
Abstract
Research on common factors in therapy largely focuses on qualities in the therapist, relationship, or client, with little attention to the meaning of the physical environment. This study contributes to the literature on common factors, aiming for a qualitative in-depth analysis of the ways place, nature, and natural materials affect therapy with hospitalized chronically ill children. The study compares the experience of therapy in the Outdoor Care Retreat (OCR)—an architect-designed cabin in a natural setting behind the Oslo University Hospital in Norway—with therapy in a traditional hospital setting. The findings are based on two group interviews with seven leaders, six individual interviews with therapists (psychologists, social workers, and medical doctors), and four individual interviews with parents of hospitalized chronically ill children. The qualitative data were analyzed according to reflexive thematic analysis and categorized into eight main themes. The (1) affordances of the OCR positively influenced the therapy. The analysis yielded examples of positive influence from the natural setting and materials on both child and therapist, in terms of (2) natural bodily reactions, (3) multifaceted role activation, (4) situations of opportunities, (5) restorative emotional reactions, (6) stronger alliance, and (7) valuable expectations. The subthemes demonstrate which mechanisms were in play, and how these contribute to (8) therapeutic flow in a holding environment. The case study demonstrates the value of considering place and nature for therapy with children. A model of the meaning of the physical environment in therapy is proposed, to be tested in further research.
Introduction
One component in therapy that has received little attention is the physical setting. Office or hospital environments, for instance, may prompt associations that will influence therapy and treatment in different ways. The patients' perceptions of the physical environment include evaluations of their own role, value, and safety in a particular setting. Studies show that these types of associations affect patients' comfort and expectations regarding the quality of the care they will receive (Devlin, 2008; Noble & Devlin, 2021). A sterile cold room may not be the best option for therapy—especially not for therapy with children.
Furthermore, hospital settings tend to elicit fear in children (Coyne, 2006; Gaminiesfahani, Lozanovska, & Tucker, 2020; Salmela, Salanterä, & Aronen, 2009), and this may influence their contact and alliance with the therapist and hospital staff. A child entering a hospital typically brings with them expectations and some degree of bodily stress; whether these expectations are positive or negative, and the stress is enhanced or reduced, will influence their alliance with the medical staff. This in turn will have an impact on the therapy and the child's ability to handle medical treatment (Kozlowska, Scher, & Helgeland, 2020).
Research gap concerning physical context as a common factor in therapy
The effect of psychotherapy has traditionally been seen as a combination of unique factors and nonspecific common factors. Research on common factors in therapy has mainly focused on qualities in the therapist, the relationship, or the patient (Finsrud et al., 2022; Lin, 2016; Wampold, 2015), but little attention has been given to the meaning of the physical environment. Safe healing settings may elicit positive expectations for therapy (Frank & Frank, 1991; Noble & Devlin, 2021). Accordingly, a healing context and the meaning attributed by patients and therapists to the context might affect the therapeutic outcome. The use of healing contexts as mental conceptions in trauma therapy illustrates the power of the physical environment for creating a good safe place for therapy (Gerge, 2018).
Research combining clinical and environmental psychology is limited. According to Jackson (2018), there are few studies on the effect of the physical indoor environment on therapy, and in practice, and rarely is the selection of interiors in therapy offices evidence based. However, some studies suggest that patients prefer comfortable and familiar or homey settings, as this helps them feel safer (Jones, 2020; Nasar & Devlin, 2011; Sander & Lehmann, 2019).
Therapy is also typically conducted indoors, despite the growing body of research on the positive effects of outdoor-/adventure-/nature-based therapy (Bragg & Atkins, 2016; Cooley, Jones, Kurtz, & Robertson, 2020; Fernee, Gabrielsen, Andersen, & Mesel, 2020; Gabrielsen et al., 2019; Jong et al., 2021; Naor & Mayseless, 2021). A literature review by Cooley et al. (2020) concludes that nature's enrichments to therapy are mutuality, freedom, holism, interconnectedness, and practitioner well-being.
However, research on nature-based therapy often concerns therapy characterized by outdoor play and risk (Harper, Rose, & Segal, 2019), as well as longer stays in the wilderness, away from everyday life. This type of research is seldom related to a generic focus on the meaning of the place for therapy or linking findings to common factors in therapy. Thus, there is a gap in the literature with regard to explaining precisely how place/therapeutic settings influence therapeutic interventions (Harper, Fernee, & Gabrielsen, 2021; Johnsen, Lindheim, & Hauge, 2022).
Aim and definitions
This article presents the results of a qualitative interview-based study of the Outdoor Care Retreat (OCR) at Oslo University Hospital (OUS). The OCR is an architect-designed cabin outside the hospital buildings, near the forest (see A case study of the OCR). It is mostly used for therapy with children with serious somatic diseases, for integrated course treatment and recovery. These children are often too ill to leave the hospital area, so the OCR was developed to give them nature experiences despite being hospitalized.
Staff, patients, and relatives have reported that the cabin rapidly became a preferred space for therapy (Lindheim, Johnsen, Hauge, & Diseth, 2020), and this is the first systematic research study of their experiences: What is the experience of the meaning of the physical environment in therapy in the OCR compared to traditional hospital environments? A further aim of the study was to propose a general theoretical model of the meaning of the physical environment in child therapy.
