
Abstract
Background:
Vitamin D has been proposed as a potential modulator of diabetic foot ulcer (DFU) risk and healing due to its immunomodulatory and wound-healing properties. However, its independent role in DFU pathogenesis and ulcer outcomes remains unclear.
Methods:
This case–control, observational study included 960 patients attending a tertiary diabetic foot care clinic, of which 727 were included comprising 526 patients with DFU and 201 without DFU (non-DFU control). Serum 25-hydroxyvitamin D [25(OH)D] levels obtained at presentation were quantified and categorized into deficiency (<20 ng/mL) or absence of deficiency (>20 ng/mL), followed by subgroup analysis (severe deficiency, <12 ng/mL; deficiency, 12–20 ng/mL; insufficiency, 20–30 ng/mL; sufficiency, >30 ng/mL). Logistic regression assessed the independent association of 25(OH)D levels with DFU occurrence, adjusting for body mass index, duration of diabetes, glycated hemoglobin, retinopathy, neuropathy, and coronary artery disease (CAD)/cerebrovascular accident (CVA). Kaplan–Meier and Cox regression analyses were performed for DFU healing and long-term outcomes.
Results:
Median serum 25(OH)D levels were significantly lower in the DFU group than in the non-DFU group (20.1 ng/mL vs. 25.4 ng/mL, P < 0.001). Logistic regression revealed no significant association between 25(OH)D levels and DFU occurrence (odds ratio [OR] = 1.01, P = 0.280). In contrast, neuropathy (OR = 23.1, P < 0.001), CAD/CVA (OR = 8.40, P < 0.001), and retinopathy (OR = 2.76, P = 0.001) emerged as the strongest significant predictors. Serum 25(OH)D levels were not associated with DFU severity (P = 0.860) or healing (Kaplan–Meier, P = 0.43). Cox regression confirmed no significant predictors of healing outcomes, including serum 25(OH)D levels (P = 0.719).
Conclusions:
Vitamin D deficiency is prevalent in patients with DFU, but it does not corelates with occurrence, severity, or healing of foot ulcer in people with diabetes. The presence of neuropathy, retinopathy, and coronay artery disease are stronger predictors of DFU risk. These findings highlight the multifactorial nature of DFU pathogenesis and underscore the need for a multidisciplinary management approach.
Introduction
Diabetic foot ulcers (DFUs) represent a major clinical and economic challenge globally and are among the most common causes of hospital admission in patients with diabetes mellitus, accounting for 32% of all hospitalizations in this population. 1 DFU also causes excess morbidity due to the risk of amputation and mortality. 2 Vitamin D, a steroid hormone crucial for calcium homeostasis and bone metabolism, has gained attention for its potential immunomodulatory and wound-healing properties.2,3 Multiple studies have reported an association between vitamin D deficiency and the occurrence of diabetic foot ulcers,4–7 although conflicting results have also been noted. 8 The proposed mechanism underlying this association involves increased inflammatory cytokines in patients with vitamin D deficiency, which may contribute to ulcer formation. 9 Furthermore, studies have observed increased severity of DFUs in patients with vitamin D deficiency. 6 Additionally, a randomized controlled trial and a meta-analysis have demonstrated that cholecalciferol supplementation improves wound healing in DFU.10,11 The mechanism proposed involves the increased expression of cathelicidin, an antimicrobial peptide, by vitamin D metabolites. 12
Despite these findings, there remains a lack of data on whether the association between vitamin D deficiency, DFU, and their outcomes is independent of confounding factors, such as neuropathy, nephropathy, retinopathy, and coexisting macrovascular complications. We conducted this study to address this gap by analyzing the data from patients attending a specialized diabetic foot care clinic at a tertiary care hospital. This study evaluates the association between serum 25(OH)D levels and various clinical aspects of DFUs, including their occurrence, severity, and healing rates.
Methods
Study design and setting
This retrospective, case–control, observational study was conducted at a tertiary care diabetic foot clinic, reviewing the records of patients who attended the clinic between January 2017 and December 2024. Ethical approval for the study was obtained from the institutional ethics committee.
