
Abstract
In this perspective we provide an overview of the recent advances in automated insulin delivery (AID) technologies including adaptive closed-loop algorithms, enabling fully autonomous insulin dosing with meal announcements. This is leading to a paradigm shift in insulin management for both people with diabetes and clinicians, potentially expanding diabetes technology access to a broader population. We discuss the potential for these advances to reduce the cognitive burden of daily diabetes self-management for those on insulin therapy as well as bringing new considerations including psychological adjustments regarding transferring management to an algorithm. We include key themes identified in a recent qualitative study with users of an advanced AID system: dealing with perceived lack of control and developing trust, psychological and behavioral changes in diabetes management and daily routine, and ongoing challenges including the physical burden of pump therapy. Finally, we discuss the implications of technology advances on clinical practice and how clinicians interact with and support people with diabetes using these advanced tools. This includes redefining success that may involve achieving an acceptable level of management for the individual with less effort while improving quality of life. As automation takes on more of the technical burden, clinicians are empowered to engage more deeply in the overall health and life goals of their patients. As automation advances, we are moving toward simplification of diabetes management.
The Evolution of Automated Insulin Delivery Technology
Diabetes is a chronic, demanding condition that poses a constant burden both on people with diabetes and on the clinical teams that care for them. While improving in recent years, only a minority of people with type 1 diabetes (T1D), 26% in the United States, meet glycemic targets, demonstrating that there is an unmet need for better methods to achieve these goals.1,2 Insulin delivery and glucose monitoring technology in T1D care have rapidly advanced with the goal of improving glycemia to be closer to that of people without diabetes. Insulin pump and continuous glucose monitoring (CGM) sensor integration have progressed from low-glucose and predictive low-glucose suspension of insulin delivery when sensor glucose crosses (or is predicted to cross) the low threshold level to algorithm-driven semi-automated insulin delivery based on sensor readings with manual meal and correction boluses. Further advances have included autocorrection boluses, meal detection, as well as the availability of multiple glucose target set points.3–5 One AID system, the iLet bionic pancreas (BP) (Beta Bionics, Concord, Massachusetts), provides fully autonomous insulin dosing automatically titrating all therapeutic insulin including basal, correction, and prandial insulin enabled by three adaptive closed-loop algorithms. The system requires qualitative meal announcements versus precise carbohydrate counting to autonomously determine prandial insulin. To initiate the AID system, only the user’s body weight is needed as input. The system then perpetually learns and automatically refines dosing no longer requiring manually calculating, programming, and adjusting system settings. 6
Randomized controlled trials and real-world clinical studies with various AID systems demonstrate improvement in glycemia (reduction in A1c and hypoglycemia and increase of time-in-range [70–180 mg/dL or 2.9–10.0 mmol/L] to an average of 65%–75% without compromising time-below-range [<70 mg/dL])in people with T1D across all ages and education levels and regardless of diabetes duration, prior insulin delivery method, or baseline A1c levels,7–17 resulting in AID being recommended as the standard of care for people with T1D. 18 Clinical practice guidelines 19 and consensus recommendations on AID use in clinical practice20–22 have been published. The PANTHER program by the Barbara Davis Center for Diabetes, University of Colorado, provides comparative charts of the various systems and clinical management pointers for each (PANTHERprogram.org). 23
Overall, the term “AID” is becoming standard and is used by regulatory agencies such as the U.S. Food and Drug Administration (FDA). The term “AID” is preferred over previous terms such as artificial pancreas or hybrid and advanced hybrid closed-loop technologies.18,21 Currently available semiautomated insulin delivery systems require individualized insulin plans for the initialization of therapy and meal doses based on carbohydrate counting for routine operation. In contrast, the BP is initialized only based on body weight, makes all dose decisions, delivering insulin autonomously, and uses qualitative meal announcements without carbohydrate counting. 6 Fully autonomous insulin dosing with meal announcements represents the next stage in AID development and is changing the paradigm for clinical management of insulin therapy in T1D care.
