
Abstract
Background:
Uptake of exercise in people with type 1 diabetes (T1D) is low despite significant health benefits. Fear of hypoglycemia is the main barrier to exercise. Continuous glucose monitoring (CGM) with predictive alarms warning of impending hypoglycemia may improve self-management of diabetes around exercise.
Aim:
To assess the impact of Dexcom G6 real-time CGM system with a predictive hypoglycemia alert function on the frequency, duration, and severity of hypoglycemia occurring during and after regular (≥150 min/week) physical activity in people with T1D.
Methods:
After 10 days of blinded run-in (Baseline), CGM was unblinded and participants randomized 1:1 to have the “urgent low soon” (ULS) alert switched “on” or “off” for 40 days. Participants then switched alerts “off” or “on,” respectively, for a further 40 days. Physical activity, and carbohydrate and insulin doses were recorded.
Results:
Twenty-four participants (8 men, 16 women) were randomized. There was no difference in change from baseline of hypoglycemia <3.0 and <3.9 mmol/L with the ULS on or off during the 24 h after exercise. With ULS alert “on” time spent below 2.8 mmol/L compared with baseline was significantly (P = 0.04) lower than with ULS “off” in the 24 h after exercise. In mixed effects regression, timing of the exercise and baseline HbA1c independently affected risk of hypoglycemia during exercise; exercise timing also affected hypoglycemia risk after exercise.
Conclusion:
A CGM device with an ULS alert reduces exposure to hypoglycemia below 2.8 mmol/L overall and in the 24 h after exercise compared with a threshold alert.
Background
The World Health Organization (WHO) recommends that adults 18–64 years of age undertake at least 150 min of moderate-intensity aerobic physical activity or at least 75 min of vigorous-intensity aerobic physical activity per week as well as muscle-strengthening activities on two or more days per week. 1 The exercise recommendations are the same for people with type 1 diabetes (T1D). 2
Physical activity improves HbA1c, cardiovascular risk, dyslipidemia, hypertension, and reduces body mass index and risk of early death. 3 –6 Despite these benefits, uptake of exercise by those with T1D is low, with 67% undertaking no physical activity. 7,8 Fear of hypoglycemia is the main barrier preventing people with T1D from exercising. 9 Hypoglycemia is common during and after exercise. 10,11 The symptoms of hypoglycemia can mimic those that occur routinely during exercise, leading to difficulties identifying hypoglycemia.
The impact of exercise on blood glucose is influenced by multiple factors, including type of exercise, intensity, timing, duration, circulating insulin (insulin on board), insulin modality (multiple daily injections [MDI] or continuous subcutaneous insulin infusion [CSII]), pre-exercise glucose level, glucose variability before exercise, glycogen stores, previous hypoglycemia, and aerobic fitness 12 –14
Aerobic exercise, such as walking, running, and swimming, predominantly relies on hepatic and muscle glycogen, with an increasing reliance on fat oxidation and circulating glucose as exercise continues. 14 Aerobic exercise therefore tends to result in a drop in blood glucose levels in people with T1D unless insulin on board is reduced or carbohydrate is consumed. People with T1D commonly become hypoglycemic within around 45 min of commencing aerobic exercise, dependent on baseline glucose. 10,15
High-intensity exercise often has a different effect on blood glucose due to changes in how fuel is metabolized and because of the stimulation of counter regulatory hormones often resulting in an increase in blood glucose. 16 Resistance exercise, that is strength training such as lifting weights, tends to result in less glucose variability than aerobic exercise, and in combination with aerobic exercise can be particularly useful for people with T1D, as the counterregulatory hormones secreted during resistance exercise reduce glucose disposal during aerobic exercise. 14 The benefits of resistance exercise in the general population are well documented. 17 The benefits in T1D are less clear, however it is known that diabetes is an independent risk factor for low muscular strength 18 which can be improved by resistance training. 19
Late hypoglycemia, particularly nocturnal hypoglycemia, is of concern in T1D, especially if the exercise has been undertaken in the late afternoon or evening. 14 While the glucose disposal associated with exercise stops soon after the exercise stops, increased insulin sensitivity associated with physical activity persists for at least 24 h. 14,20 Adequate carbohydrate intake to promote replenishment of glycogen, as well as reduced insulin on board are essential to prevent hypoglycemia, although limited research means that the optimal strategy is yet to be fully identified. 14
Continuous glucose monitoring (CGM) systems measure glucose in the interstitial fluid every 1–15 min, providing the users with continuous feedback of the level and trend of their blood glucose. The use of CGM has increased dramatically and become an essential part of diabetes management for many people. An “Urgent Low Soon” (ULS) alert, present on the Dexcom G6 and G7 devices, alerts when the system predicts that the sensor glucose will be ≤3.1 mmol/L in the next 20 min. In a review of 15,000 anonymized records of people with T1D using the Dexcom G6 device there was a significant difference in hypoglycemia between those with the predictive alert on and those with the alert off, regardless of screen views, reducing their time spent in hypoglycemia by >36%. 21
The use of CGM during exercise is less well-studied than in the general T1D population, however, could support optimized exercise for people with T1D by addressing fear and occurrence of hypoglycemia. Limited evidence means clinical advice on the use of CGM in exercise relies heavily on a consensus statement. 22
As measured by percentage mean or median absolute relative difference (%MARD), the accuracy of CGM during exercise has been shown to be worse, due to multiple physiological changes that occur in exercise that alter the glucose interstitial fluid dynamic, resulting in a longer lag time from the glucose in venous blood. 23 This is despite improvement in the accuracy of sensors overall in the last 30 years. 24
The Physical Acitivity, CGM & Exercise (PACE) study aimed to assess the impact of a ULS alert on frequency, duration, and severity of hypoglycemia during and after exercise in people with T1D, and to investigate the dominant factors associated with hypoglycemia during and after exercise.