Study population
Patients aged 18 years or older with a diagnosis of diabetes mellitus and attending the diabetic foot clinic of a tertiary care hospital were included in the study. A total of 960 patients’ data were reviewed, and 727 patients with all relevant outcome details were included. The cohort was divided into two groups: those with DFU (DFU group, n = 526) and those without foot ulcers (non-DFU group, n = 201), having visited the clinic for other complaints such as diabetic neuropathy or Charcot’s foot. Demographic, clinical, and laboratory data were extracted from electronic medical records. Information collected included age, sex, duration of diabetes, body mass index (BMI), glycated hemoglobin (HbA1c), and the presence of comorbidities such as peripheral neuropathy, nephropathy, retinopathy, peripheral arterial disease (PAD), coronary artery disease (CAD), and relevant ulcer details including depth of the ulcer graded as modified Wagner’s grade. The diagnosis of comorbidities was based on the existing American Diabetes Association (ADA) guidelines. Standard ulcer treatment was provided to all the patients as per prevailing guidelines including ulcer debridement, antibiotics for infected DFU, wound dressing, and appropriate offloading. Serum 25(OH)D was quantified using an electrochemiluminescence assay (COBAS 8000, Roche Diagnostics, Germany) with a coefficient of variation of 6%–8%. Serum 25(OH)D levels were categorized into deficiency (<20 ng/mL) and absence of deficiency (>20 ng/mL) according to Endocrine Society guidelines. 13 Further subgroup analysis classified levels as severe deficiency (<12 ng/mL), deficiency (12–20 ng/mL), insufficiency (20–30 ng/mL), and sufficiency (>30 ng/mL).
Statistical analysis
Descriptive statistics were used to summarize the demographic and clinical characteristics of the study population. Data were assessed for normality using the Shapiro–Wilk test. Normally distributed continuous variables were expressed as mean ± standard deviation (SD), while non-normally distributed variables were presented as median with interquartile range (IQR). Differences between groups were analyzed using chi-square tests for categorical variables and independent t-tests or Mann–Whitney U tests for continuous variables, as appropriate. Kaplan–Meier survival curves and log-rank tests were used to evaluate the association between vitamin D status and DFU healing time. Cox proportional hazards regression was performed to adjust for potential confounders, including age, sex, HbA1c, BMI, and comorbidities. A P value <0.05 was considered statistically significant. All analyses were conducted using SPSS version 29 (IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics
A total of 727 patients were included in the study, comprising 526 patients with DFU (DFU group) and 201 without DFU (non-DFU group). The baseline characteristics are presented in Table 1, which demonstrates significant differences between the two groups. The median serum 25(OH)D levels were significantly lower in the DFU group compared with the non-DFU group (P < 0.001), as illustrated in Figure 1.
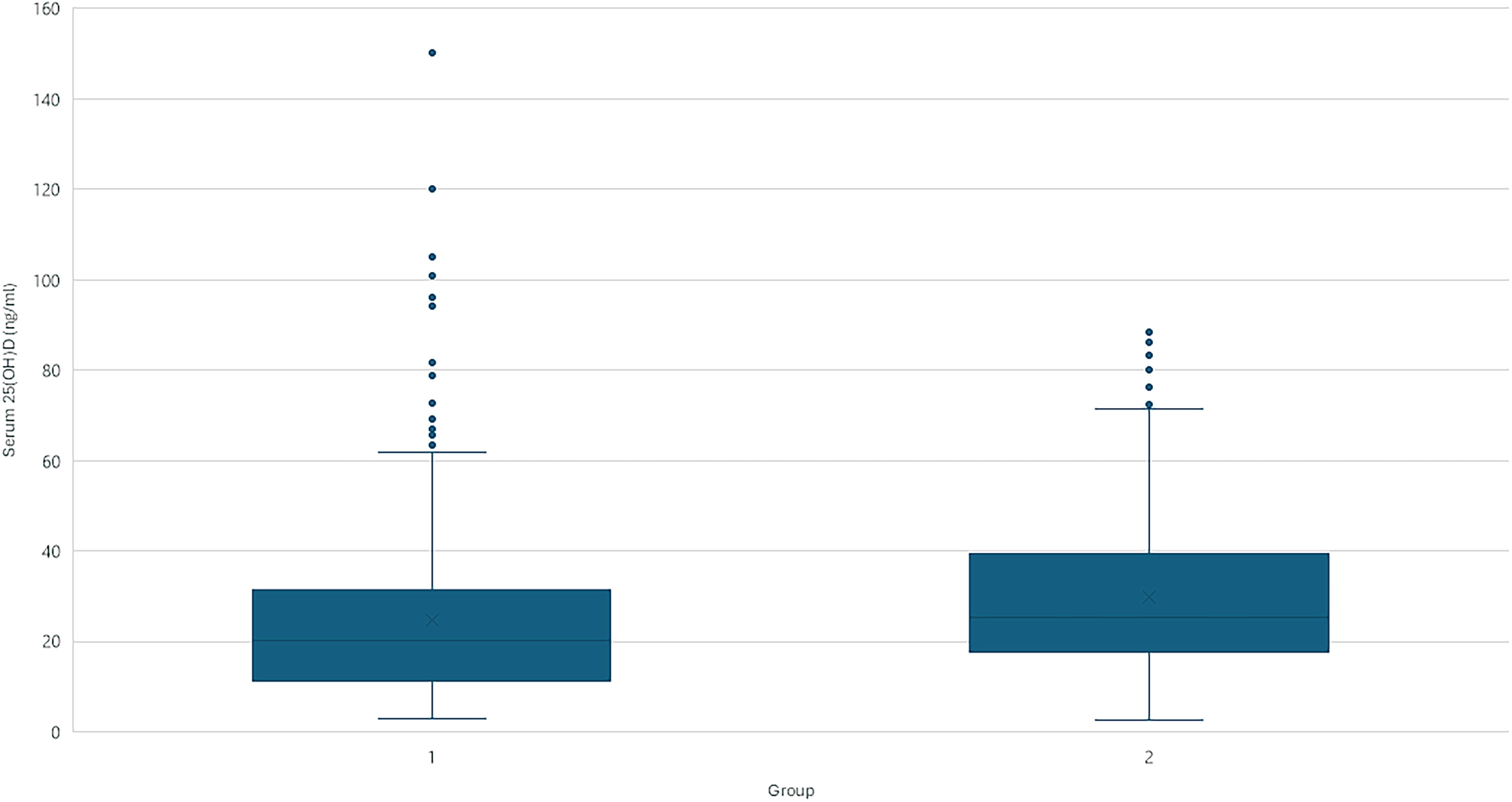
Serum 25(OH)D levels in patients with DFU and without DFU. 25(OH)D3, 25-hydroxyvitamin D3; DFU, diabetic foot ulcer.
Baseline Characteristics of Patients in Group 1 (Patients with DFU) and Group 2 (Non-DFU Patients)
25(OH)D, 25-hydroxyvitamin D3; BMI, body mass index; HbA1c, glycated hemoglobin.
DFU occurrence
A significantly higher proportion of patients had vitamin D deficiency in the DFU group compared with the non-DFU group (P < 0.001). Subgroup analysis revealed significant differences in serum 25(OH)D levels across the categories of deficiency: severe deficiency (<12 ng/mL), deficiency (12–20 ng/mL), insufficiency (20–30 ng/mL), and sufficiency (>30 ng/mL), as presented in Supplementary Table S1.
Logistic regression analysis demonstrated that serum 25(OH)D levels were not a significant predictor of DFU occurrence (odds ratio [OR] = 1.01 [0.99–1.02], P = 0.280). The analysis identified neuropathy (OR = 23.1, P < 0.001), coronary artery disease (CAD)/cerebrovascular accident (CVA) (OR = 8.40, P < 0.001), retinopathy (OR = 2.76, P = 0.001), and male sex (OR = 1.96, P = 0.009) as significant predictors of DFU occurrence. Age, higher BMI, and PAD were also associated with increased odds of DFU occurrence, as shown in Table 2.
Logistic Regression Analysis of Predictors for Diabetic Foot Ulcer Occurrence
25VIT(OD)D3, serum 25-hydroxyvitamin D; B, regression coefficient; CAD/CVA, coronary artery disease/cerebrovascular accident; CI, confidence interval; OR, odds ratio; P, P value; PAD, peripheral arterial disease; SE, standard error.
DFU severity
Serum 25(OH)D levels were not associated with ulcer depth as measured by the modified Wagner grading (P = 0.860). Kruskal–Wallis tests revealed no significant differences in serum 25(OH)D levels across the Wagner grade categories, as depicted in Figure 2.

Serum 25(OH)D levels across different Wagner grades in patients with DFU.
DFU healing time
Kaplan–Meier survival analysis indicated no significant differences in healing times between groups with vitamin D deficiency and those without (P = 0.43). Median healing times were 16 weeks (2–26 weeks) in either group, irrespective of vitamin D deficiency status, as shown in Figure 3.