In addition to currently available commercial AID systems, multiple others are being developed including dual-hormone closed-loop systems adding other hormones such as glucagon and/or amylin, to more closely imitate physiological glucose regulation 24 and as laid out in the bifurcated AID road map. 25 Unregulated open-source systems provide open-access algorithms for customizing an AID system for personal use. 26
Expanding Diabetes Technology Access and Adoption: The Democratization of Health Care
In a 13-week, multicenter, randomized trial, the bionic pancreas pivotal trial (BPPT), a total of 326 people with T1D were randomly assigned to the BP group (219 participants) or the standard care group, defined as any insulin delivery method with unblinded, real-time CGM (107 participants). Participants ranged in age from 6 to 79 years, and the baseline A1c level ranged from 5.5% to 13.1%, with nearly two-thirds having an A1c > 7.5%. A total of 74% of the participants identified as being non-Hispanic White, 10% as non-Hispanic Black, 10% as Hispanic, and 6% as another or more than one race or ethnic group. A total of 34% of the participants reported having less than a Bachelor’s degree, 35% reported having a Bachelor’s degree, and 29% reported having education beyond a Bachelor’s degree (remaining unreported). A total of 34% of the participants were using multiple daily insulin therapy at baseline; 31% were using pump therapy without automation; and 35% were using an insulin pump with partial automation (23%, Control IQ; 8% 670G; 4% predictive low-glucose suspend devices). There were no exclusions for hypoglycemic unawareness, recent episodes of severe hypoglycemia, recent hospitalizations for dysglycemia, or for baseline A1c. 6
The A1c level decreased from 7.9% to 7.3% in the BP group and did not change (was at 7.7% at both time points) in the standard care group (mean adjusted difference at 13 weeks, −0.5 percentage points; 95% confidence interval [CI], −0.6 to −0.3; P < 0.001). The percentage of time that the glucose level as assessed by CGM was below 54 mg/dL did not differ significantly between the two groups (13-week adjusted difference, 0.0 percentage points; 95% CI, −0.1 to 0.04; P < 0.001 for noninferiority). The rate of severe hypoglycemia was 17.7 events per 100 participant-years in the BP group and 10.8 events per 100 participant-years in the standard care group (P = 0.39). No episodes of diabetes-related ketoacidosis occurred in either group. 6
The BPPT pediatric cohort was 65.5% non-Hispanic White, 14.5% Hispanic, 9.7% non-Hispanic Black, and 2.4% Asian and therefore reflective of the population of children with T1D as reported in the SEARCH study. 27 The overall cohort, while not perfectly representative, was more reflective than previous pivotal studies of semiautomated systems of the general U.S. population with T1D in terms of race/ethnicity, socioeconomic status (SES), range of A1c, and the distribution of baseline therapies (multiple daily insulin injection therapy, insulin pump, and semi-automated insulin pump); thus, the results observed may be more generalizable. 6
A sub-analysis of the BPPT showed that use of the BP resulted in improvements in glycemia by a similar degree among both White and minority participants when adjusted for baseline A1c. 28 In the standard care group, baseline difference in A1c between White and minority participants remained unchanged at follow-up, while in the BP group, the difference in A1c among White and minority participants was reduced at follow-up. While the treatment effect did not differ by race when adjusting for baseline glucose, the differences in A1c between White and minority participants were reduced after using the BP system, likely because those with higher baseline A1c had greater improvements with the BP system than those with lower baseline A1c. Those with lower SES had higher baseline A1c, reflected in greater improvements with the BP system.