Methods
Consort reporting guidelines were adhered to throughout.
25
Ethics approval was received from the London-Westminster NRES committee and the study was registered in the
Adults over 18 years of age with T1D (confirmed based on clinical features) using a multiple dose insulin injection regimen or insulin pump for >6 months were recruited from Imperial College Healthcare NHS Trust outpatient clinics and screened and enrolled by a research dietitian. Participants had received structured diabetes self-management education and were undertaking regular exercise in line with the WHO exercise guidelines. Remote recruitment was used during the COVID-19 pandemic and the inclusion criteria were changed so that all new participants were under 40 years of age and had diabetes for <10 years, to eliminate the need for a screening ECG.
Exclusion criteria included pregnant or planning pregnancy, breastfeeding, being enrolled in other clinical trials, active malignancy or under investigation for malignancy, severe visual impairment, reduced manual dexterity, and being unable to participate due to other factors, as assessed by the Chief Investigator.
The study design was a randomized crossover study, which included a blinded phase to collect baseline data, and two intervention phases, as shown in Figure 1.
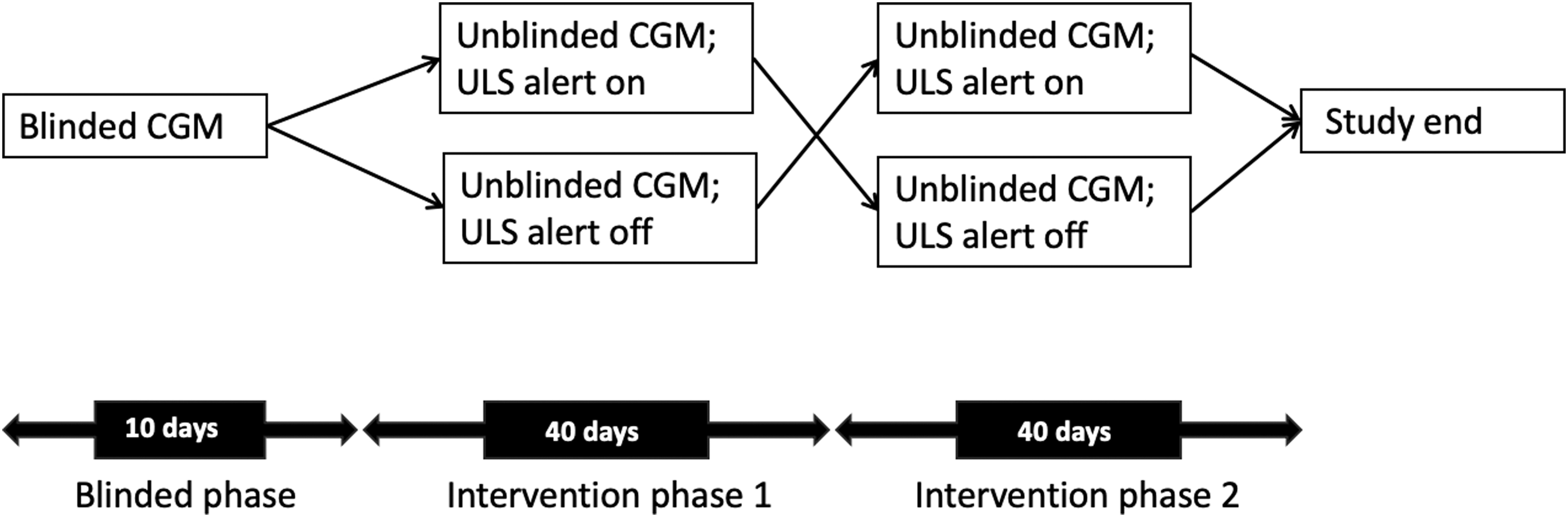
Study design of the PACE study indicating a blinded phase of CGM and two intervention phases with the ULS alert on or off. CGM, continuous glucose monitoring; PACE, Physical Activity, CGM & Exercise; ULS, “Urgent low soon.”