The physical setting in this study comprised both nature and architecture. Nature and architecture are often treated as contradictions; however, architecture may consist of natural elements and biophilic design (Kellert & Wilson, 1995). Biophilic design is a framework for including the satisfying experience of nature in the built environment, for example, through organic forms, natural materials, and vegetation (Kellert & Calabrese, 2015). Architecture and nature may, therefore, be intertwined: The OCR is a good example of this. The case study of the OCR includes both its architecture and its outdoor surroundings.
In this study, psychotherapy is broadly defined as the utilization of psychological methods in the treatment of psychological challenges (Sourkes, Kazak, & Wiener, 2015). Therapy with hospitalized children aims to help them cope with somatic illness, stress, and anxiety, and preparation for medical procedures. The case of the OCR may deepen our understanding of how best to take advantage of the OCR and similar natural settings in therapy.
The meaning of nature and place
Bodily, emotional, and cognitive effects of nature and natural environments
Several studies demonstrate the positive effects of nature on therapy and treatment (for reviews, see Bragg & Atkins, 2016; Cooley et al., 2020). The bodily effect of nature on regulative processes can be measured physically through reduced pain, heart rate, blood pressure, and cortisol level (Malenbaum, Keefe, Williams, Ulrich, & Somers, 2008; van den Berg, Koole, & van der Wulp, 2003).
Nature and biophilic design affect emotions, in terms of psychological restoration, increased mental well-being, and reduction in depression, anxiety, and stress (Bakir-Demir, Berument, & Akkaya, 2021; Bragg & Atkins, 2016; McMahan & Estes, 2015). Studies show that people actively seek nature to regulate emotions (Hartig, Kaiser, & Strumse, 2007; Korpela et al., 2018). Johnsen (2011) states that nature has a direct regulative effect on emotions, and likely also an indirect effect through cognitive processes.
Place attachment, favorite places, and trauma therapy
Morgan (2010) describes how attachment to primary caregivers gradually expands to include attachment to home and place. Place attachment is defined as the bonding between individuals and their meaningful environments, organized along three dimensions: person, place, and processes (Scannell & Gifford, 2010). The process dimension is relevant for therapy, with regard to how the place supports safety and emotion regulation (Korpela, 2012). Place attachment to natural places is more easily developed (Basu, Hashimoto, & Dasgupta, 2020; Scannell & Gifford, 2010), and environments and objects that remind children of safe and happy places to which they are attached may lead to feelings of safety.
Safety is important for creating an alliance with the client (Allison & Rossouw, 2013), and in this way, the setting may influence emotional security and therapy. Korpela, Kyttä, and Hartig (2002) describe how children use their favorite places to regulate self and emotions. In trauma treatment, an inner safe place (Gerge, 2018) is often used as a basis for therapy, hypnosis, eye movement desensitization, and reprocessing (Shapiro, 2014).
Symbolism and creativity in nature
The concept of affordances (Gibson, 1986) relates to what the physical environment offers to humans. In the built environment, objects and buildings often have defined purposes; however, in nature, the interpretation and use of the environment are more ambiguous and thus allow more creativity (Harper et al., 2019). Research shows that humans are more creative in nature (Palanica, Lyons, Cooper, Lee, & Fossat, 2019; van Rompay & Jol, 2016)—as such, nature may influence a therapist's ability to capture a child's interests and curiosity. The therapists' creativity and use of metaphors may help widen and deepen stories about the child (White & Epson, 1990)—in this case, developing identity as something broader than the illness they are fighting.
Naor and Mayseless (2021) found that metaphors in nature are powerful because they are real and involve all senses, and because the client is physically in the metaphor. This supports learning and change processes because clients semantically relate cognition and bodily involvement (Corazon, Schilhab, & Stigsdotter, 2011).
Methods
A case study of the OCR
A qualitative interview-based study was chosen for the purpose of gaining in-depth knowledge about the meaning of place in child therapy, with nature and natural materials in a specific setting. The OCR is a unique case, and the perspectives of different types of users constitute embedded cases (Yin, 2014). As this study aimed for both internal generalization within the case and external generalization to other similar cases (Braun & Clarke, 2022; Maxwell, 2020), the context of the OCR is detailed hereunder.
The OCR was developed in cooperation between the Department of Child and Adolescent Mental Health at OUS, the Outdoor Care Retreat Foundation (friluftssykehuset.no), and the architecture firm Snøhetta in 2018. The goal was to develop a good peaceful space in nature for patients and their families (Lindheim et al., 2020). The OCR is located close to the hospital and the forest (see Fig. 1). It was constructed using wooden materials, with crooked walls meant to resemble a treehouse built by children. Inside the cabin, there are large pillows in different colors that can be used for relaxation or play (see Figs. 2 and 3).

Exterior: photograph by Maren Lindheim.

Therapy room: photograph by Øystein Horgmo.

Family room: photograph by Åshild Hauge.
The cabin also contains other objects meant for play and activities, made of natural materials (e.g., leather, shells, and rocks). Equipment such as fishing rods and hammocks are available for use. Large windows look out on a small stream and the forest and are meant to invite users to explore the surroundings. Outside, there is a fireplace (see Fig. 4), and a small bridge crossing the stream.

