
Abstract
Background:
Diabetes is a significant global health challenge, with a rapidly increasing prevalence worldwide. Managing type 2 diabetes (T2D) effectively requires addressing clinical, behavioral, and social factors. Despite major advances in healthcare in the UAE, the majority of individuals diagnosed with type 2 diabetes (T2D), even those with access to care and the latest pharmacotherapy remain classified as “poorly controlled,” highlighting the urgent need for new models of care. The GluCare hybrid care model integrates in-clinic care and remote continuous data monitoring (RCDM) to optimize long-term diabetes management, incorporating advanced digital tools as an adjunct focused on behavioral change. The GluCare hybrid model’s effectiveness is evaluated using the International Consortium for Health Outcomes (ICHOM) diabetes standard set. This study examines 12-month outcomes of T2D patients under the GluCare model, focusing on clinical and medication trends.
Methods:
This retrospective, real-world observational study included 208 patients with T2D randomly selected managed under the GluCare hybrid model for at least 12 months. Complete datasets were required. Data were collected from medical records, adhering to the ICHOM diabetes standard set.
Results:
The study revealed significant improvements across all clinical parameters. Mean HbA1c decreased from 7.7% to 6.55% (P < 0.001), with 72.6% of patients achieving levels below 7%. Patients with baseline HbA1c > 7.5% demonstrated the greatest reductions (9.18%–6.93%). Lipid profiles improved, with reductions in total cholesterol (−20 mg/dL), LDL (−19.2 mg/dL), and increases in HDL (+3 mg/dL). Systolic and diastolic blood pressure decreased significantly by 6.1 mmHg and 4.2 mmHg, respectively (P < 0.001). BMI and waist circumference showed notable reductions (−1.9 kg/m2 and −5 cm, respectively). Insulin use decreased by 50%, and patients achieved better glycemic control (HbA1c < 7.5%), aligning with the model’s focus on reducing medication dependency through enhanced behavioral change and engagement with RCDM techniques.
Conclusion:
Despite widespread access to GLPs, most diabetes patients in the UAE remain poorly controlled. The GluCare hybrid model significantly improved glycemic control, cardiovascular health, and weight management over 12 months, surpassing traditional care. Estimated cost analysis showed a $23,485 reduction in health care costs within the first year. Maintaining glycemic control could prevent costs from rising up to 9.4 times over a decade. Future research should assess cost-effectiveness, long-term complications, and scalability.
Introduction
Diabetes represents a major global public health challenge, with an estimated rising prevalence of 10.2% (578 million) by 2030, worldwide. 1 The International Diabetes Federation (IDF) has reported that 12.3% of the adult population in the UAE are diagnosed with diabetes, which accounts for 990,900 cases 2 with type 2 diabetes (T2D), accounting for 90% of the population 1 and over 75% of patients with T2D are classified as poorly controlled, with the largest diabetes provider in the UAE reporting an average HbA1c of 7.4% despite no barriers to care access or medications. 3 However, it is important to note that T2D is affected by many other behavioral and social factors including perception of illness, individual’s coping mechanisms, readiness to change behavior, presence of family support, and financial capabilities. 4 Traditional care providers have passed the onus of behavioral change exclusively back to patients and have largely taken a prescription-only approach when it comes to the management of chronic disease. Recent studies have emphasized the role that digital tools, such as mobile applications, play in diabetes management by tracking dietary habits, sleep, and overall adherence to the treatment regimen provided by health care professionals.5,6
Despite the wide range of monitoring and tracking features that digital tools offer, the management of diabetes is not helpful unless their health care professionals are completely bought into the concept and actually using such technology in daily practice. 7 Fang et. al reported that regular communication between health care providers and patients via text messages and phone calls have brought about a significant decrease in HbA1c levels. 8 In addition, the importance of health care providers’ role in building trust and fostering self-management in patients has been well-documented, emphasizing the need for “active partnerships” and “personalized education”. 9 Digital health stand-alone solutions that were designed to help improve diabetes outcomes have largely failed. 10 These gaps could be bridged through the incorporation of hybrid models in diabetes care to ensure both monitoring and feedback systems between patients and health care providers are fulfilled. 11