Similar improvements in glycemia with the BP relative to standard care in minority and White participants may be due to the autonomous dosing by the BP, which determines every insulin dose independently of the skill of the health care provider or the user’s level of diabetes numeracy or technical ability. It is possible that a broad base of prescribing health care providers and individuals with diabetes could use the device safely and effectively.29,30 The BP improved glycemic outcomes in a racially and ethnically diverse minority cohort, with similar improvements seen in both minority and White subpopulations, suggesting generalizability to a real-world population of people with T1D. 28
A real-world analysis studied the impact of the BP on glycemia during the first year after FDA clearance and compared with the results of the BPPT. Commercial BP users who had a baseline A1c value available and had at least 3 weeks of BP data in the cloud were included. Baseline A1c values were compared with the glucose management indicator (GMI) values calculated from all available CGM data, both reported as mean ± standard deviation. Adults (≥18 years) and children were analyzed separately. Data from the BPPT were analyzed in the same way for comparison. The percentage of time with CGM glucose <54 mg/dL during BP use was calculated for all groups and reported as median (interquartile range). Data from 2759 adults and 541 children were included in the real-world analysis and from 218 adults and 112 children in the BPPT analysis. Adult commercial users had a baseline A1c of 8.4 ± 1.9% and a BP GMI of 7.2 ± 0.4% (difference: –1.2%), compared with 7.7 ± 1.2% and 7.0 ± 0.3%, respectively, in the BPPT (difference: –0.7%). Pediatric commercial users had a baseline A1c of 9.1 ± 2.1% and a BP GMI of 7.7 ± 0.5% (difference: –1.4%), compared with 8.1 ± 1.2% and 7.4 ± 0.3%, respectively, in the BPPT (difference: −0.7%). The 3300 commercial users of all ages had a baseline A1c of 8.5 ± 1.9% and an iLet GMI of 7.3 ± 0.5% (difference: –1.2%). The time with CGM glucose <54 mg/dL was 0.3 (0.1–0.6)% in adults and 0.3 (0.1–0.6)% in children in commercial use and 0.3 (0.1–0.5)% in adults and 0.3 (0.2–0.6)% in children in the BPPT. The baseline A1c values of commercial users were higher, and the decreases from baseline A1c to BP GMI values were larger than among participants in the BPPT. The time spent <54 mg/dL was comparable in both settings. 31
This research in fully autonomous insulin dosing highlights the transformative potential in broadening access to technology. Traditionally, ideal candidates for insulin pump therapy have been individuals highly engaged in their diabetes management, able to manage complex tasks such as carbohydrate counting, bolus adjustments, and manual corrections based on an insulin sensitivity factor. 32 Advancements in fully autonomous, adaptive systems are redefining these criteria. Fully autonomous, adaptive systems such as the BP may be suitable for individuals who previously struggled with manual management due to the complexity involved. The BP’s ability to maintain target glycemia with less user input could make it an option for those experiencing diabetes burnout or those who have difficulty following intensive self-management plans. The BP exemplifies a shift toward simplifying diabetes management, reducing the need for high-level expertise, and potentially changing the traditional criteria for insulin pump therapy candidacy.
The author (P.M.) has refined a three-step decision-making process for clinicians to use to help people with diabetes on insulin therapy make informed choices regarding their preferred method of insulin delivery, as shown in Figure 1.
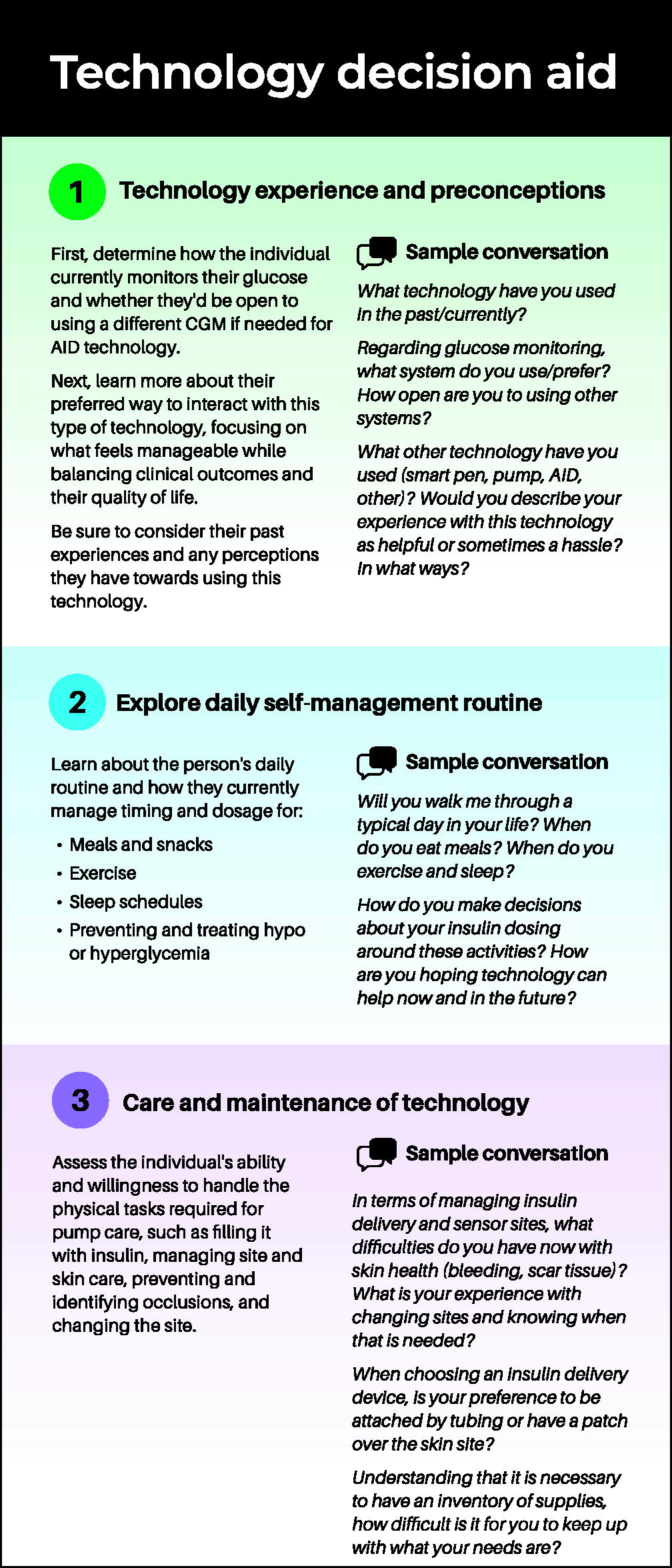