Fireplace in winter: photograph by Øystein Horgmo.
In contrast, the setting of the Department of Child and Adolescent Mental Health in the hospital is characterized by a traditional hospital interior, with white walls and long corridors. There are areas for children to play, and family areas, and it is decorated with art. Nevertheless, the environment might not be considered homey, and might also be experienced as noisy and chaotic.
When referring to the OCR in this study, we mean both the indoor environment, the exterior, and the outdoor area in connection to the cabin, with the fireplace and the small stream nearby. These areas are used interchangeably when patients and staff are in the OCR.
Reflexive thematic analysis
The data consist of three separate interview studies, following an interpretative phenomenological approach (IPA) (Smith & Shinebourne, 2012). IPA is an approach “dedicated to the exploration of personal meaning and lived experience,” and “how participants are making sense of their personal and social world” (Smith & Osborn, 2015, p. 25). In line with this, the goal for these studies was to explore how the participants made sense of their experience of the OCR. To reanalyze the data as a whole, however, we employed reflexive thematic analysis.
The reasons for this are threefold: (1) more data were gathered than in a typical IPA study; (2) the different groups of participants were not the homogeneous sample typically found in IPA research; and (3) the analytic purpose was to explore patterns across the data sets, rather than unique features (Braun & Clarke, 2021). Thematic analysis is a family of flexible methods for analyzing patterns of meaning in qualitative data, and the reflexive approach implies “a disciplined practice of critically interrogating what we do, how and why we do it, and the impacts and influences of this on our research” (Braun & Clarke, 2022, p. 5). The reflexive thematic analysis was conducted within a contextualist epistemology, where the themes are seen as coproduced by the researcher and the interview participants (Braun & Clarke, 2022).
Ethics and reflexivity
The data collection was approved by the Norwegian Center for Research Data, and their guidelines for securing personal data were followed. All participants provided written informed consent before the study.
According to Braun and Clarke (2022), reflexive thematic analysis highlights the researcher's active role in knowledge production, and subjectivity is valued; the authors highlight that researchers must be aware of how their background influences their interpretation of data. In this study, the researchers were familiar with and trained in environmental psychology, and, therefore, knew the effect of nature on well-being and health. On the positive side, this may have deepened the understanding of the subject matter; on the negative side, it might have led to an exaggeration of the meaning of nature.
Since one of the authors of this article is a therapist and leader at the OCR, the external researchers conducted most of the data analysis. There were also several rounds of discussion around whether personal hopes for positive effects of the OCR could have exaggerated the positive results. To counteract results in favor of nature, we checked for alternative explanations.
Participants and interviews
To explore the OCR from different perspectives, this study is based on three groups of participants, (1) focus group interviews with seven leaders, (2) individual interviews with six therapists using the OCR, and (3) individual interviews with four parents of the patients. There were 17 participants in total. They were recruited through the management of the OCR. All leaders of departments with child and adolescent patients at the hospital were recruited for the focus-group interviews. They had not taken part in developing the OCR and had no interest in its success. The leader interviews were especially important for understanding the hospital context.
All therapists at the Department of Child and Adolescent mental health using the OCR in therapy were recruited for individual interviews (the other staff in this department do not work in ways that make it natural to use the OCR). Furthermore, these therapists were asked to suggest families that were in a life situation capable of research participation despite their child being seriously ill. Families with dying children were not included. Eight families were asked, and four of these said yes.
The patient population for this hospital reflects the Norwegian population, including minority groups with different cultural backgrounds. However, in this case, the therapists and parents interviewed were ethnically Norwegian.
The children will be interviewed in the next phase of the project. The advantage of the selected informant groups is their meta perspective, and their ability to compare different treatment settings. See Table 1 for an overview of the participants.
Participants and Interviews
OCR, Outdoor Care Retreat.
We developed semistructured interview guides with broad open-ended questions, but with keywords to use if the participants did not spontaneously speak about relevant topics. All interviews were mainly about the experience and use of the cabin. The interview guide for therapists was more focused on how they did therapy/the experience of therapy in the different settings. Both therapists and parents were asked to compare the OCR with the traditional hospital setting.
The focus group interviews were conducted at the OCR. Owing to the coronavirus pandemic, some of the interviews with therapists and parents were conducted online. Most individual interviews took ∼1 h, and the group interviews took 1.5 h. The interviews were conducted and analyzed in Norwegian. The interviews were audio recorded and transcribed by the same individuals who conducted the interviews. The translation of the quotes was done by a professional translator.
Analysis and methodological integrity
The results were analyzed according to Braun and Clarke's (2022) six steps for data analysis in reflexive thematic analysis: familiarization with the data, data coding, initial theme generation, theme development and review, theme refining, defining and naming, and writing up the analysis. The analysis was inductive, driven by the data content. The coding and theme development were done in MAXQDA program for data analysis (VERBI Software, 2021). The categorization and naming of themes were discussed in several meetings between the researchers. To increase transparency, quotes from participants are used to exemplify the main themes.
The interviews with the leaders were used mostly for background information. The core themes in the analysis are mainly from the interviews with the therapists and parents. The main themes were supported by a majority of these participants, and all subthemes were supported by at least two participants.