The GluCare hybrid care model exemplifies this approach by creating an end-to-end vertical integration solution using remote continuous data monitoring (RCDM) with in-clinic consultations, leveraging advanced digital tools such as continuous glucose monitoring (CGM) and wearable devices such as ŌURA rings. The model, detailed in a recent in-depth NEJM Catalyst article, highlights its unique data-driven, patient-centric approach, emphasizing real-time tracking, feedback, and multidisciplinary care. 11 While an in-clinic setting is crucial for building trust between health care providers and patients, it also tackles the necessary parts of the treatment in diabetes education and behavioral therapies, which might be challenging to overcome in a digital-only offering. 12 The hybrid model utilizes the strengths of both digital and physical care elements to facilitate real-time monitoring, personalized and timely interventions, and continuous patient engagement with their health care providers as part of the standard care model; therefore, leading to a more comprehensive and integrated approach to optimize long-term patient outcomes.13,14
In a previous study, the incorporation of the GluCare Hybrid Model has shown significant results in reducing weight (−4.0 ± 5.3, P < 0.001), waist circumference (−4.74 ± 7.8, P < 0.001), HbA1c levels (−1.00 ± 1.3, P < 0.001), and systolic (−3.1 ± 13.1, P = 0.035) and diastolic blood pressure (−3.4 ± 9.9, P = 0.002). 14 In this study, the International Consortium for Health Outcome Measurement (ICHOM) diabetes standard set was used, where it takes into account the clinical measurements (HbA1c, lipid profile, TSH, etc.). 15 The use of this standard set plays a pivotal role in advancing patient care by providing a framework for measuring and comparing health outcomes. 15 In this study, we aim to further investigate the long-term outcomes of T2D patients managed under the GluCare hybrid care model using the gold-standard ICHOM standard set by examining clinical parameters such as glycemic control, cardiovascular health, anthropometric measures, and medication change over time.
Methodology
Intervention: The GluCare hybrid model
The GluCare hybrid model integrates traditional in-clinic, patient-centric care with a data-driven, RCDM approach to optimize the management of T2D. The model emphasizes personalized, holistic care through the seamless combination of real-time monitoring and direct interaction with a multidisciplinary care team. Its efficacy and innovation have been highlighted in the context of advanced diabetes and obesity care delivery frameworks.11,13,14
In-clinic component
The in-clinic care aspect adheres to the standards of the American Diabetes Association, focusing on evidence-based, patient-centered strategies. Patients receive individualized consultations from a multidisciplinary team, including physicians, dietitians, diabetes nurse educators, exercise practitioners and life coaches. In addition to glycemic management, in-clinic visits focus on optimizing pharmacotherapy and comprehensive diagnosis. Regular assessments of comorbidities and behavioral factors are integrated into the care process. Personalized goals for diet, stress, physical activity, sleep and adherence are established, which are reinforced through the RCDM component and wearable technology.
Out-of-clinic component—RCDM
The RCDM component compliments the in-clinic by integrating advanced mobile apps, wearable devices, and connected health technologies for real-time monitoring by the same team members mentioned in 2.1.1. Key features of RCDM include: (i) CGM: patients track glucose levels in real time, providing actionable insights for both patients and health care team. (ii) ŌURA ring: track additional metrics such as sleep data, stress, heart rate variability, physical activity, and body temperature. These metrics are integrated into the care model to monitor overall health and detect early signs of physiological stress, which may impact diabetes management. (iii) Food logs: patients log their meals and activity levels using the app’s advanced AI scanning technology, which calculates calorie and macronutrient content. This approach improves compliance with food logging compared with traditional methods. With detailed carbohydrate breakdowns, dietitians provide personalized feedback, helping patients understand how their dietary choices impact their glucose levels and overall health. The integration of continuous wearable data and patient-reported metrics enables a view of the patient’s health. Physicians, dietitians, and health coaches review these data bi-weekly, providing real-time feedback and adjusting care plans as needed. 11 As part of the provider’s commitment to shift away from a fee for service care model to an outcome based one, it is important to note that nonreimbursable services such as wearables, exercise practitioners, life coaches, and continuous monitoring are all offered as standard to patients with no additional cost to patients or payors.