Technology decision aid and sample conversation. A 200-character description of the article for social media: Fully autonomous insulin dosing with meal announcements is the next stage in AID development, shifting the paradigm for T1D management toward simplification and expanding technology access to a broader population. AID, automated insulin delivery; T1D, type 1 diabetes.
Reducing the Cognitive Burden of Diabetes: Diabetes Numeracy and Carbohydrate Awareness
While automated insulin dose calculators as part of smart insulin delivery systems have eased the burden of calculating meal doses, counting carbohydrates can still be problematic for those with limited numeracy skills. It is estimated that approximately 69 million Americans have limited health numeracy skills. 33 The ability to apply numeracy skills to perform diabetes self-management tasks is crucial in the management of diabetes, particularly for those on complex, intensive insulin therapy. 34
Traditional candidates for insulin pump therapy were those who could perform advanced or precise carbohydrate counting as in the Diabetes Control and Complications Trial.35,36 Though critical to optimize insulin pump therapy, many with diabetes are challenged to accurately quantify the carbohydrate content of foods. A small, randomized controlled trial of 31 adolescent subjects using AID compared precise carbohydrate or relative meal-size bolus dosing and found that both approaches resulted in achieving similar glycemic outcomes, suggesting that AID systems can provide acceptable levels of glycemia for nonexpert carbohydrate counters. 37 Some level of carbohydrate awareness is still important for AID users, to maximize time-in-range. A continuum of carbohydrate awareness is a framework developed by Sulik et al., starting with the ability of individuals to identify foods containing carbohydrate to, at the next level, simplified carbohydrate counting, which is being able to quantify carbohydrate foods in order to assign meal size, to the advanced stage, which is being able to determine grams of carbohydrate in a food/serving (advanced or precise carbohydrate counting). It is recognized that as the complexity of carbohydrate awareness increases, the potential burden increases. 38 While precise carbohydrate counting is an important skill to master for traditional pump therapy, advanced algorithms in current AID systems incorporate sensor glucose, glucose trend, rate of glucose change, and active insulin to adjust insulin delivery on a continuous basis. These systems accommodate less accurate carbohydrate entry or qualitative meal announcements and can partially compensate for missed or late boluses.6,37,39
New Considerations and Paradigm Shifts
Perceived lack of control and establishing trust
While AID has resulted in improvements in diabetes-specific quality of life, increased flexibility, and improvements in relationships, the advances in technology also bring some additional considerations. In fully autonomous, adaptive systems such as the BP, this includes learning to trust the system and relinquish control to the algorithm. This can be particularly challenging for those who have spent years of their life with diabetes being ever-vigilant in responding to the many variables impacting glycemia, 40 and, in fact, with semiautomated AID systems, a certain level of vigilance is still required due to limitations of the system. Upon initiation of AID, there may be a probation period as users assess the system’s effectiveness in managing glycemia safely and gain a level of understanding about how the algorithm works. Particularly with fully autonomous, adaptive systems, such as the BP, the algorithm’s learning process requires the user to refrain from intervening and let the system work at its own pace in addressing falling or rising glucose levels. Limited options to report day-to-day contextual variations such as physical activity and certain types of meals contribute to uncertainty in trusting the algorithm.41,42 Those with higher baseline A1c tend to report greater satisfaction and trust in automated systems, while those with lower baseline glycemia are more likely to engage in compensatory behaviors and experience greater cognitive and emotional stress in the event of suboptimal automation performance.41,42