Support for the results was supplemented through a feedback meeting on November 21, 2022, with the staff at the department of the interviewed therapists. They agreed with the results and the categorization. However, they were concerned about the description of the therapeutic work in the traditional hospital environments coming out too negatively, even if it had been said in this way in the interviews. We, therefore, jointly decided to grade the adjectives in the subthemes' column of the description of therapy in the traditional hospital setting. We also jointly decided to point out that these subthemes are relative to the OCR and relate to the physical environment.
Results
Table and figures of findings
The analysis resulted in eight main themes about the meaning of the OCR in therapy with children. We were specifically interested in the dialectical process of juxtaposing the traditional environment with the OCR, as this was of particular interest for theory building. Most of the participants (especially therapists and parents) compared the OCR with the traditional hospital setting when describing their experience—both when asked to do so and unbidden. The way they described the differences compared with the traditional hospital settings emphasized the benefits of the OCR. The results are, therefore, presented as dichotomies.
Another important insight that emerged, and that affected how the categories are presented, was that the OCR influenced leaders, therapists, children, and parents in many similar ways. Therefore, instead of separating findings between participant groups, we chose to combine them. The table specifies where the influence from the OCR was mainly on the children. See Table 2 for the categorization of the themes and subthemes, and Figure 5 for a visual presentation of the main themes.
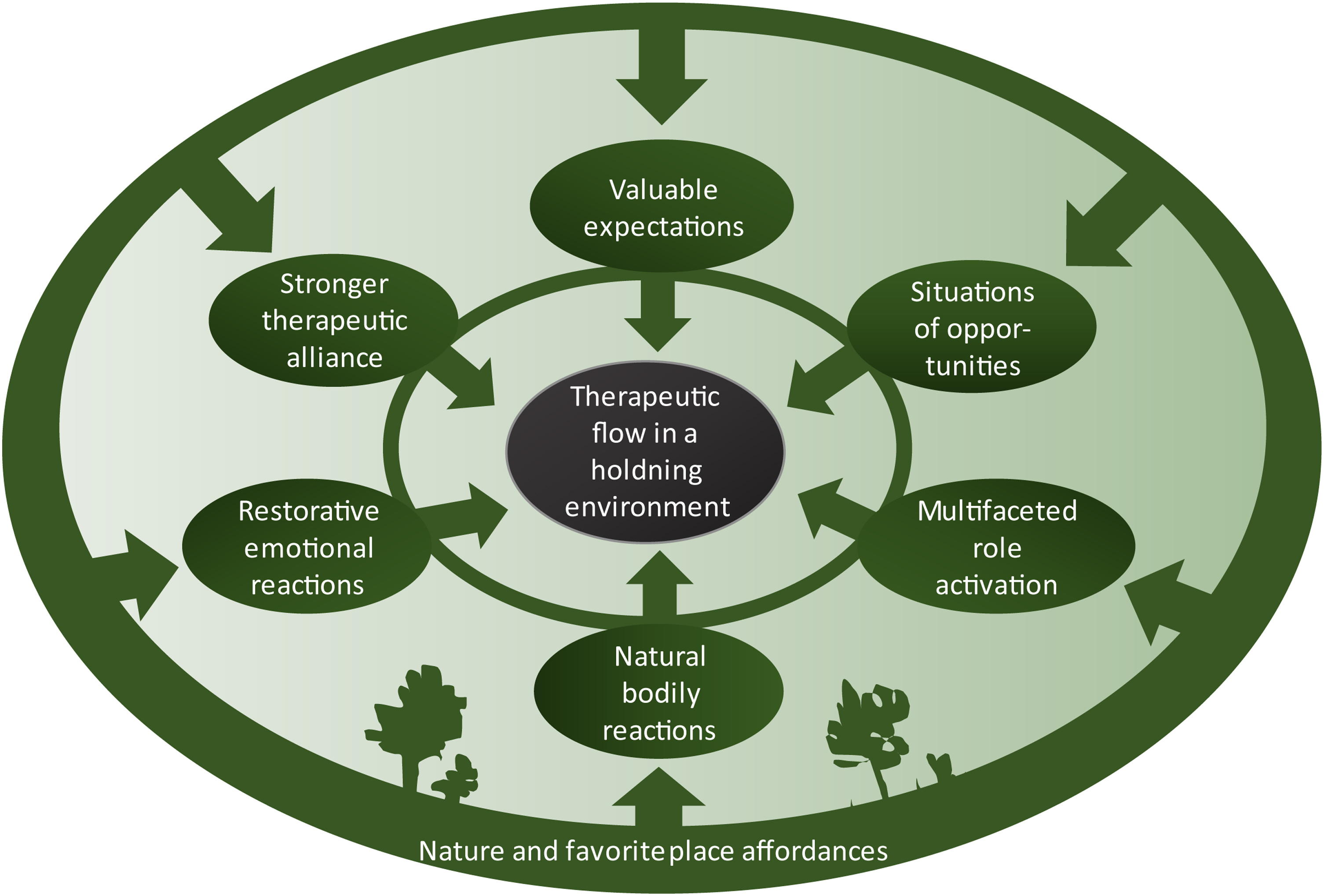
How nature and favorite place affordances influence therapy with children.