Study design and participants
This retrospective, real-world observational study analyzed the long-term outcomes of patients with T2D managed under the GluCare hybrid model of care, using the ICHOM standards set. The study included patients attending GluCare Integrated Diabetes Center, based in Dubai, UAE. Written informed consent was obtained from all patients during their initial visit and all patients were given the chance to opt out of the RCDM components. Inclusion criteria were as follows:
Patients diagnosed with T2D. Patients introduced and managed under the GluCare model of care for a minimum of 12 months. Patients with recorded baseline HbA1c. Patients with at least two in-clinic visits (baseline and follow-up) and documented ICHOM-compliant health metrics.
The final analysis included 208 randomly selected patients who attended both baseline and 12-month follow-up measurements.
Data collection
The data were extracted from the physicians’ patient records using the electronic medical record (Diamond, Hicom, UK) and categorized based on the ICHOM set scales of measures. 15 Variables collected included: patients’ gender, age, weight, height, waist circumference, diabetes duration, current diabetes-related drug intake including GIP/GLP-1 receptor agonists, GLP-1 receptor agonists, oral hypoglycemic agents (e.g., metformin, SGLT2 inhibitors, sulfonylureas, and DPP-4 inhibitors), and insulin (short and long-acting) for diabetes management regimen. The cost of these medications was calculated, and the costs were converted from UAE Dirhams to U.S. Dollars using the official conversion rate of 1 USD = 3.67 AED. Hypertension treatments were also recorded, such as ACE inhibitors, beta blockers, angiotensin II receptor antagonists, and calcium channel blockers. In addition, statin therapy for lipid management was included. Laboratory variables were also extracted including lipid profile (total cholesterol, LDL, HDL, and triglycerides), liver enzymes (AST and ALT), kidney profile (eGFR, uric acid, and urinary microalbumin), and HbA1c.
Ethical approval
Ethical approval was obtained from the Dubai Health Authority, and patient data were anonymized to maintain confidentiality.
Statistical analysis
Baseline characteristics of the study cohort were summarized using appropriate descriptive statistics. Categorical variables were expressed as frequencies and proportions, while continuous variables were presented as means with standard deviations (SD). Differences in baseline characteristics between participants with baseline HbA1c levels ≤7.5% and >7.5% were assessed using chi-square tests and Fisher’s exact tests for categorical variables and independent t-tests for continuous variables.
The clinical laboratory parameters of the cohort, including HbA1c, were analyzed across the entire cohort and stratified by baseline HbA1c levels (≤7.5% and >7.5%). Changes in these parameters between baseline and the 12-month follow-up were assessed using paired t-tests for normally distributed variables and Wilcoxon signed-rank tests for non-normally distributed variables. The unadjusted mean HbA1c values and their corresponding 95% confidence intervals (CI) at each time point (baseline and 12 months) were estimated. All analyses were performed using R version 4.4.0. A P value < 0.05 was considered statistically significant.
Results
Basic demographics and characteristics
At baseline, the study cohort (n = 208) had a mean age of 48.26 ± 10.39 years, with no significant difference between HbA1c subgroups (P = 0.353), and consisted predominantly of males (79.8%, P = 0.939). The mean BMI was 30.1 ± 5.51, and waist circumference averaged 102.75 ± 13 cm, both showing no significant differences between HbA1c ≤7.5% and >7.5% groups. Notably, the use of GIP/GLP-1 receptor agonists (44.1% vs. 26.1%, P = 0.006) and insulin (16.1% vs. 4.3%, P = 0.001) was significantly higher in the HbA1c >7.5% group, indicating a greater therapeutic burden at baseline in patients with poorer glycemic control (Table 1).