Fostering an atmosphere of trust and collaboration between the individual living with diabetes and their care team invites an ongoing dialogue regarding efforts to maximize benefits and reduce the burden of AID therapy, recognizing the trade-offs are unique to each individual. 40 It may be time to redefine success in insulin management, recognizing the need for a balance between achieving an optimal level of glycemia with the effort required to achieve it. The individual perceptions of device benefits and burdens are key in continued device use. 43 While higher use of the algorithm has been associated with more optimal glycemia,44–46 an average discontinuation rate of 50%, particularly among youth, has been reported with semiautonomous AID.45,47 Reasons for discontinuation include cost, supply challenges, physical burden related to wearing devices, higher workload than expected, disappointment if glycemic benefits are not met, disruptions in daily routines, and other life stressors.48–51 With fully autonomous, adaptive insulin dosing, those with the highest A1cs at baseline benefit from the largest reductions in A1c without increased engagement. 52
Psychological and Behavioral Changes in Diabetes Management and Daily Routine
Research on AID systems have included person-reported outcome measures to evaluate quality-of-life changes in addition to clinical benefits, and while results have been mixed, overall improvements have been found in diabetes-specific distress (in adults and caregivers but not consistently in children and adolescents), 53 subjective and objective sleep, the emotional and behavioral burden of glucose management, self-management burden and worries, and increased flexibility and spontaneity, as well as relationships. 41 A randomized controlled trial conducted in a high-risk cohort of youth with suboptimal glycemia (A1c > 8.5%) on pump therapy with or without CGM evaluated the efficacy of semi-automated AID. The study found that while glycemia improved, there was no evidence for difference in psychosocial outcomes between the two groups at study end, suggesting the need for ongoing psychosocial support for this cohort. 54 Instruments are available to measure specific perceptions and experiences related to AID therapy including the INSPIRE questionnaires 55 and adaptations of the Technology Acceptance Scale.56,57 Diabetes-related distress scales are available for assessing diabetes distress in T1D and T2D. 58
Given the uniqueness of the fully autonomous, adaptive BP, it is vital to assess the psychosocial impact and user experience when using the system. The BPPT, previously discussed, also evaluated the psychosocial impact and user experience of the BP. 59 Subjects completed psychosocial questionnaires at baseline, mid-study, and the end of the trial. In all age-groups, most participants would recommend using the BP, including those with previous experience using AID devices. Similarly, the vast majority of participants reported a high level of perceived benefits and a low number of perceived burdens. Adult participants reported significant decreases in the fear of hypoglycemia and in diabetes-specific emotional distress, as well as improvements in their perceived well-being. Findings demonstrate acceptability, reduced burden, and positive psychosocial outcomes for adults. Children and teenagers also report high acceptability and reduced burden but less clear improvements in psychosocial outcomes.
