students met weekly online for 8 weeks (due to COVID-19), and during the second semester, they met in person to participate in facilitator-led nature walks, as well as nature-based journaling, photography, mindfulness, and group discussions. MINT activities included guest speakers, nature-based meditations, relationship skill conversations, and photo-elicitation discussions of students' nature photography.
Re-Imagining Environments for Connection and Engagement: Testing Actions for Social Prescribing in Natural Spaces
Re-Imagining Environments for Connection and Engagement: Testing Actions for Social Prescribing in Natural Spaces (RECETAS) is funded by the European Commission, with aims to develop and test the effectiveness of a nature-based social intervention that the initiative calls Friends in Nature, reduce loneliness, and increase health-related quality of life in six countries in Europe, Australia, and South America (Coll-Planas et al., 2024; Litt et al., 2024).
The premise of the project is that social prescribing in natural spaces can alleviate loneliness by engaging people in socially organized activities that are connected to the natural environment where they live and carry out their daily activities (e.g., nature walks, community gardening, bird watching, tree planting, community cycling). It is developing and testing interventions that engage diverse populations vulnerable to loneliness, who may face barriers to accessing and enjoying public space and outdoor activities in groups. Importantly, these interventions are linking professionals working in local health and social care systems with nature-based solutions nearby to support lonely people.
The Friends in Nature model tested in RECETAS cities is adapted from the Circle of Friends® methodology and customized to the specific target population in each study area, with a focus on nature-based activities. Two main components are expected to complement each other: (1) peer support group and empowerment processes, including specific group dynamics and elements adapted from Circle of Friends® (individual interviews, empowerment letters, diaries, and training) (Jansson, Savikko, & Pitkälä, 2018; Pitkälä, Savikko, & Routasalo, 2015); and (2) nature-based activities chosen by participants from a menu based on their preferences. These interventions will be tested in Barcelona, Cuenca, Helsinki, Marseille, Melbourne, and Prague. As the study is in progress, more information can be found at RECETAS (n.d.).
Similarities and Differences between Nature Prescribing and Nature Programming
Similarities and differences between nature prescribing and nature programming are apparent if we assess them according to four criteria: participant engagement; program leadership and community partnerships; the role of health care providers; and financial sustainability (following Kondo et al., 2020). Evaluating them according to these criteria can help health care and social service professionals determine which approach will be most effective in different contexts, in terms of participant needs and care system resources. These comparisons, which are summarized in Table 1 and analyzed in more depth in Table 2, are discussed in the following four sections. The text and tables identify both barriers and advantages to each approach.
Summary of Nature Prescribing and Nature Programming
Similarities and Differences Between Nature Prescribing and Nature Programming
Participant engagement
Participant engagement, for purposes of this discussion, includes two components: Adherence and activation. The number of scheduled sessions that each participant attends is the program's attendance rate. The number of participants who attend the program for the entire duration represents the program's completion rate. Both the attendance rate and the completion rate are measures of adherence. Activation refers to how participants incorporate their experiences into their daily lives after they complete a program. The more frequently they engage in behaviors influenced by their experiences in either nature prescribing or programming, the greater the activation level.
An important prerequisite for participant engagement in either nature prescribing or programming is access to a care professional who participates in such a program. In the United States, primary care providers are the most common health care professionals who participate in nature prescription programs. While many primary care providers, especially pediatricians, are strong proponents of Park Rx programs, they often cite lack of insurance reimbursement as a major barrier to recommending time in nature to patients (Besenyi, Hayashi, & Christian, 2020). The later section on “Financial Sustainability,” however, shows that ways to get reimbursed are possible.
Even after participants gain access to nature prescribing, they face barriers to engagement. To take advantage of prescribing recommendations, they must live in walking distance of parks or other natural areas or have transportation to these resources. Social and cultural barriers may make it difficult for some people to accept counseling about the benefits of spending time in nature (Crnic & Kondo, 2019). For example, symptoms of mental illness—including lack of motivation, loss of interest, low energy, and social anxiety—can make it difficult for people with mental health problems to find transportation, keep appointments, and engage in group activities (Wood, Polley, Barton, &Wicks, 2022). When parents struggle with food insecurity and unstable housing, they are not likely to prioritize access to nature for themselves and their children (Razani et al., 2020).