Baseline Characteristics Overall and Based on Starting HbA1c at Baseline (n = 208)
The P values <0.05 indicate the statistical significance.
Twelve-month clinical outcomes of the GluCare hybrid care model
After 12 months of the GluCare hybrid care model, significant improvements were observed across all clinical parameters (Table 2). Mean HbA1c decreased from 7.7% ± 1.71% to 6.55% ± 1.13% (P < 0.001), with consistent reductions across both HbA1c subgroups up to 6.23% ± 1.01% for HbA1c ≤7.5 and 6.93% ± 1.1% for HbA1c > 7.5. Systolic and diastolic blood pressure improved significantly, from 125.6 ± 14.9 mmHg to 119.5 ± 12.9 mmHg (P < 0.001) and 79.5 ± 10.5 mmHg to 75.3 ± 7.7 mmHg (P < 0.001), respectively. Lipid profiles showed favorable changes, including reductions in total cholesterol (174 ± 45.6 mg/dL to 154 ± 42 mg/dL, P < 0.001) and LDL (112.4 ± 39.1 mg/dL to 93.2 ± 37.8 mg/dL, P < 0.001), and an increase in HDL (44.4 ± 9.83 mg/dL to 47.4 ± 11.23 mg/dL, P < 0.001). Triglycerides also decreased significantly (150 [114.4–225.7] to 118.7 [83.9–181.4], P < 0.001). Inflammatory markers improved, with CRP declining from 0.23 [0.12–0.43] to 0.14 [0.07–0.31] (P < 0.001). Anthropometric measures showed significant reductions in BMI (30.1 ± 5.51 to 28.2 ± 4.62, P < 0.001) and waist circumference (102.6 ± 13.1 cm to 97.6 ± 11.2 cm, P < 0.001).
Clinical Parameters at Baseline vs. 12 Months, Overall and Based on Starting HbA1c at Baseline (n = 208)
The P values <0.05 indicate the statistical significance of paired sample t-test and Wilcoxon signed rank test.
HbA1c trends over 12 months
Figure 1 represents the reduction in mean HbA1c (%) over 12 months, stratified by baseline HbA1c levels (≤7.5% and >7.5%) and the overall cohort. The overall mean HbA1c decreased significantly from 7.71% (7.47, 7.94) to 6.54% (6.39, 6.7), with consistent improvement over time. Patients with baseline HbA1c >7.5% experienced the largest reduction, from 9.18% (8.89, 9.48) to 6.93% (6.69, 7.17), with the steepest decline in the first 3 months. Patients with baseline HbA1c ≤7.5% showed a smaller, gradual reduction from 6.52% (6.39, 6.64) to 6.23% (6.04, 6.42) over the same period.

Unadjusted mean and 95% confidence intervals for HbA1c (%) overall and stratified by HbA1c at baseline (≤7.5% vs. >7.5%).
Medication profile trends over 12 months
Figure 2 illustrates the trends in medication combinations used by patients over 12 months. At baseline, GIP/GLP-1 (n = 57) and GLP-1 (n = 56) were the most frequently used monotherapy. Over time, there was a notable shift toward the increased use of advanced therapies, particularly GIP/GLP-1 receptor agonists, which rose significantly to become the most frequently used combination by 12 months (n = 69). At baseline, 8 subjects relied solely on insulin. Concurrently, the use of insulin decreased by half.

Upset plot showing the combination of the medication used by the patients at each visit.
At baseline, the most frequently used medications were GIP/GLP-1 and GLP-1 agonists. However, by the 12-month follow-up, this trend shifted to GIP/GLP-1 agonists and oral hypoglycemic agents. A trend was observed in the use of the combination therapy of GIP/GLP-1 agonists and insulin, which was utilized by 7 subjects at baseline, decreased to 5 subjects at 6 months, and further to 4 subjects at 12 months.
