
Abstract
Diabetic peripheral neuropathy (DPN) and periarthritis of the shoulder (PAS) are common complications in long-standing diabetes, both contributing significantly to pain, disability, and reduced quality of life. DPN, characterized by sensory, motor, and autonomic disturbances, affects up to 50%, while PAS affects 20% of those with diabetes. In this case, the integrated yoga and naturopathy (IYN) intervention has demonstrated a favorable therapeutic effect in patients with DPN and PAS. A 60-year-old woman had complaints of DPN and PAS of the left side along with neck pain radiating to the left upper limb, limited shoulder mobility, burning and pricking sensations in both feet, and depression. After inadequate results from conventional treatment, the patient sought care through a 10-day IYN intervention followed by a 3-month follow-up. Compared with the baseline, the post-assessment showed a marked reduction in the glycated hemoglobin, homeostatic model assessment of insulin resistance, fasting insulin, fasting blood sugar, and reduction in scores of visual analog scales for pain, Shoulder Pain and Disability Index, Neck Disability Index, and Patient Health Questionnaire-9, and increase in the range of motion. This case demonstrates that IYN intervention are effective in addressing both physical and mental challenges in patients with DPN and PAS. However, as this is a single case report, more studies with a larger sample size are recommended to validate the findings of the study.
Introduction
Diabetic peripheral neuropathy (DPN) and periarthritis of the shoulder (PAS) are common complications in patients with long-standing diabetes. DPN, a nerve damage caused by chronic hyperglycemia, primarily affects peripheral nerves in the feet and hands, causing sensory, motor, and autonomic disturbances. Diabetic neuropathic pain, characterized by tingling, burning, and electric shock sensations, can be moderate to severe, affecting patients’ quality of life, daily activities, and mood. It affects approximately 50% of patients with both type 1 and type 2 diabetes (T2D). 1 DPN is more prevalent in T2D patients, with 26% of youths and 42% of adults experiencing it at baseline. 2 PAS, also known as frozen shoulder or adhesive capsulitis, is a condition characterized by shoulder pain, stiffness, and functional restriction, often self-limiting and resolving within 1 to 3 years. It occurs in 2%–5% of the general population and 20% of diabetics. 3
Integrated yoga and naturopathy (IYN) intervention is a holistic, noninvasive, an indigenous Indian system of medicine using various therapeutic methods for treating various systemic disorders. 4 DPN and PAS frequently result in chronic pain and limited mobility, contributing to psychological difficulties such as depression and anxiety, which can substantially impact the quality of life. 5 Previous research has shown that IYN therapies such as hydrotherapy, mud therapy, yoga therapy, heliotherapy, fasting, acupuncture, and dietary modifications can alleviate pain, improve nerve function, and enhance the quality of life in patients with DPN. 5 Previous studies suggest that IYN such as joint loosening exercises, revulsive compresses, rope exercises, and acupuncture are shown to alleviate pain, inflammation, and stiffness caused by PAS. 3
While yoga and naturopathy have shown benefits in managing DPN and PAS separately, their combined impact on patients with both conditions remains unexplored. Hence, this case study was conducted to find the impact of IYN on glycemic control, pain, disability, mobility, and mental well-being in patients with DPN and PAS.
Patient Information
A 60-year-old woman with DPN and PAS (left) was admitted to our hospital on October 18, 2023. Over the past month, she has complained of neck pain that radiates to her left upper limb, associated with numbness and jerky movements in her left hand. She had reduced range of motion (ROM) in her left shoulder and trouble in elevating her left hand. She had a burning sensation with pricking pain in both feet for the past 3 years. She had been a known case of T2D for the past 10 years. Her father had a relevant history of DPN with diabetic foot ulcer and died due to the complications of DPN. She visited an allopathic physician, and he prescribed tablet metformin hydrochloride (500 mg) with glimepiride (2 mg) 1-0-1 and teneligliptin (20 mg) 0-0-1 for the past 5 years, capsule Pregaba-M 75 [pregabalin (75 mg) and methylcobalamine (750 mg)] 0-0-1 for past 3 years. Due to unsatisfactory results, she visited our hospital and underwent yoga and naturopathy interventions.
Clinical Findings
On physical examination, she looked depressed due to chronic pain. Pedal edema and wound scar were noted in both legs. On observation, the patient had rounded shoulder on the left side. On palpation, she had tenderness along the coracoid process and the back of the shoulder. The limited ROM is noted in flexion, abduction, and external rotation of the left shoulder, and pain was measured using the visual analog scale (VAS). She had a tingling and pricking sensation in both feet. She had limited cervical ROM, which is measured by the goniometer. Radiological findings of the magnetic resonance imaging of the left shoulder revealed periarthritis of shoulder (i.e., thickening of joint capsule, obliteration of the axillary pouch with inflammatory changes) and X-ray of the cervical spine showed degenerative changes with reduced joint space.