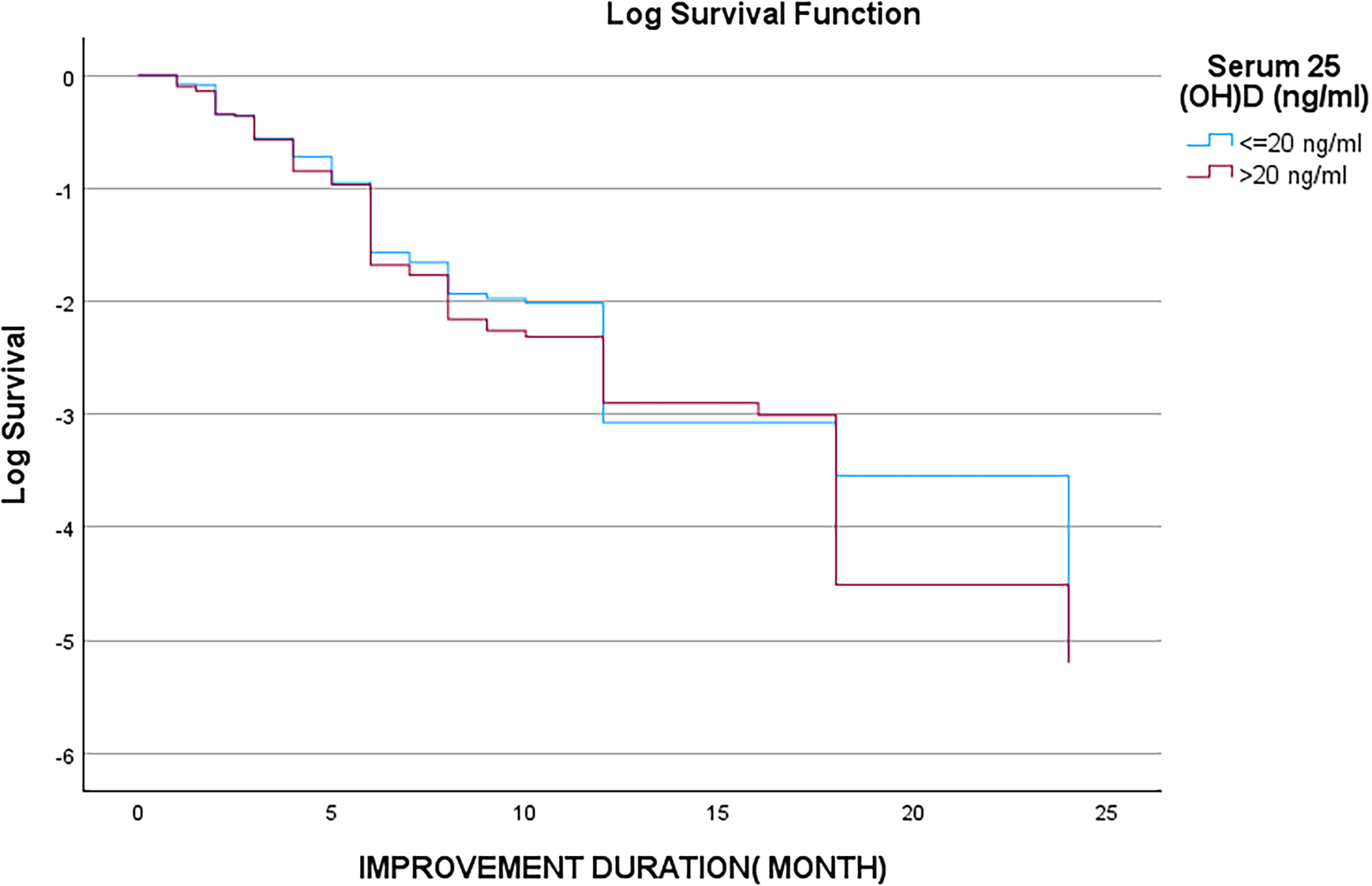
Log survival function of improvement duration in patients with DFU based on serum 25(OH)D Levels.
Final outcomes
Cox proportional hazards regression confirmed that variables such as serum 25(OH)D levels (P = 0.719), age (P = 0.776), HbA1c (P = 0.672), retinopathy (P = 0.813), neuropathy (P = 0.918), PAD (P = 0.379), CAD/CVA (P = 0.801), and duration of diabetes (P = 0.326) were not significant predictors of DFU healing. Similarly, Wagner grade (P = 0.341), BMI (P = 0.476), and creatinine levels (P = 0.471) did not significantly affect healing outcomes, as outlined in Supplementary Table S2.
Table 3 provides a summary of key findings from prior research alongside the results of our study.
Summary of Findings from Previous Studies and Current Analysis
DFU, diabetic foot ulcer; DM, diabetes mellitus; T2DM, type 2 diabetes mellitus.