Figure 3 illustrates the relationship between changes in HbA1c levels and changes in medication costs over the study period. In the HbA1c > 7.5% group, a clear trend is observed where decreases in HbA1c levels are associated with corresponding reductions in medication costs. Conversely, in the HbA1c ≤ 7.5% group, most data points are concentrated around zero change in HbA1c, indicating stable glycemic control. However, this group exhibits substantial variability in cost changes along the y-axis, suggesting that despite stable glycemic control, intervention intensity, and medication adjustments contributed to fluctuating costs. Notably, both groups present outliers, with some individuals experiencing extreme positive changes in costs, likely due to individualized therapeutic adjustments or additional health care interventions required over the course of treatment.
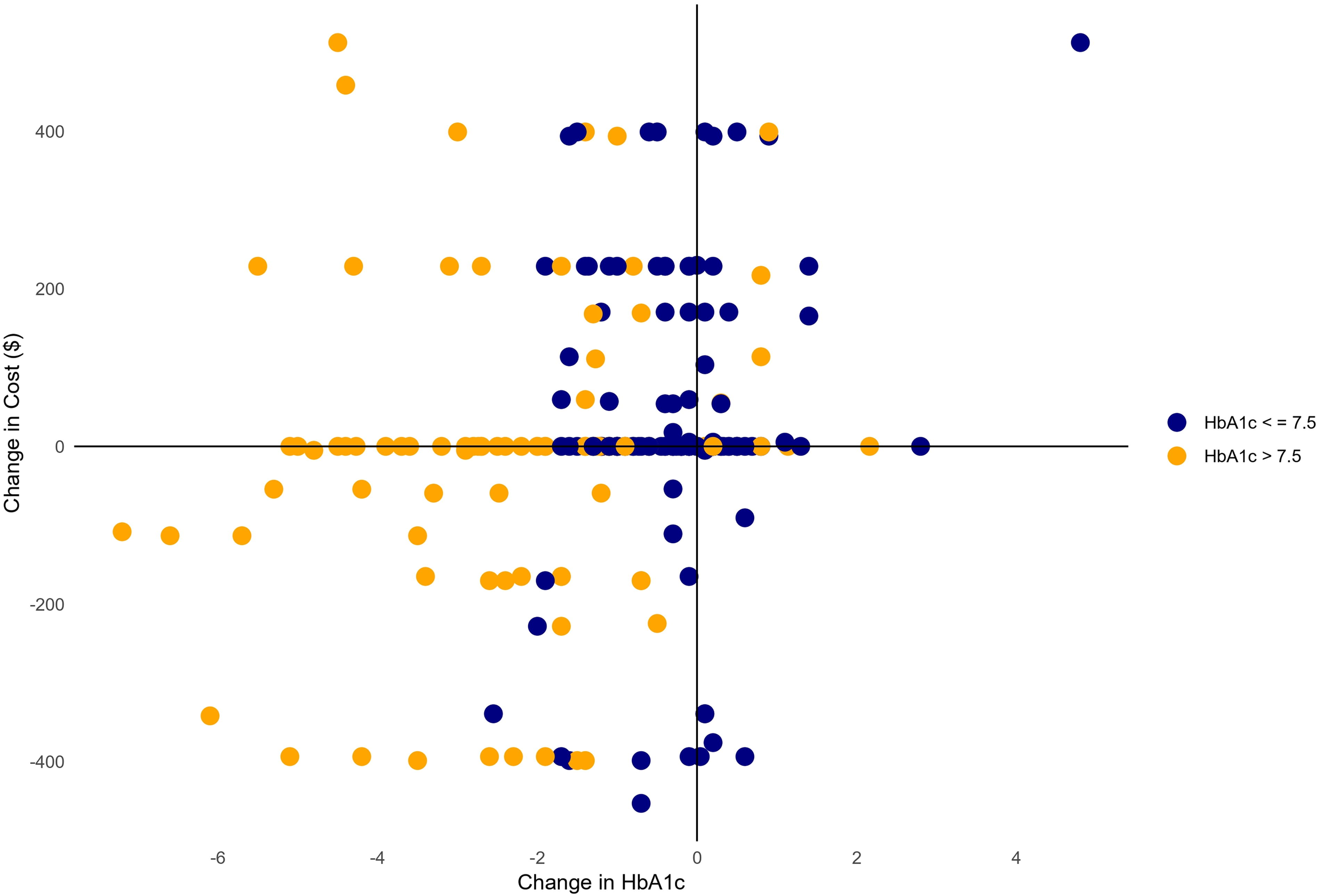
Change in HbA1c vs. Change in Cost ($). The costs were converted from UAE Dirhams to U.S. dollars using the official conversion rate of US$ (1 USD = 3.67 AED).