Participants wore a GPS-enabled sports watch with built-in heart rate monitor (Garmin Forerunner 935; Garmin Ltd, Kansas) for the entire duration of the study. Recording all activities of 15 min or longer, participants chose from a list of 20 preloaded activities in the Garmin software closest to the activity they were undertaking (or other if needed). Participants recorded their carbohydrate intake and insulin doses throughout the study either in their insulin pumps, or using the MySugr app (MySugr, Vienna, Austria) if using MDI. Participants made all insulin dosing decisions as usual, based on their prestudy insulin:carbohydrate ratios. A structured education refresher focusing on carbohydrate counting; hypoglycemia avoidance; recognition; and management, insulin action, and the theory and practicalities of CGM was provided.
Participants used the Dexcom G6 CGM system (Dexcom, San Diego, CA) throughout the study. The baseline phase of the study required participants to undertake blinded CGM. At the end of the blinded phase, unblinded Dexcom G6 was used on a smartphone. During the first 40-day intervention phase, half the participants had the ULS alert turned on and the other half had it turned off. They switched for the second intervention phase. Participants were randomized 1:1 using Sealed Envelope (Sealed Envelope Ltd, London, United Kingdom). Threshold glucose alerts were set at 4.4 mmol/L, with the option to reduce this to 4.0 mmol/L after 2 weeks. Participants used the same threshold alert for the same amount of time in the two intervention phases.
To assess changes in quality of life during the study, Hypoglycemia Fear Survey-II (HFS-II), Gold hypoglycemia awareness score and the Diabetes Distress Score 17 (DDS17) questionnaires, which assess fear of hypoglycemia, hypoglycemia awareness, and diabetes distress were measured at the start, after the first intervention, and at the end of the study.
CGM data from all participants with complete (>70% of time) data throughout the study were collected. One participant was excluded from the primary analysis as they did not have baseline data. CGM recorded in the 12 and 24 h after exercise were collated into separate data sets. The percentage time spent below 3.9, 3.0, and 2.8 mmol/L during baseline, 40 days with alert on and 40 days with alert off were calculated, and then the change from baseline was calculated and analyzed. A Wilcoxon signed-rank test was used to analyze the between-group differences in change from baseline time spent below thresholds measured throughout the study period, in the 12 and 24 h after exercise.
The primary outcome was the time spent below 3.0 mmol/L in the 12 h after exercise. Secondary outcomes included time below 3.9 and 2.8 mmol/L in the 12 and 24 h after exercise. Although we nominate a primary hypothesis, the study design invited a range of investigations and secondary analysis significances were not corrected for multiple comparisons. Secondary analyses were, instead, treated as hypothesis generating and as guides to interpretation. A power calculation was undertaken that indicated 20 participants, would demonstrate as significant at P < 0.05 and with 80% power a mean difference in time in hypoglycemia between predictive hypoglycemia alert on and off of 0.45 standard deviations or more. 26
In a secondary analysis, CGM for each exercise and the post exercise period were collected and were coded according to whether or not an episode of hypoglycemia <3.9, <3.0, or <2.8 mmol/L occurred. A mixed effects logistic regression with participant identity number as grouping variable was used to assess associations between hypoglycemia occurrence at the different thresholds (dependent variable: 0 = no hypoglycemia occurred, and 1 = hypoglycemia occurred) and variables that might influence risk of hypoglycemia. Potential predictors of hypoglycemia that were explored included: Insulin modality (CSII or MDI) Age of participant (years) Duration Diabetes (years) Baseline HbA1c (mmol/mol) Sex of participant (Male or Female) Predictive hypoglycemia alert (on or off) Exercise timing (morning/afternoon/evening/night) Duration of activity in minutes Maximum heart rate reported as percentage maximum heart rate (i.e., adjusted for age) Activity type (19 categories) Whether the activity occurs within 12 h of the previous activity (Yes or No)
Due to varying numbers of activities provided by different participants, univariate mixed effects modeling was undertaken to identify the variables that were significant univariate predictors (P < 0.05) for hypoglycemia. These variables were then selected for multivariable mixed effects modeling. Each analysis was undertaken twice, once with hypoglycemia defined as a single reading below threshold, and once where hypoglycemia was defined as three consecutive readings below threshold. This article reports on the results from the single reading analysis.