Discussion
This study provides a comprehensive evaluation of the association between serum 25(OH)D levels and various outcomes in patients with DFU. Despite the theoretical and mechanistic evidence supporting the role of vitamin D in immune function and wound healing, our findings suggest that vitamin D deficiency does not independently predict the occurrence, severity, or healing of DFUs.
The key findings of the present analysis include significantly lower median serum 25(OH)D levels in the DFU group compared with the non-DFU group (20.1 ng/mL vs. 25.4 ng/mL), no significant association between vitamin D levels and DFU severity (P = 0.860), and no differences in healing times across vitamin D status (P = 0.719). Instead, neuropathy, CAD/CVA, and retinopathy emerged as significant predictors of DFU occurrence. The findings of this study suggest a limited utility of serum 25(OH)D levels as a biomarker for DFU risk and outcomes. While vitamin D deficiency is prevalent among patients with DFUs, its role appears to be overshadowed by other confounding variables that are directly related to ulcer pathogenesis in people with diabetes.
Consistent with previous studies, such as Zubair et al. and Tiwari et al., our study found significantly lower serum 25(OH)D levels in patients with DFUs compared with those without.4,5 However, our logistic regression analysis demonstrated that this association was not independent of covariates. In contrast to the meta-analysis from Li et al., which reported an overall association between vitamin D deficiency and DFUs, our findings highlight the complex interplay of other factors such as neuropathy, CAD/CVA, and retinopathy, which emerged as stronger predictors of DFU occurrence. 7 The inverse association between HbA1c and DFUs in our study likely reflects the tertiary care referral bias, and patients with DFUs may have glycemic optimization before presentation to us. The prominent role of neuropathy, PAD, and vascular complications including CAD and CVA further emphasizes the systemic burden of diabetes-related complications in the pathogenesis of DFU.14,15
Our findings indicate no significant association between serum 25(OH)D levels and ulcer severity. However, they contrast with Feldkamp et al., which observed an inverse correlation between vitamin D levels and ulcer severity (Armstrong grade). 6 The discrepancy may arise from differences in study design, including our adjustment for confounders such as neuropathy and PAD, as well as the larger sample size in our study. These findings suggest that while vitamin D may have some indirect effects on wound modulation, factors such as infection, vascular supply, duration of wound, and local tissue status are more critical determinants of ulcer severity. 2
Our study found no significant association between serum 25(OH)D levels and healing or outcomes such as amputation or death, as determined by Kaplan–Meier survival analysis and Cox regression. These results differ from Razzaghi et al. and Kinesya et al., which demonstrated a beneficial role of vitamin D supplementation in wound healing and ulcer size reduction.10,11 The lack of significant predictors in our study may reflect the advanced disease stages managed in a tertiary care setting, where systemic complications and delayed presentations limit the potential for biochemical markers like vitamin D to influence healing outcomes. The nonsignificant relationship between serum 25(OH)D levels and final outcomes, such as amputation or death, further supports the notion that vitamin D may not be a primary driver of clinical outcomes in DFUs. Furthermore, this underscores the need for a holistic management approach targeting multiple systemic factors rather than focusing solely on serum 25(OH)D levels. Previous studies examining the role of vitamin D deficiency in DFUs have yielded mixed results.
The strengths of our study include its large sample size, the use of a standardized assay for vitamin D measurement, and rigorous adjustment for key confounding variables. Additionally, the study provides a detailed assessment of vitamin D levels across a spectrum of DFU-related outcomes, including occurrence, severity, and healing. However, the retrospective design introduces inherent limitations, such as potential selection bias and reliance on single-point vitamin D measurements, which do not capture temporal variations. Furthermore, the single-center nature of the study may limit the generalizability of findings to broader populations. Future prospective studies and randomized controlled trials are warranted to further elucidate the role of vitamin D as a potential adjunctive therapy in select populations.
Conclusions
In conclusion, while serum 25(OH)D levels were significantly lower in patients with DFUs, they did not independently predict ulcer occurrence, severity, or healing outcomes after accounting for confounding factors. Our findings reinforce the multifactorial nature of DFU pathogenesis, with comorbidities playing pivotal roles in ulcer development. These results emphasize the importance of a multidisciplinary approach addressing vascular, metabolic, and neurological complications in DFU management.
Footnotes
Acknowledgment
The authors sincerely thank Miss Reshma for data entry.
Authors’ Contributions
R. Shah contributed to investigation, visualization, and writing—original draft. R. Singh performed data curation and formal analysis. A.R. contributed to conceptualization, project administration, validation, supervision of the study, and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.