Discussion
Results from this retrospective cohort study reveal that patients managed under the GluCare hybrid care model achieved statistically significant and clinically meaningful improvements in glycemic control, lipid profiles, blood pressure, and anthropometric measures over a 12-month period. Patients with baseline HbA1c >7.5% demonstrated the greatest glycemic improvement, with a reduction of 1.61% points (from 9.18% to 7.57%, P < 0.001), indicating that the hybrid care model could potentially be a solution for these patients considering they were already diagnosed and being treated via traditional, episodic care. This decline occurred primarily within the first 3 months of the intervention, highlighting the model’s rapid impact on poorly controlled diabetes, with sustained improvements over the subsequent 9 months. While engagement levels vary and have previously been highlighted, the authors believe a critical factor for this improvement is due to the introduction of new structured lifestyle modifications provided to patients as standard, and centered around digital bio-marker tracking and the data insight-feedback loop, as the majority of patients did not have access to continuous feedback, a multidisciplinary team, education, or wearables before introducing them to the hybrid care model. 13 These limitations exist with all UAE health care providers that typically follow episodic care and focus only on services that are reimbursable. The results are consistent with studies by Greenwood et al., who highlighted that patients with higher HbA1c levels tend to experience larger reductions when supported by technology-enabled diabetes self-management education. 16 Improved glycemic control has also been linked to reduced health care costs, with a 1% reduction in HbA1c associated with a 13% decrease in diabetes-related expenses and annual cost savings of up to $736 per patient. 17 Patients with baseline HbA1c ≤7.5% maintained stable glycemic control, with a modest reduction from 6.52% to 6.18% (P < 0.001), demonstrating the program’s effectiveness in supporting glycemic stability, which is often challenging in diabetes management.
One of the standout findings of this study is that a significant proportion of patients managed under the hybrid care model achieved HbA1c levels under the target threshold of 7%, highlighting the effectiveness of combining in-clinic care with remote monitoring and personalized interventions. This outcome contrasts with findings from digital-only diabetes self-management education and support (DSMES) programs, where patients with poor baseline glycemic control often experience less substantial reductions. A recent study evaluating a DSMES program showed HbA1c improvements, limited to patients with baseline HbA1c >8%, where HbA1c was improved from 9.48% to 7.47% at 12 months. 18 These results underscore the added value of hybrid models in achieving glycemic targets, particularly for patients requiring more intensive and personalized interventions.
In addition to these findings, the well-controlled group (HbA1c ≤ 7.5%) offers valuable insights into the impact of the GluCare model’s intensive RCDM and behavioral change components. Despite most of these patients being on established medications, the hybrid care approach appears to enhance glycemic stability further through tailored lifestyle modifications, continuous monitoring, and patient engagement strategies. This highlights how an integrated model of care can support even those already on effective treatment regimens, providing an added layer of benefit beyond pharmacological interventions.
Long-term reductions in HbA1c are clinically significant as they are associated with decreased risks of diabetes-related complications, including microvascular and macrovascular events.19,20 Studies indicate that a 1% decrease in HbA1c corresponds to a 37% reduction in microvascular complications and a 14% reduction in myocardial infarction risk. 21 In our study, the association of medication use with HbA1c levels further substantiates these findings. GIP/GLP-1 receptor agonists were significantly more prevalent in the HbA1c >7.5% group compared with those with HbA1c ≤7.5%, while insulin use also showed a significant disparity (16.1% vs. 4.3%). This is especially important to demonstrate efforts to use only more expensive GIP/GLP-1 for poorly controlled patients. These results suggest that the reduction in insulin use and the concurrent rise in GIP/GLP-1 receptor agonist prescriptions align with targeted management strategies aimed at optimizing glycemic control.