Results
In total, 32 participants were recruited between December 2019 and April 2021. Two were excluded at screening. One person dropped out due to a serious adverse event unrelated to the study. Five people dropped out when the study was restarted after the COVID lockdown and the study design was altered to virtual study visits (Fig. 2). The study ended when the last participant finished the study in July 2021. Twenty-four people with T1D (16 women) on MDI 13 or CSII 11 who exercised regularly (150 min/week or more) completed this randomized, within-subject crossover study. Eight participants were using intermittently scanned CGM, 5 were using real-time CGM, and 11 were not using CGM of any kind. None was using hybrid closed loop. Their demographics are shown in Table 1.
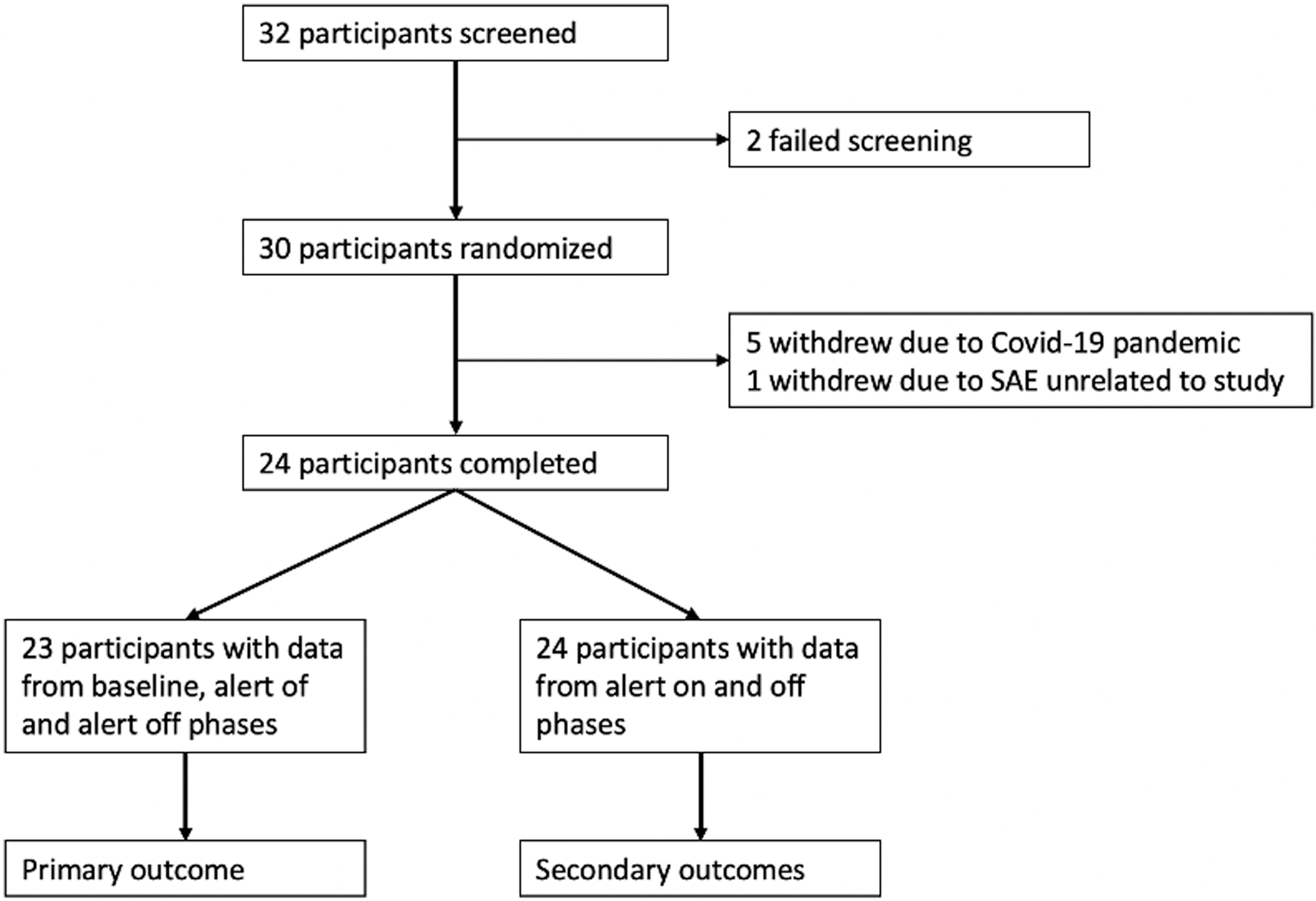
Consort diagram of PACE study. SAE, serious adverse event.