Categorization of Themes
Presentation of themes
When presenting the themes in the following sections, the main themes are used as headings, and the subthemes for the meaning of OCR for therapy with children are emphasized in italics.
Nature and favorite place affordances
This theme covers aspects of what the physical environment offers humans, in line with Gibson's (1986) definition of affordance. All participants describe the OCR as offering nature and natural materials in contrast to the traditional hospital setting. The nature surroundings further provide a diversity of activities in contrast to a patient room or an office. When compared with a playroom in the hospital, some therapists say that a child often becomes overwhelmed and stressed by all the toys, making it difficult to connect with the child.
Nature and cabin surroundings, in contrast, seem to offer a diversity in activities in a way that does not distract children from human contact. In addition, the setting offers flexibility for interaction. The parents may be nearby or in the background once the child feels safe enough, and the participants describe this as a more natural process in the OCR surroundings. The participants also describe the OCR as offering a favorite place (Korpela et al., 2002) for most visitors, in contrast to the traditional hospital setting that is typically a place where people, especially children, do not want to be. A parent described the child at the OCR this way:
In the beginning he liked to sit on the floor, for example, and I think that gave him a sort of sense of security. And it was possible to put cushions on the floor and put on slippers and wool socks, and this gave a bit of the atmosphere of being in a cabin. So, his favourite place was … well, first it was on the floor, or in that little tent there. (Parent 2)
Therapists and parents also describe the hospital setting as full of negative distractions (e.g., nurses and doctors coming in for tests, and noise from medical equipment). The OCR, by contrast, is peaceful, with no disturbances, and although there are distractions, these are positive distractions, consisting of nature views or interacting with nature—these distractions offer relieving breaks from therapeutic work or a focus on illness.
Natural bodily reactions
This theme encompasses aspects that relate to bodily reactions to the OCR, compared with the hospital setting. The participants describe how both therapists and children become more active in the OCR and the surrounding nature, in contrast to the hospital setting where both therapist and client are more bodily passive. They describe how children in the hospital setting are tense. The affordances for activities in nature and natural surroundings, however, seem to lead to more relaxed children with more open body language. The children's bodily energy level also seems to vary, from relaxed to vital, in the OCR. In the traditional hospital setting, the children's energy level is more controlled, in accordance with norms or expectations. This means that the bodily energy level in the outdoor setting is freer and more natural.
Well, children are creative by nature, and like to be in motion, so it (the OCR) is really a setting that is more natural for most children. The fact that they are allowed to be active and be the way they are accustomed to be with their bodies. It isn't natural for children to sit down on a chair and talk. (…) So, what I have found is that when things are deadlocked within them, they are often loosened up in another way when we go outdoors. (Therapist 4)
Multifaceted role activation/positive identity
This theme comprises the roles or identities that the settings activate in the therapeutic situation. In the hospital setting, the therapists often experience the challenge that the therapist–child relationship seems like a subject–object relationship, where a child is an object under medical treatment. The OCR is described as a setting that through its affordances makes the client and therapist more equal. This relates to how the natural setting offers a shift in focus onto what is normal and healthy about the child. In addition, the more personal sides of the therapist become activated.
Inside the cabin, I know that she (hospitalized child) makes many of her own decisions too. And then she shows who she really is. That's what she thinks is really fun, that she shows who she really is and not that scared person, the girl who is afraid of needles. (Parent 1)
Some of the therapists use the term multifaceted relationship to describe their bond with the child in the OCR, pointing to what many of the therapists and parents describe: In the hospital setting, the therapist gets to know the child in only one way, and with the illness in focus, but in the OCR the therapist gets to know the child through a diversity of activities, with an additional focus on the healthy aspects of the child.
Situations of opportunities
This theme captures the differing situational aspects between the two therapy settings. Both parents and therapists describe the setting in the OCR as more like everyday life situations, and a break from the clinical life in the hospital. The parents in particular focus on how the OCR is a situation where the child is in control, in contrast to the hospital, where the child is a patient who is controlled and must accept all medical procedures. The OCR provides the foundation for a creative and playful setting—one that is sometimes even magical.
Something happens with the young people, it (the OCR) is a special place where some quite magical things happen. Maybe they become a bit more secure there and able to talk a little about particularly important things. (…) I think it's so much easier to create that kind of holiday feeling or a bit of magic out there. (Therapist 1)
Restorative emotional reactions
This theme describes how being at the OCR creates positive emotions that contributes to restorative processes. Emotions are often understood as reactions to events that are evaluated as meaningful, and consist of physiological, behavioral, and experiential reactions (Frijda, 1988; Gross, 1998). All leaders, therapists, and parents describe the OCR as a place that gives them good experiences/joy. The opposite is often the case for hospitalized children, who experience many difficult emotions in the hospital, which in turn create fear. Parents and therapist observe happy children who feel safe in the OCR. All participants describe restorative experiences in the OCR, and this is often linked to a sensory impression of the nature: the view through the large window, the wood interior, and the outdoor surroundings.