Significant reductions in systolic (−6.1 mmHg) and diastolic blood pressure (−4.2 mmHg) in this study reflect the hybrid model’s effectiveness in addressing cardiovascular risk factors. These findings align with the results of Hou et al. (2018), who reported similar reductions in blood pressure with mobile health interventions combined with pharmacological management. 7 Improvements in lipid profiles, including reductions in total cholesterol (−20 mg/dL) and LDL (−19.2 mg/dL), alongside an increase in HDL (+3 mg/dL), further demonstrate the comprehensive impact. Addressing lipid parameters is crucial, as effective lipid management has been shown to reduce the risk of atherosclerotic cardiovascular disease, a leading cause of mortality in T2D patients. 20 By improving these metrics, the GluCare model not only enhances patient outcomes but also contributes to long-term cost savings by preventing macrovascular complications.
The reductions in BMI (−1.9 kg/m2) and waist circumference (−5 cm) observed in our study are noteworthy. Previous studies, such as the systematic review by Debon et al., have highlighted that mobile health interventions generally result in BMI reductions of 0.5–1.2 kg/m2, suggesting that the GluCare hybrid model outperforms many digital-only interventions due to its combination of in-clinic behavioral support and continuous data monitoring. 6 Weight loss not only improves insulin sensitivity and glycemic control but also reduces mechanical stress on weight-bearing joints, potentially lowering the risk of osteoarthritis and its associated health care costs. 22
Synergistic benefits and cost implications
The collective improvements in glycemic control, lipid profiles, blood pressure, and weight observed in this study underscore the synergistic benefits of comprehensive diabetes care. These metrics are interrelated; for example, improved lipid profiles and blood pressure directly reduce cardiovascular risk, while glycemic control and weight loss enhance insulin sensitivity and reduce medication requirements. The American Diabetes Association highlights that addressing multiple cardiovascular risk factors yields significant reductions in morbidity and mortality. 20 In addition, by reducing the risk of complications, hybrid care models such as GluCare can lower health care costs, making them a cost-effective solution for managing chronic diseases. 17 The integration of wearable devices and mobile applications distinguishes the GluCare model from conventional care and other hybrid models. By monitoring sleep, heart rate variability, and physical activity, these devices provide insights into lifestyle factors that influence glycemic control. Ashrafzadeh and Hamdy emphasized the growing role of technology in identifying patterns in patient behavior that may impact diabetes management, a concept supported by our study’s outcomes. 12 Findings show that the GluCare model not only improved clinical outcomes but also reduced health care costs. Our analysis revealed that transitioning more patients from an uncontrolled to a controlled state resulted in a total cost reduction of $23,485 over 12 months based on the expected cost in the UAE for diabetes. 23 As more patients improved glycemic control, they moved into the controlled category ($2,282 per patient/year), effectively reducing the higher cost burden associated with uncontrolled diabetes. If the 93 patients who were initially uncontrolled had remained unmanaged, their total cost would have remained at $510,461, meaning the intervention saved at least $23,485 in one year. These annual cost estimates ($2,282 for controlled and $2,667 for uncontrolled patients) are based on UAE-specific health care cost data from a previously published study. 23 The implications of long-term cost savings are even more significant. Using UAE health care cost data and literature-based multipliers for diabetes-related complications, we projected 5-year and 10-year costs for patients who remained uncontrolled. 24 Over a 5-year period, the cost for patients developing microvascular complications (e.g., retinopathy, kidney disease) would increase to $545,668, a 2.2-fold increase from baseline costs. If these patients remained uncontrolled for 10 years and developed macrovascular complications (e.g., heart attacks, strokes), the projected cost would rise significantly to $1,587,398 (6.4 times the baseline cost). In a worst-case scenario, where patients developed both microvascular and macrovascular complications, the 10-year cost would escalate to $2,331,491, a 9.4-fold increase. The estimated long term cost saving is illustrated in Figure 4. The observed cost savings and improved clinical outcomes support a shift toward performance-based health care reimbursement models rather than traditional fee-for-service models. Since all components of RCDM (wearables, remote monitoring, digital tools, and personalized behavior change) were provided at no additional cost to patients or payors, these findings suggest that adopting a hybrid model can lead to both better health outcomes and significantly reduced long-term health care expenditure. Future models could entail payors sharing a portion of the cost savings with hybrid care providers as an incentive to provide the out-of-clinic engagement model.