These studies highlight that while AID systems offer significant benefits, challenges related to device wearability, user satisfaction, and glycemic control can influence discontinuation rates. Advances in automation have the potential to significantly reduce patient attrition from AID devices by addressing key barriers to sustained use. More sophisticated algorithms that minimize the need for user input—such as fully autonomous dosing with meal announcements that does not require precise carbohydrate counting or frequent manual adjustments—can reduce the cognitive and emotional burden associated with diabetes management. This simplification may improve user satisfaction and decrease frustration, particularly among those with limited numeracy or diabetes-related burnout. Furthermore, automation that adapts to individual routines and physiological patterns can enhance trust in the system’s ability to manage glucose levels reliably, which is critical for long-term use. Reducing technical complexity also makes the technology more accessible across a wider range of clinical settings and user populations, including those previously considered less ideal candidates. By improving glycemic outcomes with less user effort and fewer disruptions to daily life, these advancements may foster greater confidence, convenience, and quality of life—factors that could support reduced discontinuation rates.
Addressing deskilling and establishing backup plans
AID systems can help users achieve improved glycemia with less effort compensating for carbohydrate counting inaccuracies, disruptions in daily routines, unplanned physical activity, or missed boluses, and so forth.59–61 This raises the potential for deskilling, that is, forgetting how to carry out key diabetes self-management tasks such as giving injections, checking blood glucose, carbohydrate counting, and so forth. Concern around deskilling should not deter a clinician from providing the benefits of technology to individuals, but rather the clinician should provide and educate on an easy-to-interpret plan for manual diabetes therapy (i.e., nonautomated subcutaneous insulin delivery by pump or injections) for the infrequent occurrence of technology absence/failure. 18 Individuals using advanced technologies should have an adequate technical understanding of the technologies to be able to troubleshoot. The user and their clinical team should have remote access to their AID system data to determine manual basal, mealtime, and correction doses. Cloud-based data including the basal doses and usual meal doses are available on demand for both BP users and their clinical team. These data are visible within the device by reviewing metrics displayed by selecting the Bionic Circle/CGM value and in the device’s history.
Reducing the Clinical Burden for the Clinician
AID systems are increasingly used in T1D, typically provided in the endocrinology clinic due to the intensive setup and programming required and the need for expertly trained staff and resources for ongoing support. 62 Since it is estimated that approximately half of U.S. adults with T1D see their primary care provider (PCP) for diabetes management, it is vital to be able to offer technology such as AID in primary care. 63 With 75% of U.S. counties not having endocrinologists available, endocrinology clinics are less accessible than primary care offices, especially in rural areas. 63 Historically, managing insulin delivery devices has required more time and expertise than a PCP might be able to provide due to the need to address a variety of health concerns in a short visit time frame. In a 2023 survey, 46% of PCPs who did not prescribe insulin pumps (n = 112) identified the time required to manage patients on insulin pump as a barrier to prescribing pump therapy. 64
The BP was deployed in a randomized clinical trial including 40 participants with T1D comparing deployment in primary care versus endocrinology and in-person versus telehealth. Of the participants, 97% achieved an average glucose <183 mg/dL, representing an A1c level <8%, while 64% achieved an average glucose <154 mg/dL (representing an A1c level <7%). An overall average glucose reduction of 17 mg/dL and a time-in-range increase of 11% with no change in sensor-measured hypoglycemia using BP compared with usual care were achieved showing that the BP can be effectively initiated by PCPs and via telehealth, raising the potential to meaningfully expand technology access. 29
A qualitative sub-study sought to identify and understand the experiences of primary care patients with T1D using the fully autonomous, adaptive BP during the clinical trial. 30 Participants completed a brief semi-structured interview after the trials’ completion regarding their perceptions of and experiences with using the BP. In addition to clinical improvement, results showed the beneficial impact of the system on psychological and behavioral aspects of diabetes management. Since ongoing adjustment of insulin therapy settings is not required, the diabetes care and education specialist can play an expanded role in the ongoing management of the system in partnership with the user as prescriptive authority is not required for providing the education regarding dosing behaviors that influence the functioning of the adaptive-closed-loop algorithms.