Participant Demographics
SD, standard deviation.
One person was excluded from the primary analysis due to incomplete data.
A total of 1746 activities greater or equal to 30 min were undertaken, of which 130 (7%) resulted in a reading of <3.9 mmol/L during activity, 572 (33%) resulted in a reading of <3.9 mmol/L in the 12 h after activity, and 781 (45%) resulted in a reading of <3.9 mmol/L in the 24 h after activity. A reading <3.0 mmol/L occurred during 47 (3%) of activities, 212 (28%) in the 12 h after, and 305 (17%) in the 24 h after activity. A reading <2.8 mmol/L occurred in 31 (2%) of activities and 139 (8%) and 218 (12%) in the 12 and 24 h after exercise.
Impact of ULS through the duration of the study
Analysis of between-group differences in change from baseline time spent below thresholds measured throughout the baseline and intervention periods (i.e., irrespective of exercise) showed that compared with baseline, participants spent less time at level 2 hypoglycemia (<3.0 mmol/L) when the predictive hypoglycemia alert was switched on than switched off, as shown in Table 2.
Percentage Time Below Hypoglycemia Thresholds and Change in Percentage Time with Urgent Low Soon Alert on and Alert Off (Median [IQR) at Baseline and During the 24 and 12 H After Commencement of Exercise
Bold represents a statistically significant finding where p < 0.05.
ULS, urgent low soon.
Impact of ULS alert in the 12 h postexercise
In the 12 h after exercise, the median percentage time spent below 3.9, 3.0, and 2.8 mmol/L during baseline, was (median [IQR]) 3.480 [0.595, 8.102], 0.464 [0.000, 1.842], and 0.117 [0.000–0.921]%. The change from baseline in the 40 days with the ULS alert on at 3.9 mmol/L was −0.373 [−3.924, 0.284] and with ULS off −0.750 [−3.866, 0.137]%. The equivalent figures for a threshold of 3.0 mmol/L were, −0.301 [−1.237, 0.000] and 0.00 [−1.468, 0.161] and with 2.8 mmol/L 0.000 [−0.828, 1.100] and 0.000 [−0.734, 0.188]%. However, despite a trend toward lower median times in hypoglycemia with ULS on, there were no significant between-group differences.
Impact of ULS alert in the 24 h postexercise
As shown in Table 2, there was a between-group difference in the change from baseline of time spent below 2.8 mmol/L with the ULS switched on, compared with switched off, favoring the alert on (P = 0.03). There was no significant difference for the hypoglycemia threshold of 3.0 and 3.9 mmol/L.
Secondary analysis—factors influencing hypoglycemia during and after activity
A total of 1746 activities were analyzed, of which 772 activities (44%) were walking, 323 (18%) were “indoor cardio” assumed to be gym-based aerobic activities (such as using the ski ergometer, treadmill, or exercise bike), 225 (13%) were cycling, 148 were running (8%), and 64 (4%) were yoga. Eighteen activities were recorded by the participants as “other.” The remaining 91 (5%) activities were small numbers of a range of activity types, and therefore combined for ease of analysis, and referred to as “smaller groups combined.”
Associations between factors that might influence hypoglycemia and episodes of hypoglycemia were very similar regardless of whether hypoglycemia was based on a single CGM hypoglycemia reading or on three consecutive readings.
Hypoglycemia during exercise
There were a total of 130 hypoglycemic events of 3.9 mmol/L or below during exercise, which equates to 7% of activities. Forty-seven of those activities reached 3 mmol/L or less and 31 reached 2.8 mmol/L, equating to 3% and 2% of activities, respectively.