You see it a lot in the expressions on their faces, I think. They are a lot more kind of open (in the OCR). I often think that when you meet them inside the hospital it's kind of like this….they're watchful, guarded. They are sort of sceptical about who you are, what you're going to do, and why you're there, and…. That scepticism disappears much faster when you're outdoors. (Therapists 3)
Another central theme to which the leaders, therapists, and parents refer is the sense of mastery that the OCR surroundings create in the child, when the child is encouraged to show skills related to the outdoor areas. This takes the focus off of all the things the child cannot master due to illness. The therapists and parents provide many concrete examples on how children light up when demonstrating jumping, handling spiders, or making a campfire. The therapists report that they have witnessed children's feelings of pride, self-efficacy, and mastery grow in the OCR.
Stronger alliance
This theme contains aspects describing the therapeutic alliance between therapist and child (McLeod, 2011), and how it often quickly becomes stronger in the OCR compared with the traditional hospital setting. This relates to both the bond and task dimensions. First and foremost, both parents and therapists describe children as curious and aware when entering the OCR. Most of the therapists state that the OCR improves response and dialogue with the child. Many of them also report that making contact and establishing attachment happen more quickly and easily in the OCR than in the hospital setting.
I do find that they quite quickly become interested in having contact (in the OCR), and that they are happy to share what they are experiencing, and quite quickly invite me into their world of experience. (…) I think that in some way or other I am less threatening outdoors, that we are a bit more, like, on the same level. (Therapist 3)
The OCR also facilitates more natural and easier contact with the relatives when the family can join outdoor activities or be nearby when the child is talking with the therapist. The therapists describe the OCR as a setting that often leads to a common project between therapist and child, whether making an indoor pillow tower or an outdoor campfire. This common project creates a stronger experience of having done something together than what occurs during therapy in a traditional setting.
Valuable expectations
This theme describes how good hospital memories form expectations for new meetings, therapy, and hospital visits. Therapy outcomes are found to be influenced by expectations (Finsrud et al., 2022). Leaders, parents, and therapists suggest and state that children look forward to being back in the OCR, instead of dreading being in the hospital. Therapists and parents also highlight how the children describe positive memories from the OCR, and that these memories make their hospital stay easier.
And there are often children I meet after an interval of perhaps six months or a year, and of course there is the question of ‘what do they remember?’ (…) Of course I remember (the OCR) ‘shall we stand up, shall we go outside, shall we go out to the cabin this time too?’ That produces a completely different alliance and connection to each other. At the same time, I think that what you remember with your body, that becomes more ingrained. (Therapists 6)
Therapeutic flow in a holding environment
Therapeutic flow covers how many sides of the therapeutic work (Sourkes et al., 2015) are described in more positive terms in relation to the OCR compared with the traditional setting. The OCR creates a holding environment, in the sense that it may contribute to a wider and deeper psychosocial context for therapy, where the totality of a child is welcomed. This category was also the main focus of this study, with the other categories laying a foundation for understanding how the physical setting influences therapeutic work. An oft-referred-to topic in the interviews with therapists is how the OCR offers an external focus.
They describe how, in a therapeutic hospital setting, the child is often quite self-conscious and sits opposite the therapist, without an easy way to rest with a shared external focus. The external focus in the OCR is important for both child and therapist, consisting either of a view of nature or being engaged in nature activities together—without looking directly at each other. This relates to the affordances of the OCR setting, regarding the positive distraction offered by the view and the diversity of available activities. Both parents and therapists state that it seems easier to motivate the child for therapy in the OCR, and this may be especially related to the playfulness of the situation.
The therapists also state that they feel more creative as therapists and are inspired by the nature to use nature metaphors. In both traditional hospital settings and in the OCR, the therapists try to follow the child in therapy, letting them take the lead; however, many state that it is easier to do so in the OCR, when the child feels more in control and masterful. Both therapists and parents have witnessed that access to difficult topics seems to come more easily in the OCR. In addition, they experience that emotion regulation when talking about difficult things occurs more easily in nature or in the OCR.
Here (in the OCR) there has been real progress and she had been herself, been able to express herself more and talk about what happened, I see it's easier. Not all that easy, but she asks more questions about what happened to her; before she was repressed and didn't want to talk about everything. So, I see that it comes easier now, when she is in that cabin there. (Parents 1)
Discussion
The meaning of the physical environment in therapy
This study adds important perspectives to the literature on common factors influencing therapy (Finsrud et al., 2022; Lin, 2016), which has traditionally overlooked the physical setting. Study findings demonstrate how the physical environment—through its affordances—influences these common factors. The perceived client and therapist characteristics (Lin, 2016) are especially influenced through what is captured by the “situations of opportunity” and “role/identity” themes. The OCR makes the situation and the roles more equal, natural, and playful, thereby altering how the client and therapist see each other.
The findings also exemplify how the therapy setting may affect the common factors identified by Finsrud et al. (2022) as influencing therapy: specifically, patient expectations, goal consensus, and confidence in the therapist and treatment. Indeed, the themes “natural bodily reactions,” “restorative emotional reactions,” “stronger alliance,” and “positive expectations” illustrate how the physical environment creates a different basis for feeling safe and having confidence in one's treatment and therapist.