Shifting from adjusting therapy settings to behavior coaching
Behaviors that contribute to optimal glycemia in semi-automated AID can be challenging in the context of fully autonomous, adaptive insulin dosing, requiring significant adjustments in learning to rely on a technology device rather than oneself to effectively and safely manage diabetes. There can be a sense of lack of control due to the limited opportunity for user input and interaction in treatment decisions.30,48,59 While the user is building trust in the proper functioning of the AID system, users may try to trick the system into delivering extra or less insulin by announcing “more” or “less” than usual meals or entering carbohydrates that are not consumed. 48 Discussing management goals and consequences of these behaviors can help in optimizing device use. The role of the clinical team shifts from making settings adjustments to behavioral counseling, a return to the art of medicine that may be uncomfortable for clinicians initially as they adjust to this evolution.
Instructing new users in BP use include advising users during the first few days of use to eat meals that have the “usual” amount of carbohydrates for them for each meal type and to announce them as “usual.” Consistency in choosing the meal type and size facilitates the system’s learning. Users should announce right at the start of the meal and can announce up to 15 min before or up to 30 min after, but not earlier or later than that. When getting started and while the algorithm is still learning, users should be advised to wait at least 4 h before eating meals with carbohydrate and announcing again to give the system time to learn if the dose should adapt up or down. Supplementary Table S1 is available online that lists potential compensatory behaviors that may be observed in BP users and the recommended clinical intervention and patient education recommended in each case.
Future Opportunities
Addressing the remaining physical burden of diabetes technology
While the cognitive or mental burden of daily insulin management with T1D may decrease with AID, the continued physical burden of wearing technology likely contributes to technology non-adoption or discontinuation. 65 Physical burden concerns include maintaining infusion site health, pain and discomfort at the site, needing to make site changes early, aesthetic concerns of wearing a visible device, dealing with the inconvenience of tubing and having a device attached when engaged in certain activities, as well as the hassles of ordering and maintaining needed supplies, and the care and maintenance of the device. 65 Current AID systems requiring wearing and maintaining two or more devices on the body may amplify these issues. Simple patch pumps not requiring tubing and implantable CGM devices or other CGM innovations will help in addressing some of the physical burden concerns.
Dual-hormone insulin pump systems, faster insulins, enhanced delivery
Dual-hormone pump systems delivering other hormones in addition to insulin (glucagon or amylin) may better reproduce the physiology of the endocrine pancreas and have been suggested as an alternative tool to overcome insulin-only limitations. 24 In addition, novel ultra-rapid-acting insulin analogs with a more physiological time-action profile are being investigated for use in AID devices, to further improve postprandial glycemia.24,66 Mechanical problems with insulin delivery, the delay and variability of insulin absorption from the subcutaneous space, and variability of insulin action represent key challenges to AID systems, particularly in the context of glycemic variability introduced by meals, exercise, and illnesses. 24 Incorporation of insulin sensing to provide a true measure of insulin-on-board could enhance AID capability. 67
Sensor and physiological data integration
The accuracy of continuous interstitial fluid glucose sensing is another critical determinant of the efficacy of current and emerging closed-loop systems. An important determinant of glucose sensor accuracy is the physiological time lag of glucose transport from the vascular to the interstitial space. In most circumstances, a 5-min time lag of glucose from the intravascular to the interstitial compartment is offset with a comparable or greater lag in the pharmacokinetics of insulin analogs. Interference with certain substances and medications, the need for fingerstick test calibration, compression artifacts, as well as pairing and connectivity issues causing transient disconnection and interruption of communication between the sensor transmitter and the receiver must be overcome.24,42
Developers are investigating the integration of additional sensors such as continuous ketone monitors and other advanced technologies, enabling automated detection of physiological variables affecting glucose, such as meal timing and composition, exercise, stress, illnesses, sleep, and circadian variations in insulin sensitivity. 42 Research is exploring the use of the heart rate as an additive input to AID systems through a heart rate monitor triggering an exercise algorithm to minimize time-below-range during exercise. 68
Alerts from an artificial intelligence (AI)-controlled smartwatch app detecting eating behavior show improved glycemia in individuals with T1D with a history of missed or late boluses. 69 Communication between such applications and an AID system could improve the accuracy of automated boluses. 42 Multivariable AID systems are in development that can handle unannounced physical activity and meals without any manual announcements by the user. These systems show promise in improving glycemia by modulating insulin dosing in response to the occurrence and intensity of spontaneous physical activities. 70 Another advancement being investigated is the estimation of gut absorption to avoid the need for manual carbohydrate counting and meal announcements. 71 Robust control algorithms and adaptive systems able to collect and integrate information from wearable devices other than glucose sensors will need to be developed.24,42
AID use in pregnancy
The use of AID in the context of pregnancy complicated by T1D is also being explored. Diabetes during pregnancy is associated with significant maternal and fetal health risks. Insulin requirements change during pregnancy, necessitating careful and effective management. Although commonly used in clinical practice, FDA-approved algorithms for AID systems do not have pregnancy-specific glycemic targets. A review of the literature found that AID systems can achieve near-desired glycemic targets with minimal hypoglycemia in pregnant women with T1D. 72 Randomized controlled trials are needed to confirm these findings and to achieve FDA indications in pregnancy.