In mixed effects regression analysis, increasing baseline HbA1c was associated with increased risk of hypoglycemia <3.9 mmol/L during exercise (odds ratio [OR] 1.042 confidence interval [CI] 1.002–1.083; P = 0.041). Exercising in the afternoon or evening was associated with an increased risk of hypoglycemia <3.9 mmol/L during exercise compared with exercising in the morning (afternoon OR 3.353 [CI 1.978–5.684] P < 0.001) (evening OR 2.285 [CI 1.224–4.265] P = 0.009). Increasing duration of exercise was associated with an increase in risk of hypoglycemia (OR 1.013 [CI 1.008–1.019] P < 0.001). Undertaking “indoor cardio” exercise was associated with a lower risk of hypoglycemia compared with walking (indoor cardio OR 0.298 [95% CI 0.119–0.747] P = 0.010). A higher maximum heart rate was also associated with the risk of hypoglycemia during exercise (OR 1.032 [95% CI 1.006–1.059] P = 0.015) (Fig. 3).
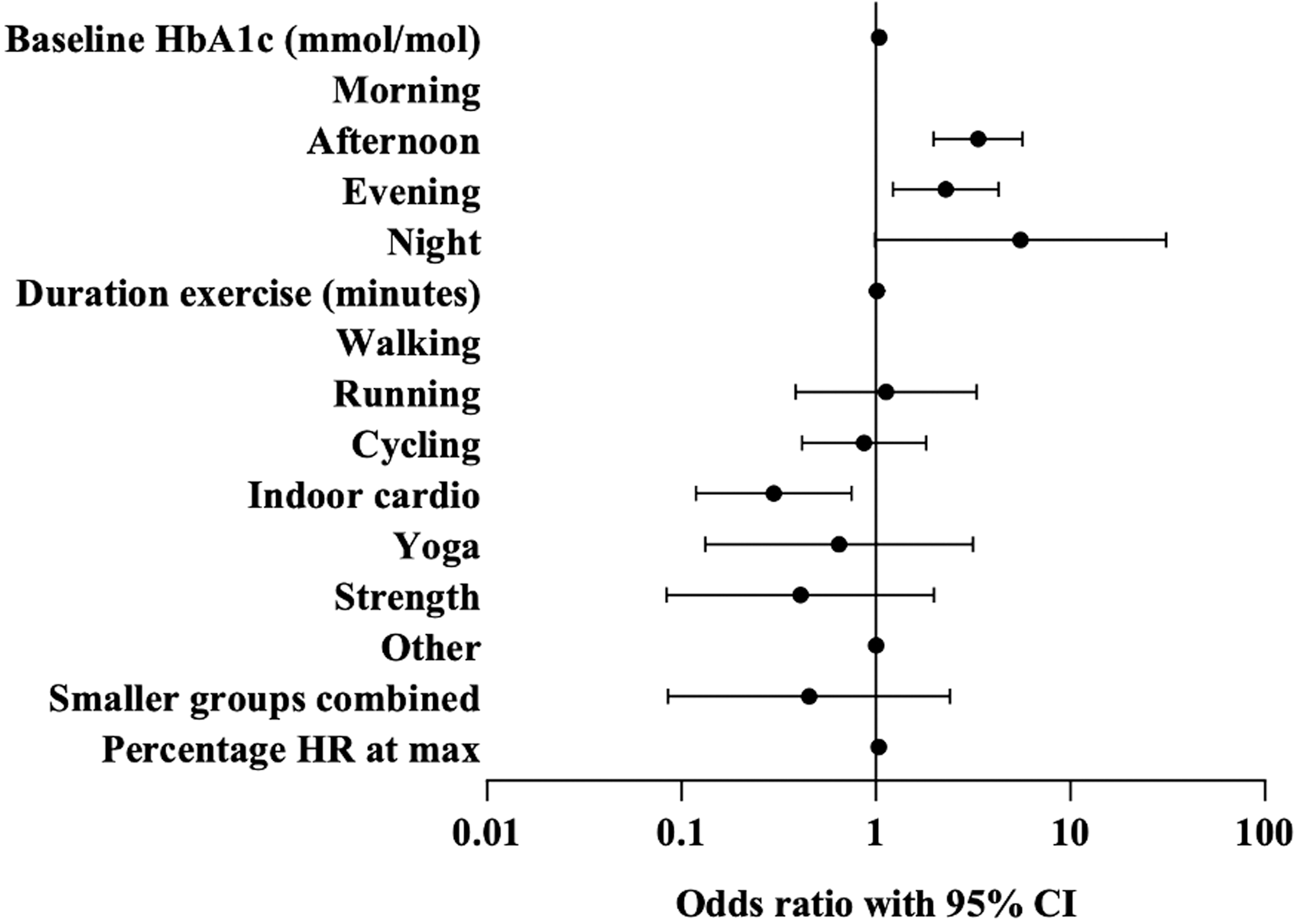
Forest plot showing odds ratios (logarithmic scale) from a mixed effects analysis of variables interacting with a single reading <3.9 mmol/L during activity accounting for participant ID. Morning was defined as exercise between 0600–1200, afternoon 1200–1700, evening was 1700–2300 and night 2300–0600. CI, confidence interval; HR, heart rate; ID, identity number.