Timeline
The timeline of the intervention from hospital admission to follow-up is provided in Figure 1.
Diagnostic Assessments
Biochemical assessments
Biochemical investigations including glycated hemoglobin (HbA1c), homeostatic model assessment of insulin resistance (HOMA-IR), fasting insulin, and fasting blood sugar (FBS) were assessed in the standard private laboratory.
HOMA-IR was calculated by using the following formula: HOMA-IR = (fasting glucose [mg/dL] × fasting insulin [mU/L]/405). 6
VAS
It is used to evaluate the patient’s overall pain intensity of all the joints on a scale 0–10, where 0 indicates no pain and 10 indicates the worst pain. The patient was asked to mark a point on the scale to indicate her pain intensity. 7
ROM
ROM of left shoulder assessed by using goniometer.
Neck Disability Index score
It is a 10-item self-reported questionnaire used to assess the impact of neck pain on daily activities, with a total score ranging from 0 to 50, with scores indicating no disability, mild, moderate, severe, and complete disability. 8
Shoulder Pain and Disability Index
It is a self-reported questionnaire that evaluates shoulder pain (five questions) and disability (eight questions) across two areas: pain and functional activities. Responses are given on a 0–10 scale, with 0 indicating no pain or difficulty and 10 representing the worst pain or greatest difficulty requiring help. The scores from both sections are averaged to produce a final score that reflects the individual’s overall level of pain and disability. 9
Patient Health Questionnaire-9
It is the depression module, which is used to monitor depression severity and treatment response using scores ranging from 5 to 20, with scores indicating mild, moderate, moderately severe, and severe depression. 10
Therapeutic Intervention
The patient underwent the following yoga and naturopathy-based lifestyle intervention: (i) Customized yoga protocol (30 min/session, twice a day) includes asanas, pranayama, and relaxation techniques; (ii) plant-based raw diet (approximately 600–650 Kcal per day), which includes seasonal fresh fruits, vegetables, sprouts, and juices; (iii) massage, including full body massage and partial massage with peppermint oil; (iv) hydrotherapy: enema, revulsive compress, revulsive foot bath, cold leg pack, cold hip bath, gastro-hepatic pack, and steam bath; (v) mud therapy: mud pack to the abdomen and eyes, and full mud bath; (vi) heliotherapy: plantain leaf bath; (vii) acupuncture and reflexology to both soles; (viii) physiotherapy: Spencer’s technique to left shoulder, pendular and ladder exercise, and median and ulnar nerve stretches; (ix) electrotherapy: wax and transcutaneous electrical nerve stimulation to the left shoulder. The details of the yoga and naturopathy intervention given to the patient are provided in Table 1.
Details of the Yoga and Naturopathy Intervention Given to the Patient
Follow-up and Outcome
After 10 days of supervised intervention at the hospital, the patient was advised to visit the outpatient department for a regular follow-up for 3 months. During the follow-up, she was instructed to adhere to the specified diet, 1 h of yoga, a cold hip bath, and cold leg packs. According to the patient’s account of the follow-up, her symptoms have improved and observed sustained benefits after three months of regular follow-up.
The findings of this study showed a marked reduction in HbA1c, HOMA-IR, fasting insulin, FBS, scores of VAS for pain, SPADI, NDI, and PHQ-9, and an increase in the ROM (Table 2).
Pre-Test and Post-Test Assessments of the Patient
HbA1c, glycated hemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; VAS, Visual Analog Scale; PHQ-9, Patient Health Questionnaire; SPADI, Shoulder Pain and Disability Index; NDI, Neck Disability Index; ROM, range of motion.
Discussion
The objective of the study was to evaluate the impact of IYN in the management of a patient with DPN and PAS. The results of this study showed a marked reduction in HbA1c, HOMA-IR, fasting insulin, FBS, and scores of VAS for pain, SPADI, NDI, and PHQ-9, and an improvement in ROM. It suggests that IYN was effective in reducing pain, shoulder, and neck disability, depression, and improving glycemic control and ROM of a patient with DPN and PAS.