A primary gatekeeper for nature programming in the United States is health insurance. Most participants in the Pathways program require insurance authorization to pay for this type of mental health service. Participants may be referred to a program by a care professional or contact a program directly to seek admission; but either way, most participants require insurance authorization to pay for this type of service, or they must pay for the cost out of pocket. Social and cultural barriers can also deter people from enrolling in nature programming, but once participants are in a program, they do not need to provide their own transportation or live near a park. Nature programs to increase health typically provide transportation to and from activity sites or use sites in walking distance of the program location.
In the United States, participants in nature prescription programs are often on their own to determine when and how to access nature once they receive initial counseling and instructions. In countries like United Kingdom, link workers follow up to help participants make connections. In nature programming, participants are supported by a range of service providers, who may include psychiatrists, nurse practitioners, social workers, licensed mental health professionals, other allied health professionals, naturalist guides, park rangers, farmer educators, and more.
How do these barriers and levels of support affect engagement? When Kondo et al. (2020) did a meta-analysis of published studies reporting evidence for nature prescription programs, they found that adherence was poor, despite attempts to reduce barriers (see also Coffey & Gauderer, 2016). However, a randomized trial within SHINE that featured park prescriptions versus personalized planning and structured programming in city parks found that each approach increased park visits, with the families who received independent park prescriptions making more weekly visits (Razani et al., 2018). In the Pathways program, preliminary evaluation data showed that adherence to treatment was high (85%), compared to the average for similar hospital-based intensive outpatient and partial hospitalization programs (40–50%). More systematic studies with a variety of programs are needed.
Activation is more difficult to measure than adherence, as it requires assessment of behavior changes that occur after a prescription has been “filled” or a program has been completed. One outcome that is used to assess activation in nature prescribing is any change in time spent outdoors in nature, such as a local park. One study showed an increase in outdoor physical activity for pediatric patients given a nature prescription (Zarr, Cottrell, & Merrill, 2017). The randomized trial within SHINE found that, with each park visit, parents experienced decreased stress and loneliness (Razani et al., 2018). Their children had increased resilience with each increase in weekly park visits, at all levels of adverse childhood experiences, stress levels, and age.
Assessments for Pathways and MINT suggested participants' motivations for continuing to spend time in nature. At the conclusion of the Pathways program, participants met with a psychiatrist for a final interview where they reported on any change they experienced as a result of program attendance. More than 50% said they felt connected to the natural world in a different way than before the program, and many said that this connection to something “bigger than me” and “larger than my problems” gave them a new perspective on the challenges they faced in their lives. A similar number felt “more relaxed,” “calmer,” and “less distracted” when they were outside in nature.
They reported that whenever they wanted to feel “more connected” or “deal with daily stress,” they went into nature between group sessions or after completing the program. In a survey at the close of MINT activities, 100% of participants described feeling closer to nature and 83% felt connected with others in the program. According to their teachers and parents, they increased time outdoors and shared about experiencing improved mental health (Sachs, Coringrato, et al., 2022). These results suggest that nature-based programs can change participants' perspectives and behavior, but more research is needed to identify long-term effects.
Program leadership and community partnerships
Program leadership and community partnerships vary between nature prescription and nature programming models. As mentioned earlier, primary care providers and staff in primary care clinics are the strongest proponents of nature prescription programs. They provide the counseling and education that are required to make this type of intervention effective. Usually, they work with little to no direct support from other community organizations, although in some cases, nonprofits such as Park Rx America, or state initiatives such as ACES Aware, may provide help with educational materials and web-based applications.
Nature programming offers multiple avenues for people to participate in leadership roles, which are not limited to health care practitioners. In addition to an interdisciplinary health care team, groups are co-facilitated by a wide range of experts, who may include park rangers, naturalist guides, outdoor educators, farmers, and horticulturalists. This diversity of roles allows leaders in community-based organizations to participate in creating and implementing nature programming, such as staff in park systems, local gardens, community farms, and environmental nonprofits. Nature programming also allows participants to become peer mentors to provide program help and assist others in treatment after they complete their own treatment. The Pathways program, for example, incorporates peer mentor training into its treatment curriculum.