Baseline HbA1c, afternoon exercise and exercise duration also increase the risk of hypoglycemia <3.0 mmo/L during exercise (OR 1.077 [1.026–1.130] [P = 0.003], 2.266 [1.030–4.984] [P = 0.042], and 1.010 [1.004–1.017] [P = 0.001], respectively). Only exercise duration increased the risk of hypoglycemia <2.8 mmol/L (OR 1.008 [1.001–1.015] P = 0.019)
Hypoglycemia in the 12 h after exercise
There were a total of 572 hypoglycemic events of 3.9 mmol/L or below in the 12 h after exercise, which equates to 33% of activities. Two hundred and twelve of those activities reached 3 mmol/L or less and 139 reached 2.8 mmol/L, equating to 28% and 8% of activities. respectively.
A mixed effects analysis of the associations of exercise timing, activity type, and percentage maximum heart rate with risk of hypoglycemia <3.9 mmol/L in the 12 h after exercise found that exercising at night significantly increased the risk of experiencing hypoglycemia in the next 12 h (OR 6.877 [CI 1.705–48.548] P = 0.10) (Supplementary Fig. S1).
For risk of hypoglycemia <3.0 mmol/L in the 12 h after exercise, a mixed effects analysis of the impact of exercise timing, type, maximum heart rate, and prior exercise found that exercising at night was associated with a significantly increased risk of hypoglycemia, as well as running compared with walking (OR 2.834 [1.234–6.508] P = 0.014). Risk of hypoglycemia was significantly lower if it was not performed within 12 h of the previous exercise (OR 0.612 [0.386–0.968] P = 0.036). Night-time exercise and running compared with walking also increased the risk of hypoglycemia <2.8 mmol/L in the 12 h after exercise (OR 5.890 [1.360–25.504] P = 0.018 and 3.197 [1.463–6.990] P = 0.004, respectively).
Hypoglycemia in the 24 h after exercise
There were a total of 781 hypoglycemic events of 3.9 mmol/L or below in the 24 h after exercise, which equates to 45% of activities. Three hundred and five of those activities were associated with hypoglycemia of 3 mmol/L or less and 218 with 2.8 mmol/L or less, equating to 17% and 12% of activities, respectively.
A mixed effects analysis of the impact of timing, type, and maximum heart rate on the risk of hypoglycemia <3.9 mmol/L in the 24 h after exercise showed that exercising at night significantly increased the risk of hypoglycemia in the following 24 h compared with exercising in the morning (OR 9.269 [1.048–82.008] P = 0.045). Cycling was associated with a higher risk compared with walking (OR 1.826 [1.064–3.135] P = 0.029) (Supplementary Fig. S2).
Exercising at night and “other” type of exercise were associated with increased risk of hypoglycemia <3.0 mmol/L (OR 13.058 [2.649–64.374] P = 0.002 and 5.880 [1.068–32.359] P = 0.042, respectively) and <2.8 mmol/L (OR 7.464 [1.717–32.456] P = 0.007 and OR 9.216 [1.356–62.649] P = 0.023) in the 24 h after exercise.
Quality of life
From a total of 24 participants, 17 had complete questionnaire data at baseline, at the end of the ULS on phase and the end of the ULS off phase. The mean (standard deviation [SD]) baseline Gold score was 2.4 (SD 0.8), DDS-17 was 1.8 (SD 0.7), and HFS-II 32.8 (SD 13.1). Wilcoxon signed-rank test indicated no significant difference in change in quality of life from baseline with alert on compared with alert off.
Discussion
The participants in this study undertook exercise regularly, with baseline glucose already close to target and low time spent in hypoglycemia at baseline. Despite this, a CGM device with an ULS alert reduced exposure to hypoglycemia below 2.8 mmol/L in the 24 h after exercise compared with a threshold alert set at 4.4 or 4.0 mmol/L. This is in line with previous work, which analyzed a large, unselected population of patients who switched from Dexcom G5 (with no ULS alert) to G6 using the ULS alert and found that the alert resulted in reduced hypoglycemia independent of screen views. 27 However, our study was undertaken in and around exercise, during which %MARD has been shown to be higher, therefore reducing reliability since we did not ask participants to confirm CGM hypoglycemia with capillary blood glucose testing.