Cultivating a safe space for exploring issues and developing oneself is essential to a positive therapeutic outcome (Gerge, 2018). Theories about place attachment and favorite places explain this through humans' need for safe places and places that make them feel good, for emotion regulation (Korpela et al., 2002; McGuinnes, 2011; Shapiro, 2014). Our findings show that when the physical environment supports a safe grounding, it takes less time for the therapist to establish an alliance and to broach topics that are difficult to talk about. Why and how might nature and biophilic design lead to this?
Nature offers rich affordances for emotion regulation (see e.g., Johnsen, 2011) and mastering. The child is more in control and appears to be able to rely more on internalized abilities. It seems as though these abilities are not decoupled from the context in children, and that children may rely more on the emotional affordances in the environment to achieve mastery over various issues. Perhaps the development of internal working models (e.g., object relations) is tied to the context and later generalized. Nature environments may be more conducive to constructing a coherent narrative and developing tools and abilities.
These environments also yield opportunities for alliance building through tasks and goals. Moreover, being in an environment that contains the very metaphor that the therapist wants to explore makes the therapeutic intervention less reliant upon verbal behavior. The setting invites both cognition and bodily involvement, thereby increasing learning and change (Corazon et al., 2011).
This qualitative case study may be used to propose a model of how the physical environment influences therapeutic work. Figure 6 is a neutralized version of the main themes from this study, illustrating six key ways that the affordances in a physical setting influence therapeutic work with children.
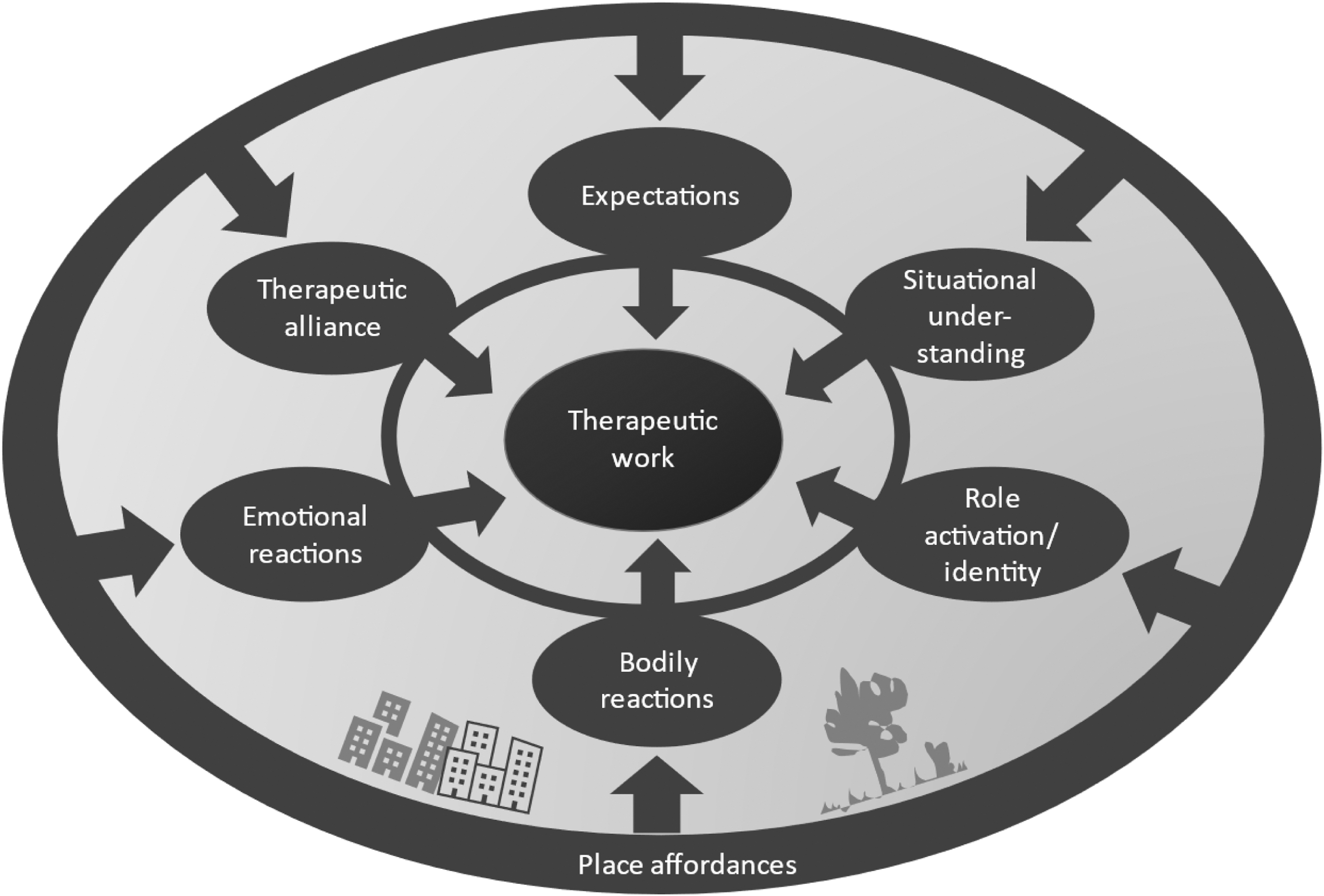
How the physical environment influences therapy with children.