Projected Health care Costs Over 10 Years: No GC Intervention vs. GC Intervention.
Strengths and limitations
A major strength of this study is the real-world evidence generated through the use of standardized outcome measures (ICHOM) and the integration of advanced technologies. However, the retrospective design and single-center setting may limit the generalizability of findings. In addition, while the study demonstrates significant improvements in clinical outcomes, further research is needed to explore patient satisfaction and the cost-effectiveness of the hybrid model in diverse health care settings. A potential limitation of the study is the effect of unequal sample sizes across the monthly measurements. While this variability might introduce some bias, the matching of baseline and 12-month samples provides a robust basis for interpreting the observed reduction as true.
The results of this study highlight the potential of hybrid care models to revolutionize T2D management by combining digital and in-clinic elements to deliver patient-centered care. The significant improvements in glycemic control, cardiovascular health, and adherence underscore the importance of leveraging technology to enhance patient engagement and outcomes. The hybrid model also achieves subsequent lowering of overall medication cost as a result of de-escalation of polypharmacy and improved results. The ICHOM standards further ensure that patient-reported outcomes are integrated into care delivery, promoting a holistic approach to diabetes management.
Conclusions and Future Implications
The GluCare hybrid care model demonstrated significant improvements in glycemic control, weight, blood pressure, and lipid profiles over 12 months, in addition to lowered overall medication cost. Approximately 72.6% of patients achieved target HbA1c levels under 7%, with those starting with poor glycemic control showing the greatest reductions. Even patients who were classified as well controlled showed improvements, highlighting the result of the additional effectiveness of the behavioral change component of the hybrid care model. These findings highlight the model’s effectiveness in integrating in-clinic care with real-time remote monitoring and wearable technology to sustain engagement and deliver personalized care.
The estimated cost analysis revealed substantial financial benefits, with an annual cost reduction of $23,485 achieved within the first year by transitioning more patients from uncontrolled to controlled diabetes. Long-term projections indicate that maintaining glycemic control could prevent significant cost increases associated with diabetes complications, which could escalate up to 9.4 times the baseline cost over a decade if unmanaged. Since all components of the RCDM were provided at no additional cost to patients or payors, these results support the shift toward performance-based reimbursement models.
Future research should explore randomized controlled trials to confirm causality, assess long-term impacts on diabetes-related complications, and evaluate cost-effectiveness. Expanding the model across diverse populations and health care settings, along with fostering collaborations with larger systems, can enhance care coordination and clinical outcomes. The GluCare model presents a scalable solution for transforming chronic disease management by combining technology with patient-centered care while demonstrating measurable cost savings for health care systems.
Footnotes
Authors’ Contributions
Conceptualization: H.Z., I.A., Methodology: H.Z., G.P. Validation: H.Z. Formal Analysis: H.Z., G.P. Investigation: H.Z., G.P. Resources: A.K. Data Curation: H.Z., G.P. Writing—Original Draft: H.Z. Writing—Review and Editing: M.C., A.A., A.H., I.A. Visualization: H.Z. Supervision: H.Z.
Author Disclosure Statement
The following authors declared the following potential conflicts of interest: The following authors are full-time employees/interns at GluCare: H.Z., G.P., M.C., A.K., A.A., A.H., and I.A.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.