Previous studies reveal that hydrotherapy techniques involving abdominal packs and hip baths (cold application) effectively lower blood glucose levels by enhancing insulin sensitivity through glucose transporter 4 translocation and stimulating nonshivering thermogenesis via the transient receptor potential melastatin-like 8-ion (TRPM-8) channels. In contrast, steam baths (heat application) promote glucose utilization by upregulating heat shock proteins (HSP-70), which reduces inflammation and improves vascular health. In addition, gastro-hepatic packs (hot and cold application), enhance blood flow to abdominal organs, aiding in blood glucose regulation for patients with T2D. 2 Revulsive compress has been shown to induce collagen tissue extensibility and modulate tissue oncotic pressure, thereby reducing inflammation and stiffness in the shoulder. 3
Acupuncture emerges as a promising adjunctive therapy in DPN management, modulating factors such as nerve growth factor signaling and reducing inflammation. Its ability to influence purinoceptors and G-protein-coupled receptors directly addresses neuropathic symptoms. Studies corroborate the efficacy of acupuncture in enhancing sensory and motor nerve conduction while mitigating neuropathic pain, aligning with the positive outcomes observed in this case. 5 Moreover, local acupuncture points used for the shoulder in this intervention likely improved regional blood flow, enhancing mobility and reducing periarthritis-related pain. 3
Yoga therapy enhanced nerve conduction velocity, reduced pain perception, and provided significant neuroprotective effects, fostering better overall management of DPN. 5 In this case, therapeutic exercises were integral in alleviating shoulder stiffness and improving the ROM. Sukshma Vyayama aids in activating the stretch reflex and toning the musculature around joints, while rope exercises increase shoulder muscular activity, enabling better movement and reduced pain. 3
Plant-based diets (PBDs) have shown remarkable benefits in improving glycemic control and alleviating pain, which results in mitigating tissue hypoxia and enhancing microvasculature perfusion, directly addressing neuropathic pain and neural damage. The anti-inflammatory and antioxidant properties of PBDs further complement the therapeutic outcomes by reducing oxidative stress, a key contributor to DPN. 5
Physiotherapy and electrotherapy effectively relieve symptoms and enhance the quality of life in DPN. Evidence suggests that exercise therapy may help reduce diabetes-related neuropathic pain, including increased sensitivity to heat and mechanical allodynia. In DPN, reduced Schwann cells impair nerve conduction, affecting nerve function. Electrical stimulation can promote Schwann cell regeneration and improve nerve conduction. It enhances dermal blood flow by increasing the release of vascular endothelial growth factor, which supports Schwann cell proliferation, axonal growth, and nerve regeneration. Several studies have found that electrotherapy can decrease the mechanical pain threshold, promote local vasodilation, and aid in wound healing in DPN. 11
Massage therapy has shown potential as a complementary treatment for DPN 12 and PAS. 13 It supports tissue metabolism by aiding the removal of harmful substances, enhancing blood oxygenation around nerves to promote repair, reducing pain, and improving mobility and ROM. 12 Specifically, Thai foot massage, which applies deep thumb pressure, has demonstrated benefits in enhancing balance, foot sensation, and nervous system stimulation in patients with DPN. 13 Massage using peppermint oil may help with diabetic neuropathy by providing pain relief, reducing inflammation, and improving circulation due to its menthol content, which activates TRPM-8 receptors to modulate pain while lowering oxidative stress and pro-inflammatory mediators through Nuclear factor-kappa B and Mitogen-activated protein kinases pathway regulation. 14
Sun exposure (heliotherapy) may help reduce cardiometabolic dysfunction, which is a risk factor for DPN. Mud therapy benefits DPN by reducing inflammation, modulating pain, increasing nitric oxide levels for better blood flow, and enhancing brain-derived neurotrophic factors to support nerve repair. 5 Foot reflexology has been found to effectively reduce peripheral neuropathic pain in diabetic patients by enhancing nerve function, improving circulation, blocking pain signals, and reducing stress, especially when combined with standard medical treatments. 15 Furthermore, these studies indicate that the combined impact of the IYN intervention may be accountable for the study’s findings.
Strength of this study
The strength of this study lies in its holistic approach, combining multiple therapeutic modalities to address both physical and psychological aspects of DPN and PAS. The comprehensive evaluation of the treatment’s effectiveness with a 3-month follow-up demonstrates sustained improvements in pain, mobility, glycemic control, and mental health, highlighting the potential benefits of yoga and naturopathy in managing chronic conditions. Interventions were well tolerated, and adverse effects were not reported by the patient during the study period.
Limitations of the study
Being a case report, the findings were derived from a single patient, which restricts their applicability to a wider population. Hence, randomized controlled studies with larger sample sizes are recommended to validate the study findings.
Conclusions
IYN intervention was found to be effective in reducing pain, shoulder and neck disabilities, and depression, improving glycemic control and ROM of a patient with DPN and PAS. Although the single case study results are encouraging, their applicability, validity, and the reliability of the study results may vary in a wider population, which is limiting the scope of this study. Hence, randomized controlled trials with larger sample sizes are recommended to validate the study findings.