The subthemes listed in Table 2, and described in the Results section, explain in detail how both positive and negative affordances in the physical environment influence therapy. Examples include how undertaking an activity in nature facilitates contact and alliance more effortlessly than when sitting opposed to each other in a traditional hospital setting. The six main categories also influence each other, as illustrated by the inner circle in Figures 5 and 6.
The place/setting influences the child's and therapist's body and emotions, which further affects their understanding of the situation and the way they see each other. These components influence the alliance between child and therapist, and the positive experiences create valuable expectations for therapy. The starting point of a positive circle like this may be natural surroundings and biophilic design.
Limitations and further research
Case studies on similar cabins and natural environments should be conducted for comparison. Nature has a special place in Western and Scandinavian culture, and the expectations of seeing nature as restorative may have colored the interpretation. We, therefore, suggest further research in which “therapy in a different place” entails something other than therapy in natural surroundings.
Lack of cultural diversity among the participants in the study is a limitation. Different sociocultural communities are likely to have different relationships to nature and outdoor spaces, and ethnicity and gender form people's experience of being outdoor (Doherty et al., 2022). We recommend that the presented framework is further studied within other cultures.
The study had therapist participants who actively used the OCR, and valuable perspectives could also come from therapists who did not use it; however, this would imply a research focus on barriers for use more than experiences with use.
Would nature offer the same benefits without the cabin? In this study, we view the cabin as constituting a gathering place in (and looking out on) nature that can be used in all weather (especially relevant in Nordic countries), thereby facilitating the nature experience for ill patients. It can be discussed whether the OCR's benefits are linked to simply being removed from the hospital and thus the risk of painful treatments. However, the cabin is part of the hospital, while also qualitatively different from the traditional hospital setting.
This study was conducted with a focus on therapists and parents' experiences of therapy with children in the OCR. Further studies should include interviews with children for a more comprehensive analysis. There is a need for a client perspective on this topic through both interviews and surveys. Analyzing videos of therapy in different settings, scoring alliance and type of conversation topics, may be conducted both through a qualitative and quantitative approach. Furthermore, there is a need for detailed research on how to actively use nature and biophilic design in therapy, especially concerning how to take the positive influence of nature indoors.
With regard to the difficulties of implementing nature and biophilic design in health care environments, the economic consequences of the benefits must be better assessed.
Transferability
Analytic generalization is based on description of contexts, and the readers' evaluation of similarities of contexts of other cases (Braun & Clarke, 2022). Study findings were generated from an extreme and unique case. The user group is particularly vulnerable, afraid (Coyne, 2006), and often deprived of opportunities to be in nature because they are seriously ill. Elements of safety are also important in child therapy outside hospital contexts, and many of the findings may be transferable to other therapeutic settings for children.
However, although children in therapy may be influenced in many of the same ways, the effects may not be as extreme for children who are free to play in nature whenever they desire. The OCR case offers an opportunity to look at the meaning of place for therapy through a lens whereby the mechanisms at play become more visible. This makes the case especially suitable for building theoretical models.
Main conclusions and implications for practice
The results show that the meanings ascribed to the physical environment appear influential for common factors in therapy. In the OCR, compared with traditional hospital environments, the affordances provided by nature and the cabin influence therapeutic work in six key ways, through how they affect bodily reactions, role activation, situational understanding, emotions, therapeutic alliance, and expectations. Accordingly, to the extent that therapeutic processes rely on these aspects, there might be a significant influence on the outcome of the therapy.
With such encouraging results, why are physical environments not more actively used—and deliberately chosen—for therapy? As stated, there is little focus and research on the meaning of the physical environment in therapy (Devlin & Arneil, 2003; Jackson, 2018). Environmental psychology is seldom combined with clinical psychology, and the growing body of research on adventure- and nature-based therapy (Cooley et al., 2020) is seldom taken into account in traditional therapeutic practice, particularly concerning indoor therapy.
The practical implications of the results of this study might point therapists toward being more aware that place matters for therapy, and to try therapy in a different place (e.g., outdoor therapy) and/or implement biophilic design in indoor health care environments. Examples on this may be furniture and interior in natural materials, large windows with nature view, or photographs of nature as wallpaper or pictures. Most hospitals are situated in urban settings, with no surrounding nature, however, roof gardens may provide some of the same experiences.
When presenting the findings at the department meeting for the therapists who had been interviewed, one of them put it this way, “in a hospital room you start therapy in minus, at the Outdoor care retreat you start in plus.”
Footnotes
Acknowledgments
We thank all the interviewees for contributing to this research, and the students who conducted the interviews (Berit Sinding-Larsen, Ibrar Manzoor, Kristine Lie Røtting, and Julie Dyveke Haakenstad). We also thank the editor and reviewers for their valuable comments, and colleagues and family for discussing theme names.
Authors' Contributions
Å.L.H. contributed to conceptualization, methodology, formal analysis, software, writing—original draft, and visualization. M.Ø.L. was involved in writing—review and editing, and resources. K.R. was in charge of interviewing, formal analysis, and writing—review and editing. S.Å.K.J. carried out formal analysis, writing—review and editing, and validation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.