The role of health care providers
The current workforce shortage in health care means more demand for health care providers' time due to higher caseloads and fewer support staff. Kondo et al. (2020) found that the success of nature prescribing depends in large measure on the capacity of physician leaders or “clinical champions” to get approval for implementation within their organization and keep the initiative functioning. Health care providers' lack of time was a major barrier to sustaining nature-based prescribing. In the United States, most of the prescriptions to spend time in nature come from primary care providers, including family physicians and pediatricians. Primary care providers have some of the highest rates of burnout and work-related stress (Office of the U.S. Surgeon General, 2022). For nature prescribing to be successful in the United States and elsewhere, providers need time and support to be effective leaders and champions.
Nature programming incorporates educators, trainers, guides, and staff from outside the health care system, making its staffing model more resilient. Trained community members, including naturalists, park rangers, and outdoor educators, can help mitigate the shortage of licensed mental health workers. Responsibility for leadership in nature programming is shared by health care “champions,” as in nature prescribing, as well as advocates from community organizations. Community partners bring different expertise in team building and knowledge of nature that complements the skills of health care leaders.
Financial sustainability
In addition to a reliable workforce, nature prescribing and programming need predictable financing to be widely adopted and sustained. In 2019, the National Health Service in United Kingdom initially funded 1000 “link workers” in general practitioners' offices to do social prescribing. By 2023, the NHS intends to have 4500 link workers in its primary care networks, delivering social prescribing services to 900,000 patients (Tierney, Mahtani, & Turk, 2020). In addition, the NHS has dedicated funds to offset the costs of recruiting and hiring link workers. However, many voluntary, community and social enterprise organizations claim that funding is not sufficient to provide appropriate management and supervision of these new nonmedical care workers (Cole, Jones, & Jopling, 2020).
The situation in the United States is more precarious, where social prescribing is usually not reimbursed by government-funded insurance, such as Medicare and Medicaid, or commercial insurance. In the United States, nature prescribing is primarily funded by national and local philanthropies and health care charities (Sandhu, Alderwick, & Gottlieb, 2022). In addition, a few hospitals and professional societies, like the American Academy of Pediatrics, provide support. Because nature prescription funding is unpredictable and unreliable, programs struggle to make long-term plans or set ambitious goals. The funds they receive are usually only enough to cover direct services.
Nature programming takes place in a variety of clinical settings and in different outdoor environments, which means that funding depends on the context where it occurs. Because programs like Pathways serve people with mental health problems, who need more intensive services than they can receive in an outpatient setting, but not inpatient hospitalization (a level of care referred to as ambulatory behavioral health care), they offer billable services that can be reimbursed by national health services, commercial insurers, and systems like Medicare and Medicaid in the United States.
Similarly, because health care staff accompany clients on SHINE outings to parks, their time together can be billed. This means the revenue stream for nature programming can be more predictable and reliable than support for nature prescribing, which can make it possible to offer scholarships, provide training for clinicians, conduct outcomes research, and contribute resources to community partners. Because national philanthropies, local foundations, and hospitals that want to support nature programming do not have to fund direct service costs, their contributions can go toward these opportunities.
Discussion
This article evaluates nature prescribing and programming initiatives across four domains that are critical for long-term success: Participant engagement; leadership and partnerships; health care professional involvement; and financial sustainability. In addition to directions for future research, these domains suggest next steps for practical improvements. Making data on attendance and completion rates a standard outcome measure for participant engagement, as well as data on activation in terms of whether participants continue to include activities in nature in their lives and to what effect should be priorities for formative program assessments, as well as research studies.
Learning how to train and sustain leadership for nature prescribing and programming in health care and social service settings is also important. As the examples of Pathways, SHINE, and RECETAS illustrate, staff in parks, recreation departments, educational farms, and community gardens can co-develop programs to use nature sites not just for physical activity and growing healthy food but also for reducing loneliness and improving mental health. MINT shows how nature programming can be introduced into schools. Identifying and communicating different models for funding these nature-based practices are also needed. Finally, understanding barriers to people's access and engagement with nature and how to overcome them will be critical for success.