Patient Perspective
The patient reported that the intervention was very helpful in overcoming the symptoms and enhancing her physical and mental health and well-being. The intervention was simple to implement, straightforward, and successful with no negative side effects.
Informed Consent
Written informed consent was obtained from the patient before the study.
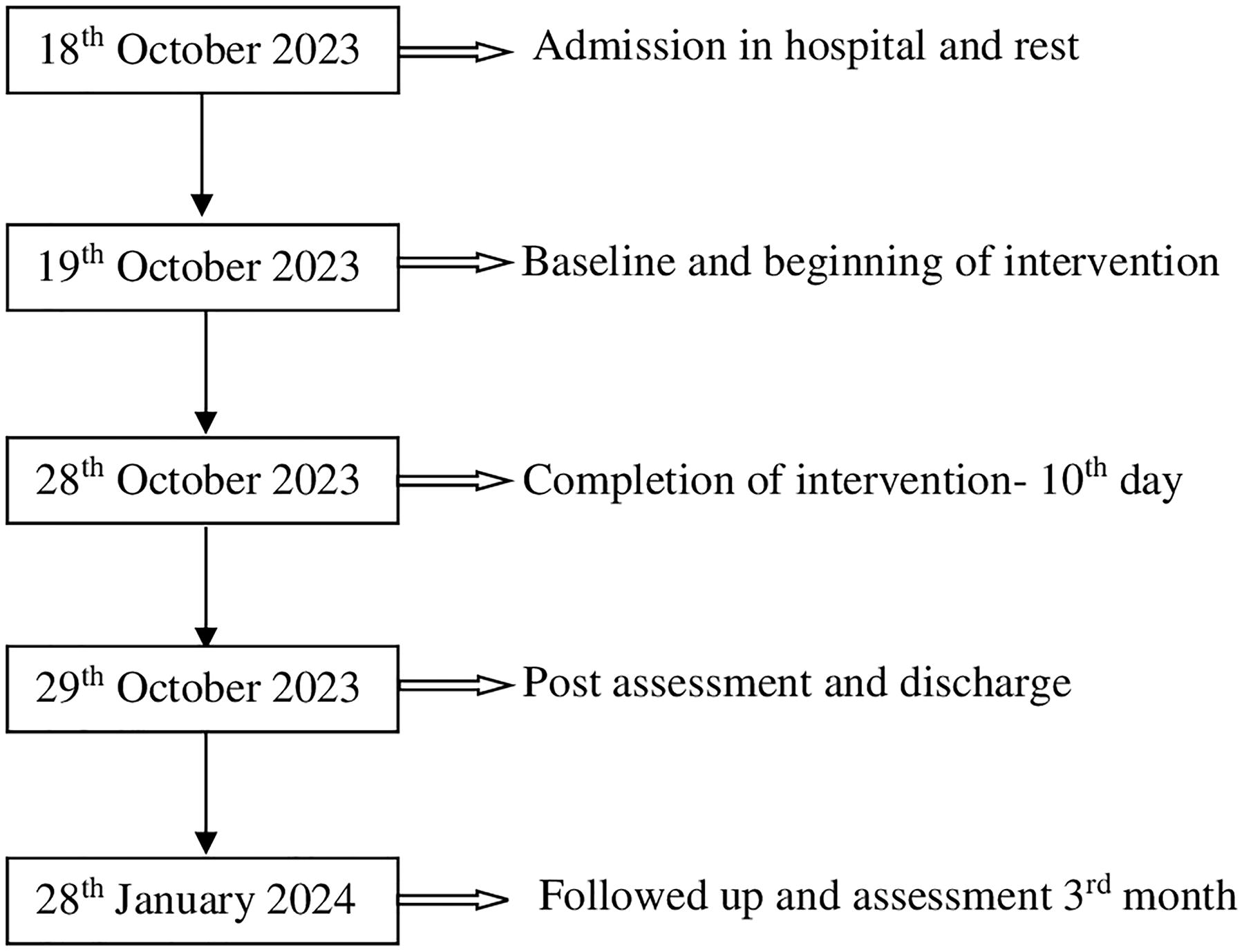
Timeline: A detail of the study from the admission of the patient in the hospital to follow-up has been shown in Figure 1.
Footnotes
Authors’ Contributions
A.V.—Writing original draft, Conceptualization, Investigation; S.S.—Writing original draft; G.S.—Methodology; L.N.— Methodology; A.M.—Writing—review and editing; N.M.—Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.