We found no statistically significant difference in hypoglycemia with ULS on or off in the 12 h after activity, perhaps because of insufficient study power or postexercise behaviors such as eating carbohydrate, but the significant difference noted in the 24 h after exercise and across the whole study suggests that an ULS alert could be particularly useful in minimizing delayed postexercise hypoglycemia. Another factor that could have impacted the significance of our findings was that the threshold alerts were set at either 4.0 or 4.4 mmol/L depending on participant preference, which may be higher than some CGM users choose. Threshold alerts set at a lower level may have increased the dependence on the ULS alert, therefore increasing the difference in the groups with it on and off.
A high proportion of activities (45%) were affected by hypoglycemia <3.9 mmol/L in the following 24 h. Many factors impact hypoglycemia unrelated to exercise, however this is a high frequency of hypoglycemia in a population with a relatively low percentage time spent in hypoglycemia (a median of 1.90% in the total 90 days of the study [IQR 0.93–4.75]).
We found that a higher baseline HbA1c was associated with a higher risk of hypoglycemia during exercise, in contrast to the often-cited phenomenon of higher hypoglycemia risk at lower HbA1c values. This may reflect greater glycemic variability and more insulin correction boluses used by people with higher HbA1c values. We found that increasing duration of exercise is associated with an increased risk of hypoglycemia at all thresholds during exercise, which could be explained by depleted glycogen stores and/or potentially insufficient reduction of insulin before exercise.
Exercising in the morning was associated with the lowest risk of hypoglycemia during exercise, possibly reflecting the higher insulin resistance from counter-regulatory hormones at that time. There were only 13 night-time exercise sessions recorded, with 6 participants contributing data. However, all but 1 of the 13 sessions was associated with hypoglycemia. Consequently, CIs were wide, but night exercise was associated with a high, significant OR for hypoglycemia.
When the risk of individual variables was analyzed, cycling regularly appeared as having a significant effect, however, when put into a model with other significant variables, it lost significance while duration maintained significance, indicating that it is the duration of cycling that may increase the risk of hypoglycemia and not the cycling per se.
There were far fewer statistically significant factors impacting the risk of hypoglycemia <2.8 mmol/L, likely reflecting the lower number of hypoglycemia episodes recorded at this level.
The signal from analyses looking at a single CGM hypoglycemia reading, and three consecutive readings were similar. While national guidelines recommend hypoglycemia being defined as 15 min in duration, during exercise, hypoglycemia can be recognized promptly by CGM, and resolved quickly to enable exercise to continue. Sports drinks and gels have a high glycemic index, so glucose is absorbed into the bloodstream quickly providing an effective treatment for hypoglycemia. It is, therefore, possible that people with T1D who are proactively monitoring their glucose levels to prevent or treat hypoglycemia, may spend <15 min in hypoglycemia.
The participants in this study all had low Gold scores and hypoglycemia fear at baseline. This may have an impact on the lack of significant results from the quality of life (QOL) analysis or may reflect the low number of completed questionnaires. The adaptation of the study design because of the COVID-19 pandemic meant that visits were undertaken remotely, which made it more difficult to gather physical questionnaires and equipment but further research exploring person-reported outcomes is important.
Conclusion
An ULS alert is an important tool to prevent biochemically important hypoglycemia in the 24 h after exercise. Timing and type of exercise impact the risk of developing hypoglycemia during and after exercise and warrant further research to maximize the advice provided to people with T1D undertaking exercise.
Footnotes
Acknowledgments
The authors would like to thank the participants of this study for their time and effort. This study was run with approval and support from NIHR Imperial Clinical Research Facility. Infrastructure support was provided by the NIHR Imperial Biomedical Research Center.
Authors' Contributions
S.R.: Methodology, formal analysis, investigation, formal analysis, data curation, writing—original draft, visualization, and project administration. N.O.: Conceptualization, methodology, formal analysis, resources, writing—review and editing, and supervision. I.G.: methodology, formal analysis, and writing—review and editing. M.T.: project administration. B.T.: Data curation. N.H.: Conceptualization, methodology, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
N.O. has received research support from Dexcom and Roche Diabetes; has participated in advisory groups for Dexcom, Medtronic, and Roche Diabetes; and has received fees for speaking from Dexcom, Tandem, and Roche Diabetes. N.H. has received research support from Dexcom. S.R., I.G., M.T., and B.T. have nothing to disclose.
Funding Information
This investigator-led study was funded by Dexcom OUS-2018-024.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.