Organizations like the National Academy for Social Prescribing in United Kingdom (n.d.), Social Prescribing USA (2022), and the Global Social Prescribing Alliance (2022) support and publish research, gather data on social prescribing practices, and share this information to improve services. There needs to be outreach to schools of medicine, public health, clinical psychology, social work, parks and recreation, landscape design, urban planning, and public policy to promote the role of access and engagement with nature as an important social determinant of health. Introducing nature-based prescribing and programming to doctors, nurses, counselors, and social workers, while they are doing clinical training, will enable them to deliver these services. More work needs to be done so the diversity and location of nature prescribing and programming initiatives can be tracked and promoted in order for potential participants to find these services.
The comparisons in this article are not meant to show that one model—nature prescribing or nature programming—is better. Rather, the goal is to identify where each practice fits into a holistic approach to population health. As the opening of this article noted, population health is about more than just health care. Research on social determinants of health shows that investments in community resources such as education, housing, and public green space have a more significant effect on health and well-being than medical care (Woolf, 2017, 2019). Parks and other natural areas should be considered public health resources just as much as clean air and water, lead-free gasoline and paint, and safe work environments. Tree-lined streets, local parks, green schoolyards and childcare yards, and green hospital grounds are part of the social infrastructure that improves a community's health (Nieuwenhuijsen, 2021).
Research shows that access to time in nature is a determinant of health that merits a high level of recognition and support. The network presented in this article suggests how health care doctors and staff, other care professionals, and community partners can collaborate to make the healing properties of nature available for people with different levels of need. Although current barriers to the widespread adoption of nature prescribing and nature programming need to be overcome, creative initiatives are happening. Nature, in all its various forms, can be a space where professionals of all backgrounds come together to imagine a future with better health, better care, and better outcomes for everyone.
Footnotes
Acknowledgments
We are grateful for the helpful suggestions of this article's reviewers, especially the suggestion for a better version of the network model in ![]() . This article was developed out of a 2023 symposium on “Nature-based Social Prescribing and Programming,” co-organized by the Community Engagement, Design and Research Center, and the Renée Crown Wellness Institute at the University of Colorado Boulder. We express appreciation for the event organizers and its many co-sponsors.
. This article was developed out of a 2023 symposium on “Nature-based Social Prescribing and Programming,” co-organized by the Community Engagement, Design and Research Center, and the Renée Crown Wellness Institute at the University of Colorado Boulder. We express appreciation for the event organizers and its many co-sponsors.
Authors' Contributions
This article was coordinated by the first author with all co-authors writing specific sections, as well as reviewing and editing the entire article. W.T. and L.C. were responsible for writing the original draft of the article. W.T., A.L.S., J.S.L., and N.R. wrote the sections related to specific programs: W.T. wrote about the Pathways program, A.L.S. contributed the section on the MINT program, J.S.L. wrote about RECETAS, and N.R. wrote the section about SHINE. L.C. drafted the Introduction, and W.T. and L.C. prepared the Tables and Figure and drafted the Discussion. All authors read and approved the final article.
Author Disclosure Statement
No potential conflict of interests was reported by the authors.
Funding Information
W.T. acknowledges support from the donors who make the work of The Trauma Foundation possible, including the Clare Rose Foundation, Legler Benbough Foundation, Healthquest Foundation, Treeline Foundation, Leonard Family Foundation, and REI Cooperative Action Fund. J.S.L. acknowledges support by the European Union's Horizon 2020 Research and Innovation Programme under grant agreement no. 945095 (J.S.L., PI), the Research Scholars Health Equity Grant (130091-RSG-16-169-01-CPPB) from the American Cancer Society (J.S.L., PI), the University of Colorado Cancer Centre and the University of Colorado Boulder (J.S.L., PI), and the Renee Crown Wellness Institute at the University of Colorado, Boulder Seed Grant Program (No. 13404887) (J.S.L., PI). A.L.S. acknowledges Graduate Student Research Grants from the University of Colorado, Boulder Environmental Studies Department; and the Renee Crown Wellness Institute at the University of Colorado, Boulder Seed Grant Program (No. 13404887) (J.S.L., PI).