AI integration
AI is increasingly being integrated into health care data applications. The use of AI to replicate AID algorithm performance in a pilot study showed that machine learning was able to produce equivalent outcomes with a six-fold lower computational demand. 73 Results indicate that the use of AI in algorithmic insulin delivery can enhance the battery life of the typically limited-power devices in which the control algorithms are commonly situated. Simultaneously, reduced processing power may increase the number of devices that can function as AID system interfaces. Research using explainable AI capabilities shows promise in the detection of acute psychological stress, which can then inform multivariable AID systems to intervene to counteract the stress-induced glycemic excursions in people with type 1 diabetes. 74
Cybersecurity, data protection, and privacy
Sherr et al. discuss these concerns extensively in the joint AID Consensus Report, emphasizing the importance of continuous testing of AID system for cybersecurity and continued efforts to ensure data generated through the use of AID systems is used in a fair and transparent manner. 21
Conclusions
AID systems offer the potential of significant glycemic and quality-of-life benefits to people with T1D as well as potential improvements in device attrition/abandonment with psychosocial and health benefits with fully autonomous, adaptive dosing. Initial concerns when first learning to rely on a technology device rather than oneself to effectively and safely manage diabetes are to be expected. Open discussions between the potential technology user and their clinical care team are vital to set expectations regarding optimal use of the technology and to clearly communicate that the more advanced, fully autonomous, adaptive systems provide limited opportunity for user input and interaction in treatment decisions. The BP’s ability to maintain target glycemia with less user input could make it an option for those who experience diabetes burnout or those who have difficulty following intensive self-management plans. The BP exemplifies a shift toward simplifying diabetes management. As devices are worn on the body, they still involve a degree of physical burden involved in the care and maintenance of the device.
It is vital to seek to understand the person–technology interaction trade-off decisions that each individual living with T1D must make when choosing technology to support their diabetes management. Readers are encouraged to use the Technology Decision Aid and Sample Conversation (Fig. 1) to facilitate informed decision-making conversations around technology. It will be important to continue to study the quality-of-life impact of AID systems as they advance, potentially bringing important insights for addressing cognitive, emotional, or behavioral barriers toward optimal use. Critical are efforts to maximize benefits and minimize burdens of AID therapy and with sensitivity to the personal trade-off between both. The future is bright with promising developments underway to significantly improve clinical outcomes and quality of life while reducing the burden of care for a much broader population. Attention must also be paid to the paradigm shifts the clinical team is experiencing as automation advances including the potential of expanding technology integration into primary care.
Footnotes
Authors’ Contributions
P.M.: Conceptualization (supporting); writing—original draft (supporting); and writing—review and editing (equal). K.P.C.: Conceptualization (supporting) and writing—review and editing (equal). J.M.: Conceptualization (lead); writing—original draft (lead); and writing—review and editing (equal).
Author Disclosure Statement
Kelly Postiglione Cook is an employee of Beta Bionics. Janice MacLeod is a consultant for Beta Bionics.
Funding Information
No funding was received for this article.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.